
Abstract
Purpose:
We developed a novel device to capture stones in vivo in an enclosed bag (PercSac) to prevent dispersion of stone fragments during percutaneous nephrolithotomy (PCNL) or cystolitholapaxy. We report on our initial feasibility trials of the PercSac device.
Materials and Methods:
PercSac consists of a specially designed polyethylene bag that is fitted over the shaft of a rigid nephroscope. The bag is used to first entrap the target stone, then tighten around it to allow fragmentation within the bag. Matched pairs of 10 canine bladder stones (2.5 cm maximum diameter) were fragmented in a human bladder model using the CyberWand™ (Olympus America, Inc.), and the procedure was assessed for markers of efficiency and effectiveness.
Results:
Median time to entrap the stone within the PercSac was 67 seconds (range 51–185 sec). Median time for stone fragmentation was significantly shorter with the PercSac than without (182.0 sec [range 108–221] vs 296.5 sec [range 226–398], P=0.004). Overall, however, there was no significant difference in the total time to entrap and fragment the stones between the two groups. A stone-free state was not achieved for any trial without the PercSac, while 9 of 10 trials with the PercSac resulted in a stone-free state.
Conclusions:
Use of the PercSac in conjunction with stone fragmentation has the potential to reduce the occurrence of residual fragments after PCNL or cystolitholapaxy. Further in vitro testing in a kidney model is planned.
Introduction
P
In a study exploring the natural history of residual fragments after PCNL, Raman and colleagues 3 found that 43% of patients left with residual fragments >2 mm experienced a subsequent stone-related event, defined as growth of a residual stone or need for an emergency department visit, hospitalization, or additional intervention. As such, strategies aimed at reducing the likelihood of even small residual fragments are desirable. To prevent fragment migration during intracorporeal lithotripsy and thereby limit residual fragments, we developed a novel device, the PercSac, to capture large stones in vivo in an enclosed bag secured to the nephroscope that allows stone fragmentation and aspiration without the possibility of fragment migration.
We report on our initial feasibility trials of the PercSac device in a human bladder model.
Materials and Methods
The PercSac device is a thin, cylindrical, trumpet-shaped polyethylene sleeve that slides over the shaft of a rigid nephroscope and extends beyond the tip to accommodate a 2.5 cm stone (Fig. 1). A nitinol wire incorporated into the circumference of the distal mouth of the bag exits along the length of the bag to its proximal end to provide a mechanism to cinch the bag closed around a stone by pulling on the two ends of the wire. A rigid rod additionally runs along the length of the bag to provide rigidity to the sleeve and facilitate advancing and retracting the bag to capture the stone.
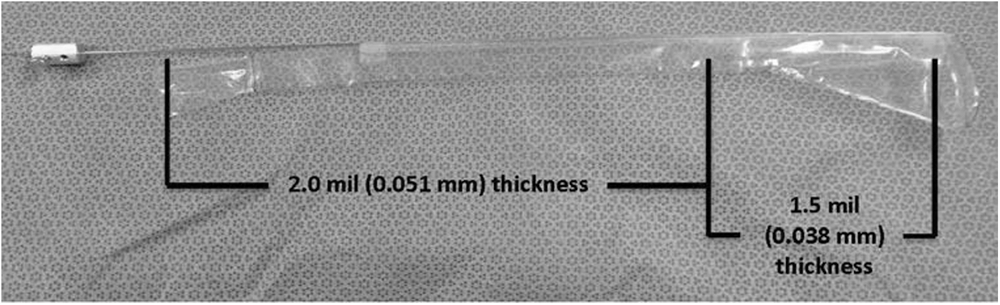
PercSac device. The material of the PercSac sleeve is thicker proximally than distally; the reduced material thickness at the distal end enables tighter cinching of the opening. The expanded distal portion of the sleeve is 7.5 cm long and the proximal portion of the sleeve that fits snugly over the nephroscope shaft is 11 cm long and 9 mm in diameter.
