
Abstract
Purpose:
To compare postoperative pain levels and postoperative morbidity between patients who underwent extraperitoneal laparoscopic radical prostatectomy (EPLRP) concomitant hernia repair and patients who underwent only EPLRP, by matched-pair analyses.
Methods:
From December 2003 to December 2012, 54 patients who underwent EPLRP with simultaneous hernia repair were categorized as group 1. Their postoperative pain levels were quantitatively compared with those of 54 patients who underwent only EPLRP (group 2), in matched-pair analyses, including age, body mass index, and American Society of Anesthesiologists scoring. Preoperative tumor characteristics, operative and postoperative data were recorded. Pain levels were evaluated by using the visual analog scale (VAS) scoring, every day, during the first postoperative week. Statistical analyses were performed.
Results:
Mean follow-up was 21 months. Mean age was 65±0.5 years. Preoperative, perioperative, and postoperative data were similar in the two groups. Group 1 needed a mean of 9.17 mg and group 2 needed a mean of 8.06 mg morphine derivative analgesic (piritramide) postoperatively. Total mean VAS scores were 5.65 and 4.98, in group 1 and group 2, respectively (P=0.06). Moreover, there was no significant difference between groups for complications.
Conclusion:
Simultaneous hernia repair does not affect pain levels after EPLRP. The procedure also does not result in prolongation of operative time and does not increase complication rates.
Introduction
L
Laparoscopic inguinal hernia repair has become popular for the management of inguinal indirect and/or direct hernia. 7 Two methods have been described for repairing inguinal hernia laparoscopically—the transabdominal preperitoneal patch (TAPP) and the totally extraperitoneal patch (TEP). Although both techniques have been reported safe and effective, TEP is more popular than TAPP. The TEP procedure has lower recurrence and complication rates and less postoperative analgesic requirements than TEPP. 8
It has been well established that hernia repair during LRP 9 –11 or RALP 12 is safe and feasible. According to our best knowledge, however, there have been no published data on simultaneous hernia repair during LRP with special attention to the pain levels in the postoperative period.
We aimed to assess the postoperative pain levels of cases of extraperitoneal LRP (EPLRP) and concomitant hernia repair cases during the first postoperative week. To the best of our knowledge, this is the first study in the literature that EPLRP and concomitant inguinal hernia repairs were assessed for postoperative pain levels.
Methods
All patients fully understood the treatment and aim of this study. Written informed consents were obtained from all patients. The data were recorded prospectively using a Microsoft Office Excel spreadsheet. This study has been a part of ongoing LRP studies in our department. The present study was a retrospective analysis of a prospectively collected database. Between December 2003 and December 2012, 2246 LRPs were performed. Exclusion criteria were previous inguinal hernia repair, bilateral inguinal hernia repair, and allergy to narcotic analgesics. The patients found to have bilateral inguinal hernias were excluded from the study to accurately compare pain status and pain-curve progress during the first postoperative week.
Data collection
We used age (year), body mass index (BMI) (kg/m2), and American Society of Anesthesiologists (ASA) scores for matched pair criteria to define postoperative pain scores accurately. There were 54 patients who had simultaneous unilateral indirect inguinal hernia repair during EPLRP. These patients were Group 1. According to the matched pair analyses, there were 54 patients without simultaneous hernia repair. They patients were Group 2.
Demographic data included age, BMI, ASA score, prostate-specific antigen (PSA) (ng/mL) level, Gleason score, and clinical stage. The operative data included estimated blood loss (EBL, mL), operative time (minutes); postoperative data included hospital stay, amount of used narcotic analgesic (mg) (piritramide), and visual analog pain scale (VAS) scores. VAS scoring was recorded during the first postoperative week independently by urologists during the morning visits.
