
Abstract
Background and Purpose:
Ureteral injuries such as avulsion are directly related to mechanical damage of the ureter. Understanding the tensile strength of this tissue may assist in prevention of iatrogenic injuries. Few published studies have looked at the mechanical properties of the animal ureter and, of those, none has determined the tensile strength of the human ureter. Therefore, the purpose of this work was to determine the tensile strength of the human ureter.
Methods:
We harvested 11 human proximal ureters from patients who were undergoing nephrectomy for either kidney tumors or nonfunctioning kidney. The specimens were then cut into multiple circumferentially and longitudinally oriented tissue strips for tensile testing. Strips were uniaxially stretched to failure in a tensile testing machine. The corresponding force and displacement were recorded. Finally, stress at failure was noted as the tensile strength of the sample. Circumferential tensile strength was also compared in the proximal and distal regions of the specimens.
Results:
The tensile strength of the ureter in circumferential and longitudinal orientations was found to be 457.52±33.74 Ncm−2 and 902.43±122.08 Ncm−2, respectively (P<0.001). The circumferential strength in the proximal portion of the ureter was 409.89±35.13 Ncm−2 in comparison with 502.89±55.85 Ncm−2 in the distal portion (P=0.08).
Conclusions:
The circumferential tensile strength of the ureter was found to be significantly lower than the longitudinal strength. Circumferential tensile strength was also lower with more proximal parts of the ureter. This information may be important for the design of “intelligent” devices and simulators to prevent complications.
Introduction
T
Of the known complications of ureteroscopy, ureteral avulsion is by far considered to be the most severe one. Although avulsion injury rate is generally low at 0.45% in most series but also reported in up to 3.75%, 5,6 it is a devastating complication that potentially can be prevented in different ways. One of them is teaching techniques to avoid and deal with challenging scenarios during ureteroscopy. 7,8 Other solutions are simulators to train new urologists with the procedure before the operating room experience 9,10 and design of “intelligent” equipment that might alert on significant strain. Such intelligent tools may include baskets and graspers that will warn or fail when the operator exceeds a cutoff tension while pulling a stone down the ureter.
To design such intelligent equipment and to improve the available simulators, it is crucial to understand the tensile strength of the ureter.
To the best of our knowledge, the tensile strength of human ureter is not yet reported in the literature. Hence, in this study, we aimed to measure the tensile strength, both circumferential (CIRC) and longitudinal (LONG), of the human ureter.
Methods
After receiving the approval of the Institutional Review Board, we collected 11 ureteral specimens from 11 patients—six men and five women who underwent nephrectomies. The mean age of the patients was 66.8 years (range 56–86 y), and the mean body mass index was 25.2 (range 22.3–27.8). All nephrectomies were performed by the hand assist or laparoscopic approach, and the diagnosis was either kidney cancer or nonfunctioning kidney. No involvement of the renal pelvis or the ureter by tumors was noted. One nephrectomy was performed for a nonfunctioning kidney with a staghorn stone and no evidence of ureteral abnormality. All ureters were resected as distal as possible to allow obtaining a larger specimen. The final specimen was then acquired by resection of the ureter from its proximal attachment to the renal pelvis. Each specimen was kept in sterile saline at 4°C and tested within 48 hours.
The ureter was then cut into multiple CIRC (n=41) and LONG (n=14) oriented tissue specimens for tensile testing (Fig. 1). The initial width and thickness of each tissue specimen was measured using calipers (Scienceware, Wayne, NJ). CIRC specimens were mounted as rings using specially designed hooks, and LONG specimens were mounted directly between the clamps (Figs. 2, 3). The specimen was slowly stretched until a small increase in load was observed; this point was denoted the initial specimen length. The specimens were preconditioned and then stretched until specimen failure as described previously 11 in a uniaxial tensile testing machine (Instron 5543A, Norwood, MA). The corresponding force and displacement was recorded, and a stress-strain curve was plotted. Finally, the tensile strength of the sample was defined as the stress value at failure, where higher tensile strength measurement represents higher force needed for tissue breakdown.

Specimen cut to multiple circumferential and longitudinal oriented tissue segments.