The PercSac is loaded onto the shaft of a rigid nephroscope, and the assembly is passed through a working sheath into the kidney or bladder. As such, the bag is in position to entrap the stone once is it immobilized with a conventional three-pronged grasping forceps passed through the working port of the nephroscope. Once the open bag is advanced around the stone, it is cinched closed by pulling on the nitinol wire. A rubber stopper locking mechanism prevents the nitinol wire from slipping and allowing the bag to open during fragmentation. The stone is then fragmented and aspirated using conventional lithotripsy devices facilitated by continuous flow irrigation through the nephroscope and within the PercSac (Fig. 2).
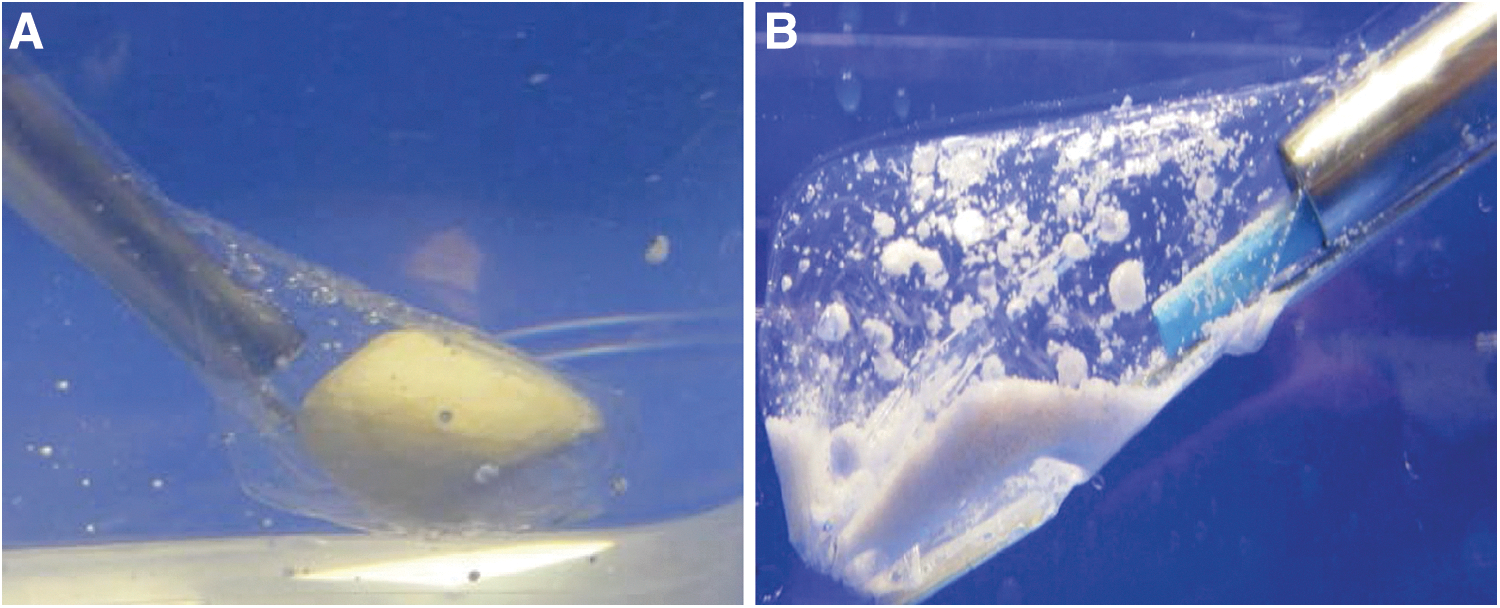
Stone entrapment and fragmentation within the PercSac. (
A total of 10 pairs of canine bladder stones matched for weight and volume (calculated using measured dimensions and the equation for volume of an ellipse) were fragmented in the bladder of a human urinary tract model (Uro-Scopic Trainer

Uro-Scopic Trainer™ with Amplatz working sheath in the bladder. The Uro-Scopic Trainer™ comprises a model of the urethra, bladder, and ureters. A 30F Amplatz working sheath is placed percutaneously into the bladder to accommodate the 24–26F rigid nephroscope.