Surgical procedures
We used the ascending extraperitoneal Heilbronn technique for LRP in all operations in the present series. 3,4 After the Retzius space was prepared, the operation continued step by step as incision of endopelvic fascia, dissection of prostatic apex, urethral division, posterior dissections and preserving neurovascular bundles, incision of bladder neck, dissection of vesicula seminalis and vasa deferentia, and division of prostatic pedicles. Urethrovesical anastomosis was performed by the van Velthoven continuous suturing technique. Pelvic lymph node dissections were performed in patients with a PSA level >10 ng/mL and/or a Gleason score >6. Tumor-Node-Metastasis classification was used for determining clinical stage. 13
The exact diagnosis of inguinal hernia was performed mainly before the operation, except for two cases of hernia diagnosed intraoperatively. A polypropylene 6×11 cm mesh (Prolene™ Mesh, Ethicon Endo-Surgery, Johnson & Johnson, Inc.) was used for hernia repairs.
Hernia repair technique
Simultaneous hernia repair did not alter the initial steps of the procedure. The extraperitoneal space was created under direct vision by a 10-mm balloon dilating trocar (Herloon, Braun, Aesculap AG, Tuttlingen, Germany). The bilateral epigastric vessels and the pubic bone arch are the main landmarks when creating extraperitoneal space. Then, the first 10-mm trocar was inserted. A 30-degree telescope was used, and the ports were placed under direct endoscopic view after establishment of the extraperitoneal space (12 mm Hg, high flow). After the epigastric vessels were identified, the dissections were performed in a lateral and cranial direction to prepare the space for the trocar placements. In this step, the peritoneum was gently pushed away using an endoscopic peanut. Two 10-mm trocars were placed at the lateral pararectal lines, about 4 cm below the umbilicus, and two 5 mm in the left and right lower quadrants at the horizontal level of the navel. Thereafter, the hernia defect and sac were identified. The hernia sac was reduced stepwise with particular care of the cord structures. We avoided an excessive coagulation during the preparation to avoid a possible thermal injury to the cord structures such as lymphatic vessels and the testicular artery. The testicular vessels, vas deferens, and peritoneum were separated and the space behind these structures was created.
The LRP with pelvic lymphadenectomy were performed as described above, briefly. 4 After accomplishing the urethrovesical anastomosis and using the same trocar constellation, a 6×11 cm polypropylene mesh was introduced through the 10-mm trocar to cover the internal inguinal ring and posterior wall of the inguinal canal. A pelvic drain was placed in the contralateral side, and carbon dioxide was released under direct vision (Fig. 1). This surgical technique (TEP) was similar to the technique described by Felix and associates. 8

Endoscopic view of extraperitoneal hernia repair during extraperitoneal laparoscopic radical prostatectomy. (
There were technical challenges in some cases. Attachments in the inguinal cord and/or adhesions of the inguinal cord with the peritoneum were dissected step by step carefully. During the dissections, we avoided excessive coagulation around the cord structures, especially lymph vessels of the inguinal cord, to prevent thermal injury and to not cause a hydrocele or an orchitis postoperatively. In addition, testicular vessels, especially the testicular artery, were prepared very carefully. After demonstrating the accurate anatomy of inguinal structures and peritoneum, the polypropylene mesh was placed properly.
Cystography was performed in all patients 7 days after the operation. If no leak was demonstrated, the urethral catheter was removed. All of the complications were classified according to modified Clavien classifications. 14
Statistical analyses
The Statistical Package for the Social Sciences (SPSS) for Windows 16.0 (SPSS Inc., Chicago, IL) was used for statistical analysis. The independent-samples t test was used to compare measurable values, and the Mann–Whitney U test was used for comparisons between the groups. Statistical significance was accepted at P<0.05.
Results
Mean age was 65±0.5 years. Mean follow-up was 21 months. There were 54 patients in group 1 and 54 patients in group 2. The demographic and preoperative data of groups are summarized in Table 1.
N.A.=not assessed; BMI=body mass index, PSA=prostate-specific antigen; ASA=Amerian Society of Anesthesiologists.
Mean operative time, EBL, and hospital stay were similar in the groups (respectively, P=0.83, P=0.79, P=0.69) (Table 2).
EBL=estimated blood loss.