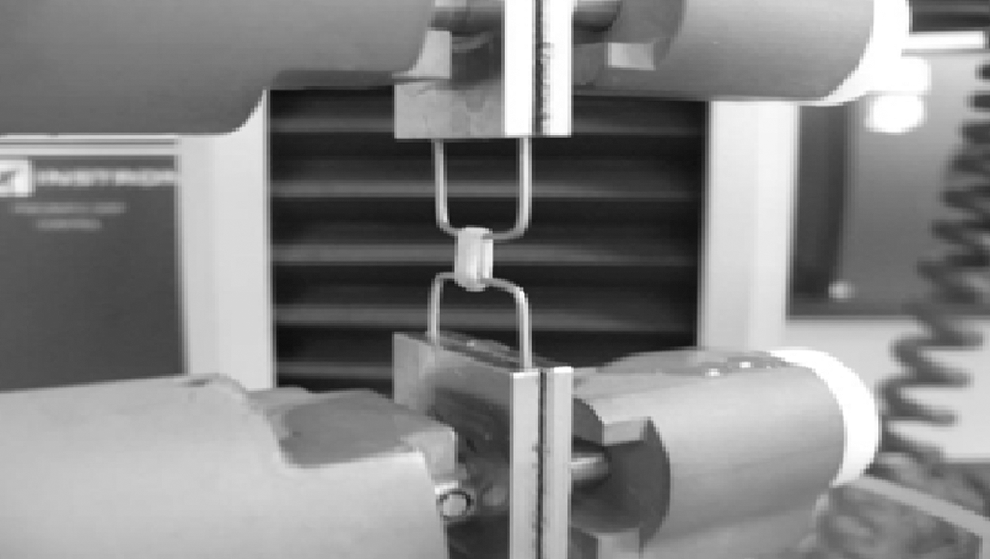
Measurement of circumferential tensile strength.
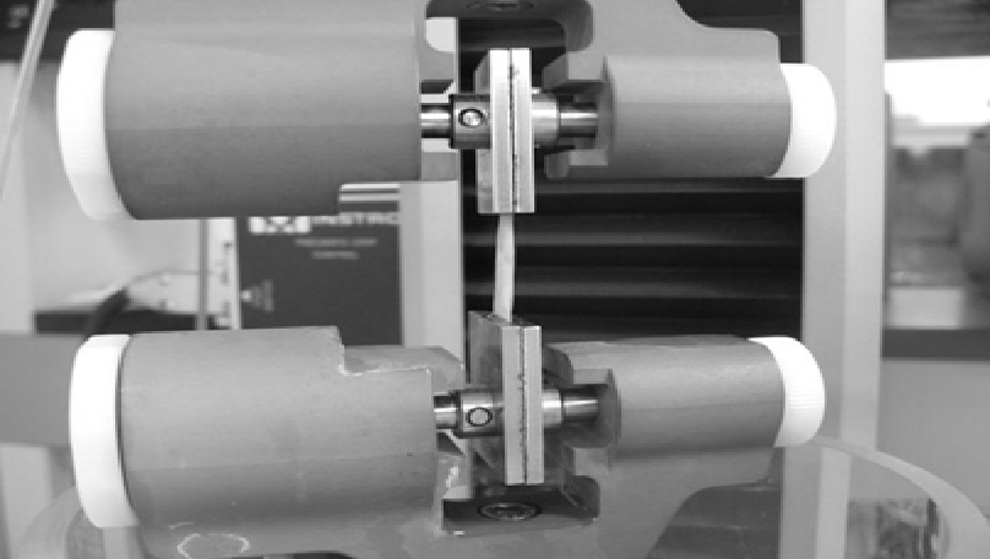
Measurement of longitudinal tensile strength.
CIRC tensile strength was also compared in the proximal (n=20) and distal (n=21) regions of the specimens.
Results
The mean CIRC tensile strength was 457.52±33.74 Ncm2 in comparison with 902.43±122.08 Ncm2 of the LONG tensile strength (P<0.001) (Fig. 4).

Comparison of mean circumferential (CIRC) and longitudinal (LONG) tensile strength.
The CIRC tensile strength was found to be higher in the distal parts of the ureter in comparison with more proximal parts (502.89±55.85 Ncm2 vs 409.89±35.13 Ncm2, P=0.08).
Discussion
The initial studies of biomechanical properties of the ureter were performed on animal models.
In the early 1970s, Yin and Fung 12 published results of mechanical properties of mammalian ureteral segments. They measured elastic parameters in both CIRC and LONG ureteral segments in different mammalian species including human fetuses. They concluded that in some species, different regions in the ureter exhibit different mechanical properties.