In the trials using the PercSac, a rigid three-pronged grasper passed through the working channel of the rigid nephroscope was used to capture the stone and immobilize it in the bag. Lithotripsy commenced once the bag was cinched, and the trial was complete when the stone was sufficiently fragmented to allow removal of the bag and its contents through the working sheath. In the trials without the PercSac, lithotripsy was performed on passage of the nephroscope into the bladder, and any remaining fragments not aspirated were then retrieved with the rigid grasping forceps. At the conclusion of each trial, the bladder model was opened and inspected for residual fragments. Statistical analyses for comparison of trials with and without the PercSac were performed with SPSS
Results
The bladder stones used for trials with and without the PercSac were comparable with regard to weight (2.57±0.98 vs 2.63±0.95 g, respectively, P=0.886) and volume (1.78±0.68 vs 1.68±0.63 cm3, respectively, P=0.735). The largest stone by volume captured in the bag was 2.818 cm3 (Table 1). Median time to stone entrapment among the 10 trials with the PercSac was 67 seconds (range 51–185 sec). Median time to stone fragmentation was significantly shorter with the PercSac than without (182.0 sec [range 108–221] vs 296.5 sec [range 226–398], respectively, P=0.004); however, median total fragmentation time did not differ significantly between the two groups (254.5 sec [range 173–302] vs 296.5 sec [range 226–398], respectively, P=0.112).
N/A=Not applicable; N=no; Y=yes.
All trials completed without the PercSac had residual fragments at the conclusion of the procedure. In contrast, all but one trial involving the PercSac resulted in no fragments left behind. Residual fragments were approximately 2 to 6 mm and had migrated out of the field of vision as opposed to not being cleared through suction. In no PercSac trial was the integrity of the bag compromised by the probe or stone.
Discussion
The goal of our study was to determine the feasibility, efficiency, and effectiveness of a novel stone entrapment device to contain stone fragments during intracorporeal lithotripsy. Using a human bladder model, we showed that percutaneous lithotripsy with the PercSac shortened the time for stone fragmentation and removal. The extra time needed to capture and secure the stone in the PercSac, however, was comparable to the time saved with fragmentation and removal, such that efficiency with regard to time was comparable with and without the PercSac. Stone-free rates, however, were superior with the PercSac, making the device more effective for stone fragmentation and removal. We believe that once the process of entrapping the stone in the sack is perfected, additional time savings may be realized.
The PercSac is able to capture stones with the intention of preventing migration of fragments into inaccessible locations or obviating the need for extensive flexible nephroscopy and fragment retrieval. We demonstrated that the PercSac could be relatively efficiently loaded onto the shaft of a rigid nephroscope and passed through the working sheath into the bladder. Furthermore, we showed that ultrasonic lithotripsy could be performed without injuring the bag. Secure closure of the sack is necessary to insure that fragments are not lost in the bladder/kidney. In the one PercSac trial in which fragments remained, we noted that the bag was not completely cinched, allowing a small volume of fragments to escape. In a majority of cases, it took approximately 1 minute to capture the stone within the sack, but larger stones needed more time to ensure complete containment of the stone within the bag. Future refinements of the device will be necessary to improve the efficiency of this maneuver.
Migration of stone fragments during PCNL is common and necessitates careful endoscopic inspection of the entire collecting system and ureter to assure that all fragments have been located and removed. Likewise, during cystolitholapaxy, removing fragments by irrigation or manually can be time consuming and tedious. In either case, residual fragments place the patient at risk of obstruction and/or provide a nidus for continued stone growth. Both sequelae can result in need for secondary procedures and the attendant additional cost.
The consequences of residual fragments after PCNL have been well documented. Raman and colleagues 3 identified 42 patients with untreated residual fragments among 527 patients who underwent PCNL and had a minimum of 6 months of radiographic follow-up. 3 At a median follow-up of 32 months, 18 patients (43%) with residual fragments (median diameter of 2 mm) experienced a stone-related event, defined as an increase in residual fragment diameter, emergency department visit, hospitalization, or secondary procedure to relieve obstruction or pain, during surveillance. By multivariate analysis, maximal residual fragment size >2 mm (hazard ratio [HR] 3.9, P=0.01) and location in the renal pelvis or ureter (HR 4.4, P=0.01) proved to be independent predictors of a stone-related event.