Group 1 needed mean 9.17 mg and group 2 needed mean 8.06 mg morphine derivative analgesic after operation; total mean VAS scores were 5.65 and 4.98, respectively (P=0.06) (Table 3). Moreover, there was no significant differences between the groups for complications.
VAS=visual analog scale.
The VAS scores decreased day by day, as shown in Figure 2. Inguinal hernias were mainly diagnosed preoperatively and were an incidental intraoperative finding only in two patients.
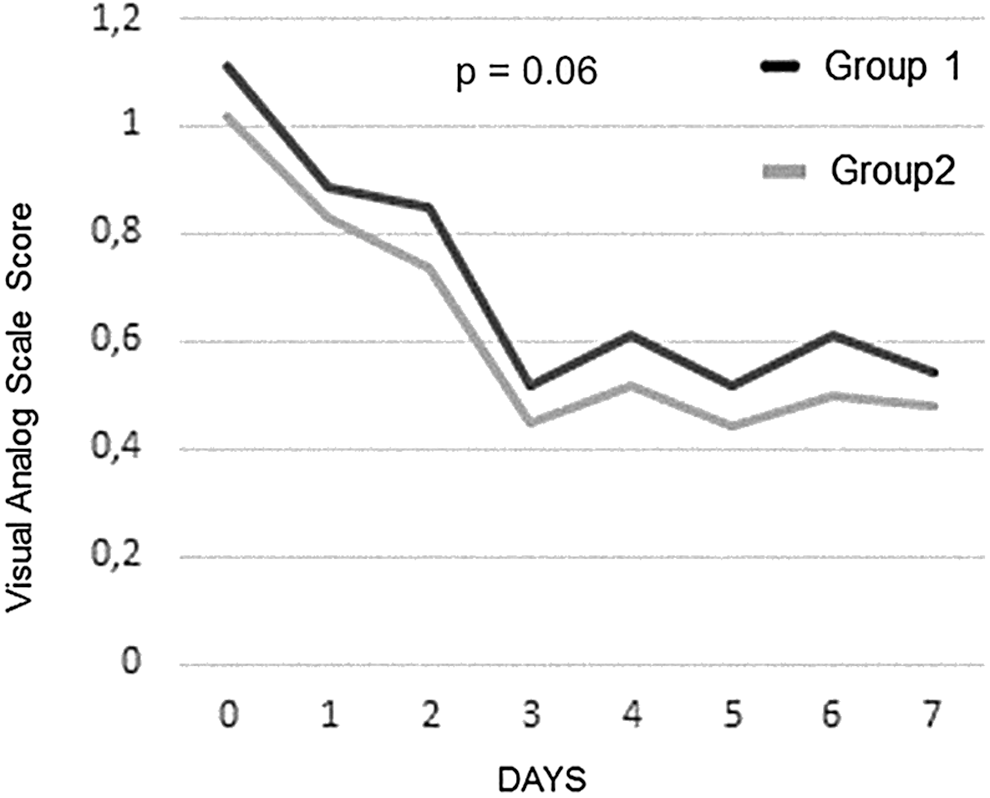
Visual analog pain scale score of patients 7 days after operation.
No patient had urine leak on postoperative cystography, and the catheter was removed.
Patients in our series had no hernia infection. We had taken maximum care to adhere to sterilization rules on the equipment, and used standard antibiotic prophylaxis with cotrimoxazole (800 mg sulfamethoxazole and 160 mg trimethoprim).
The most common complication was postoperative fever in all groups. Fever was classified as a Clavien I complication and reduced by antipyretics. One patient in group 1 and one patient in group 2 needed blood transfusion after operation. This was a Clavien II complication. There was no Clavien III and IV complications in our series. In addition, there was no complication related to the hernia repair recorded in group 1. Moreover, no hernia recurrence was noted in group 1 during the follow-up period.