Other evidence for different mechanical properties in different areas of the ureter was published by Gregersen and associates. 13 They measured the tension strain distribution at the ureteropelvic junction, middle ureter, and ureterovesical junction in pig ureters by inflation of an intraluminal balloon. They found that the ureteropelvic junction was more compliant than the other two regions.
More recently, Pedro and colleagues 14 conducted a study aiming to examine the avulsion force in a pig model as well as perforation forces in human ureters. They harvested six porcine ureters and placed a stone through a small renal pelvis incision at the ureteropelvic junction. The stone was then trapped using a basket and was pulled down the ureter to find the avulsion force. They measured the average force for avulsion to be 2.21 lb. In our study, we measured similar avulsion forces both LONG and CIRC in a human model.
We found that the CIRC tensile strength was significantly lower than the LONG.
One theoretical explanation for the higher tensile strength of the LONG segments can stem from the physiologic role of the ureter, in which peristalsis in the LONG direction allows urine passage from the kidney to the bladder. The functional process may reflect on the arrangement and configuration of the elastic and muscular layers of the ureter, therefore leading to the difference between CIRC and LONG tensile strength.
Supporting evidence for that can be found in the study of Vargiu and coworkers 15 who analyzed the physiology and configuration of CIRC and LONG muscle layers in 15 proximal human ureters. The LONG muscle layer demonstrated higher mechanical, energetic, and unitary force in comparison with the CIRC layer. The amount of different components in the ureteral wall can also play a role in its compliance and tensile strength. Knudsen and colleagues 16 were looking at collagen content in three areas of the pig ureter—ureteropelvic junction, middle ureter, and ureterovesical junction. The most abundant collagen content was found in the ureteropelvic junction area; however, that was not correlated with differences in the mechanical properties of the different regions.
Another interesting finding in our study is that the CIRC tensile strength was decreasing, although not significantly, with the more proximal location of the specimen. That may imply that the ureter is more vulnerable in its proximal parts than in its distal regions. In their report of four ureteral avulsion cases, Ge and associates 5 reviewed the literature on ureteral avulsion and showed that most of the avulsion injuries were taking place in the proximal parts of the ureter. Whether the biomechanical strength of the proximal ureter is what makes it more prone to avulsion injuries is obviously questionable, but certainly may play a role.
We believe that the preliminary results of this study should be carefully discussed because many limitations exist. While describing differences in the LONG and CIRC tensile strength of the ureter with respect to avulsion, one should remember that it may reflect only one contributing factor of operator pulling forces. Other factors, which are likely to play a role and were not evaluated in the study, are impacted stones that result in local inflammatory processes, strictures, urinary tract infections, previous ureteroscopies, and type of equipment.
No accounting for these factors, as well as sex, age, and other demographics parameters, was performed, but this is a preliminary study that was not designed to overcome these issues.
Furthermore, measurements of tensile strength in this study were performed in a uniaxial model—either LONG or CIRC—whereas in real life, one would think that the ureter is influenced by multiaxial forces. That being said, proposed mechanical characterization and its constitutive equations to predict the multiaxial behavior of the ureter have been described by Sokolis. 17 Although the ureter is a tubular structure like blood vessels, its mechanical loading conditions are different. In blood vessels, the hemodynamic pressure contributes to the multiaxial loading, but in the ureter, the peristalsis implies uniaxial loading. Besides, in the context of ureteroscopy technique, pulling of stones implies that the ureter is predominantly under axial pulling force and hence it is essential to study the ureter strength in uniaxial mode to mimic the surgical procedure.
The importance of this study is in reporting the mechanical strength data of the human ureter. We believe that this information may be valuable for the design of equipment that will be able to “sense” high tensile forces and will alert before avulsion of the ureter. This can also be of importance for simulators and training of the less experienced urologists before performing the procedure in the operating room.
Conclusions
The uniaxial tensile strength of the human ureter is anisotropic between the LONG and CIRC directions. There is also a tendency for difference in CIRC tensile strength along the ureter.
These data may be important for development of simulators and “intelligent” equipment to reduce complications rate.
Further studies are needed to evaluate the tensile strength of the ureter under different circumstances that may change the tissue strength such as inflammations and strictures.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.