Altunrende and coworkers 4 also followed the natural history of 38 patients with residual fragments and at least 24 months of follow-up among 430 patients who underwent PCNL. At a median follow-up 28.4 months, although of none of the patients with residual fragments needed surgical intervention, 26.3% experienced a symptomatic episode, 21.1% demonstrated growth of the fragments, and 7.9% spontaneously passed their stones.
These studies underscore the potential morbidity associated with residual fragments, with larger fragments carrying greater risk. Secondary procedures to remove residual fragments, however, are also accompanied by potential morbidity and cost. Raman and associates 5 performed a cost analysis to determine the cost-effectiveness of second-look flexible nephroscopy vs conservative management of patients with <4 mm residual fragments after PCNL. Using a prevalence of stone-related events (40%) obtained from their own analysis as well as from natural history studies from the shockwave lithotripsy literature and costs associated with second-look flexible nephroscopy derived from their institution, they calculated the average cost of conservative management for residual fragments ≤4 mm and >4 mm at $1743 and $4674, respectively. With an average incremental cost of $2475 for second-look flexible nephroscopy, they reasoned that a strategy of routine second-look flexible nephroscopy is cost effective for patients with >4 mm residual fragments.
Strategies that reduce the likelihood of residual fragments obviate the need for secondary procedures with their attendant cost and morbidity. A variety of devices have been introduced to prevent fragment migration and reduce the likelihood that fragments are missed, some of which were initially intended to prevent retropulsion of fragments during ureteroscopy. These devices differ from the PercSac during use with PCNL in that they are only able to prevent antegrade migration of fragments down the ureter, but have no effect on the dispersion of fragments generated during percutaneous lithotripsy within the kidney. Springhart and colleagues 2 evaluated the use of the Stone Cone™ (Boston Scientific, Natick, MA) during PCNL to prevent fragment migration into the ureter. This device consists of a coated coaxial sheath that forms a coil when deployed that occludes the ureteral lumen proximal to the stone (with ureteroscopy) during stone fragmentation and, when withdrawn, can sweep fragments out of the ureter. Among 10 patients in whom the Stone Cone™ was successfully deployed during PCNL, no fragments migrated antegrade into the ureter.
Wosnitzer and coworkers 6 used another anti-retropulsion device, the Accordian™ (PercSys, Palo Alto, CA), to prevent antegrade fragment migration during PCNL. This device consists of a microcatheter on which is mounted a thin film. The assembly is passed up the ureter alongside the stone like a guidewire, but once deployed, the film expands creating folds that occlude the ureteral lumen. These investigators performed PCNL in 60 consecutive patients, 30 without the Accordian device and 30 with the device. The Accordian was successfully deployed in the 30 patients in whom it was intended, and it prevented stone migration into the ureter in all but one (3.3%) patient. The authors noted that the single failure occurred in a patient with a very dilated ureter for which the device was not completely occlusive. Stone-free rates in the groups with and without the Accordian were not provided.
While these devices have the advantage over the PercSac that they can be used with any size stones, including staghorn calculi, to prevent migration into the ureter, they cannot contain fragments during lithotripsy.
At present, the PercSac cannot be used with larger stones (>2.5 cm) both because of the size of the bag, but more importantly because large stones prevent visual confirmation of complete bag closure, thereby potentially allowing small fragments to escape during lithotripsy, as occurred in one of our trials. This limitation stems from the design of the device in that the bag opens on the distal end rather than on the side of the sleeve, which allows the stone to block the line of sight from the nephroscope to the closed end of the bag. Although not tested here, other lithotrites with stronger suction may collapse the bag, a phenomenon that we did not experience using the CyberWand. At present, it is also unclear whether the bag would withstand pneumatic lithotripsy. These points need further evaluation.
Conclusions
The PercSac is a novel stone-capturing system that prevents dispersion of fragments generated during PCNL or cystolithalopaxy, potentially reducing the incidence of residual fragments. Our pilot study demonstrated feasibility and effectiveness of the device in reducing residual fragments. Further design modification and in vitro testing in a kidney model is planned.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.