Discussion
Inguinal hernia can be a common manifestation, with a recorded incidence of 5% to 10% in the male population. 15 Many patients with a diagnosis of PCa may have coexisting unilateral or even bilateral inguinal hernias. Furthermore, inguinal hernias can be an incidental finding during radical prostatectomy (RP) 5 and especially in laparoscopic procedures because of exacerbation of the hernia appearance with insufflation pressures. 16 LRP can have a low risk for postoperative inguinal hernia formation. 17,18 Although surgical management of localized PCa after laparoscopic hernia repair can be hazardous with the open techniques, 19 it is feasible with laparoscopic techniques. 20 In view of these data, it should be common practice that when inguinal hernia is recognized during LRP, it is easier to repair it simultaneously, rather than deal with the postoperative scar tissue in a possible future hernia repair. It can be suggested also that repairing the incidental inguinal hernia during RP can minimize the risk of development of this future potential complication. 6 All parameters above have led to a trend of simultaneous management of the two entities.
As LPR reached its learning curve, there were several studies issued regarding simultaneous laparoscopic hernia repairs. Teber and colleagues 10 performed 50 laparoscopic hernioplasties in 37 patients and compared them with a control group of 37 patients who had only LRP using a matched-pair analysis. They used both the extraperitoneal and the transperitoneal approach and reported a significant increase in the operative time, as well as the narcotic analgesic requirements, with hernia repair. They found no significant differences in the complication rate, however. In our study, after accomplishing 54 simultaneous inguinal hernia cases, these differences cannot be confirmed. These may be related to our operative technique as EPLRP and not using any material for fixing the mesh.
Lee and coworkers 9 described their experience in a retrospective study with 40 patients. Their mean operative time was 172 minutes, and none of the patients presented a hernia recurrence or hernia repair related complication after a follow-up of 10 months. Our results are comparable with them. Finley and colleagues 21 reported their experience in concomitant transperitoneal RALP and intraperitoneal inguinal herniorrhaphy by using prosthetic mesh. They performed 49 hernioplasties in 40 patients and compared them with a matched group of patients who were treated for PCa alone. Operative time was only 10 minutes longer in the intervention group, and no significant complication was noted in a follow-up period of 15 months. Nakamura and associates 12 performed a retrospective comparison study with patients who underwent simultaneous inguinal hernia repair (open, laparoscopic, and robotic), during their RALPs. They were matched with a group of patients who underwent only RALP, and they reported no significant differences in postoperative parameters, including complication rates when compared with other groups. When they compared the three methods for inguinal hernia repair, there was no significant differences in pre-, peri- and postoperative parameters, except in the operative time, which was longer in the open approach. Finally, Do and coworkers 11 presented the largest sample of patients who underwent EPLRP with simultaneous hernia repair. One hundred and nine hernia repairs in 93 patients were performed in a mean operative time of 150 minutes, and no deviation in complication rate was recorded. Limitations of their study were its retrospective nature and the lack of a control group.
All the studies above presented patients who had simultaneous RP with inguinal hernia repair using either the open, laparoscopic, or robotic method through a transperitoneal or extraperitoneal approach. In addition, studies recorded no significant complication rates related to hernia repair. It is also proven true that mesh fixation has not been necessary during extraperitoneal procedures because of the return of the extraperitoneal space to its original capacity after cessation of insufflation, creating a natural fixation of the mesh. Thus, the hazard of complications by clip placement or accidental clip migrations can be avoided.
It is common practice that dissection of the hernia sac should be performed before removal of the prostate, but repair should be performed after the urethrovesical anastomosis, because the only reported recurrences occurred in patients who underwent hernia repair before removal of the prostate. 6 In line with the previous studies, we have prepared the hernias before the lymphadenectomy and prostatectomy. We used a 6×11 cm polypropylene mesh for inguinal hernia repair after accomplishing the anastomoses. Following these principles, our series had no hernia recurrence during a follow-up period of 21 months. All studies above assessed important pre-, peri-, and postoperative parameters, as well as hernia recurrence rates. 9,11,12,21 Most of the series recorded the postoperative analgesic requirement of the patients, but there was no investigation of pain levels and whether they were affected by the simultaneous hernia repair.
Weizer and coworkers 22 quantified postoperative pain levels and analgesic requirements in 98 patients after open perineal RP. They used an analog scale from 1 to 10 and correlated these with other preoperative (age, ASA score, BMI, serum PSA levels), perioperative (lymph node dissection, operative time, EBL), and postoperative (Gleason score, tumor stage, lower extremity neuropraxia) parameters in a multivariate regression analysis. They recorded maximum pain levels in the first postoperative week and baseline levels by the end of the fourth week. In another series of 103 consecutive patients, Sved and associates 23 analyzed postoperative pain and analgesic requirements after open RP with a modified Pfannestiel incision, focusing on the application of spinal instead of general anaesthesia. They recorded a mean value of 4.5 at the patient's discharge, which decreased significantly to 1.5 by the seventh postoperative day, after the catheter was removed, by using the VAS. The analgesic requirements were correlated with the pain scoring levels. Vatansev aand colleagues 24 compared four main techniques for inguinal hernia repair regarding requirements of analgesia in the postoperative period. Seventy-four patients underwent either a Lichtenstein, Nyhus, Bassini, or laparoscopic TEP. By using patient-controlled analgesia during the 24 hours after surgery, they recorded significantly lower analgesic requirements after a laparoscopic hernioplasty.
Finally, Tolver and coworkers 25 tried to assess the different pain components until the fourth postoperative day in 50 patients undergoing a laparoscopic (TAPP) hernia repair, in a prospective designed study. Visceral pain significantly dominated over incisional pain and even more over shoulder pain. There was not any significant difference among the three trocar insertion sites. The pain levels were more intense at 3 hours postoperatively and reached the baseline levels by the third postoperative day. In the present study, all patients experienced only visceral pain, which can be explained by the minimal incision length and the extraperitoneal nature of our technique. Maximum pain levels were observed during the day of the operation, and the pain sensation reduced over the first postoperative week. This condition had another benefit for the patients, because diminished use of analgesics was needed in our series. Therefore, a comfortable postoperative period was essential in our series as well as two different operations could be performed simultaneously. In addition, we had no mesh-related pain and/or complication.
In a previous series, Schlegel and Walsh 15 described the open preperitoneal inguinal hernia repair during open retropubic RP and radical cystoprostatectomy initially. They presented the results of 41 hernia repairs and found no evidence of hernia recurrence with no complication attributable to hernia repairs during a follow-up period of 28 months. Choi and colleagues 26 compared the use of a mesh hernioplasty with the nonmesh technique. They performed 70 open RPs with preperitoneal hernioplasties in 48 patients, 35 with a mesh and 35 without a mesh placement. After a retrospective analysis with 24 months of follow-up, they recorded 14% hernia recurrence in the nonmesh group, and no recurrence in the mesh group. They found no postoperative complication in the mesh placement group. Our series had no hernia recurrence and this finding was parallel to series in the published literature mentioned above. 15,26 In addition, the present series included concurrent operations of EPLRP and hernia repair. Thus, well-known advantages of laparoscopy appeared.
We know the limitations of our study as low numbers of patients. Moreover, some technical challenges may come into question in the case of difficult dissection. Surgeons should be careful while dissecting the inguinal cord and its anatomic structures such as the testicular artery and lymphatic vessels. An interference with the drainage and anastomosis should be also avoided.
On the other hand, as the main goals of the present series, we adapted postoperative pain to the VAS, and additionally compared oncologic and functional parameters in the intervention group with an age, BMI, and ASA scores matched control group who underwent only EPLRP. To the best of our knowledge, this is the first study investigating the postoperative pain levels after EPLRP in a match-paired analysis. The recurrence time of hernia repair has been reported between 8 to 10 months after hernia repair, but we had no hernia recurrence in follow-up. 27
Conclusion
Inguinal hernia can be common in patients with PCa. Simultaneous hernia repair during EPLRP is feasible without extending operative time, and it does not lead to increased complication rates. As a consequence, no alteration in postoperative parameters and, most importantly, no significant difference in postoperative pain levels takes place, making the procedure as tolerable as a simple LRP.
Footnotes
Disclosure Statement
No competing financial interests exist.