
Abstract
Purpose:
To investigate the relationship between renal parenchymal volume (RPV) and renal function in obstructed kidneys using a novel three-dimensional (3D) volume-rendering technique.
Materials and Methods:
Forty-seven consecutive patients who underwent pyeloplasty, ureteroureterostomy, or ureteroneocystostomy at a single institution between 2007 and 2013 were reviewed. Patients with preoperative CT scan and split differential functional (SDF) assessment by diuretic renography were included. Those with solitary kidneys and bilateral obstruction were excluded. Baseline serum creatinine (Cr) and estimated glomerular filtration rate (eGFR) as calculated by the modification of diet in renal disease equation were determined. Percent of total RPV for the obstructed kidney was determined using 3D reconstruction software by drawing regions of interest around the borders of the kidney on CT. The renal pelvis, hilar vessels, and hilar fat were excluded. Percent of total RPV was then correlated with SDF.
Results:
Nineteen patients with both preoperative CT and diuretic renal scans were included. Two underwent ureteroneocystostomy, 1 underwent ureteroureterostomy, and 16 underwent pyeloplasty. Mean serum Cr was 1.07±0.26 mg/dL with a mean eGFR of 69.43±18.90 mL/minute. Mean SDF was 37.32%±11.66% in the obstructed kidneys. There was a statistically significant correlation between percent of total RPV and SDF (R 2=0.28, p=0.02).
Conclusions:
There is a significant correlation between percent total RPV determined by 3D reconstruction of CT scan images and SDF as determined by diuretic renography in obstructed kidneys. CT-based percent RPV has potential as a functional assessment tool in obstructed kidneys. With further validation, it may be used to counsel patients considering surgical repair of ureteral or ureteropelvic junction obstruction.
Introduction
T
Diuretic nuclear renography is a commonly used diagnostic procedure used to assess differential renal function and confirm or deny suspected renal obstruction. The decision to pursue surgical repair of obstructed kidneys versus nephrectomy is often based on degree of functional impairment in the affected kidney. In practice, a cutoff of 15% split differential function (SDF) is commonly used by urologists when counseling patients to undergo repair versus nephrectomy. 4 Preoperative volume assessment with computed tomography has been proposed as a possible functional estimation tool in patients with obstructed renal units. The objective of this study was to correlate percent of RPV with SDF estimation in obstructed renal units that subsequently underwent surgical repair.
Materials and Methods
Patients
After obtaining institutional review board approval, the case logs of two surgeons (T.T., A.F.) at a single academic medical center were retrospectively reviewed. Forty-seven patients underwent ureteroureterostomy, ureteroneocystostomy, or dismembered pyeloplasty from July 2007 to October 2013. Patients with a solitary kidney or bilateral obstruction were excluded from the analysis. Those with both preoperative helical CT scan images of both kidneys in their entirety and diuretic nuclear renography were included in our analysis. Patients with nephrostomy drainage underwent diuretic nuclear renography with the tube capped, as per institutional protocol. Patients with renal scans obtained at outside institutions were included provided the protocol utilized was consistent. Mechanical obstruction was defined as T ½ >20 minutes in the affected kidney. Nineteen patients met the criteria for volume acquisition and were included in the analysis. Serum Cr was obtained from blood test records before treatment for obstruction. Baseline renal function was estimated with the MDRD-GFR equation. 5,6
Percent of total RPV measurement
RPV was obtained in both kidneys for each patient using our previously described three-dimensional (3D) volume method. 7 Regions of interest were then drawn around the kidney parenchyma on axial slices of 2.5 mm thickness. Renal sinus fat, collecting system, and hilar vessels were excluded from the regions of interest (Fig. 1). The percent of total RPV in the obstructed kidney was then calculated by dividing the RPV in the obstructed kidney by the total RPV. All 19 CT scans were processed by the same user (T.D.). To our knowledge, this represents a novel method of volume acquisition in obstructed renal units.
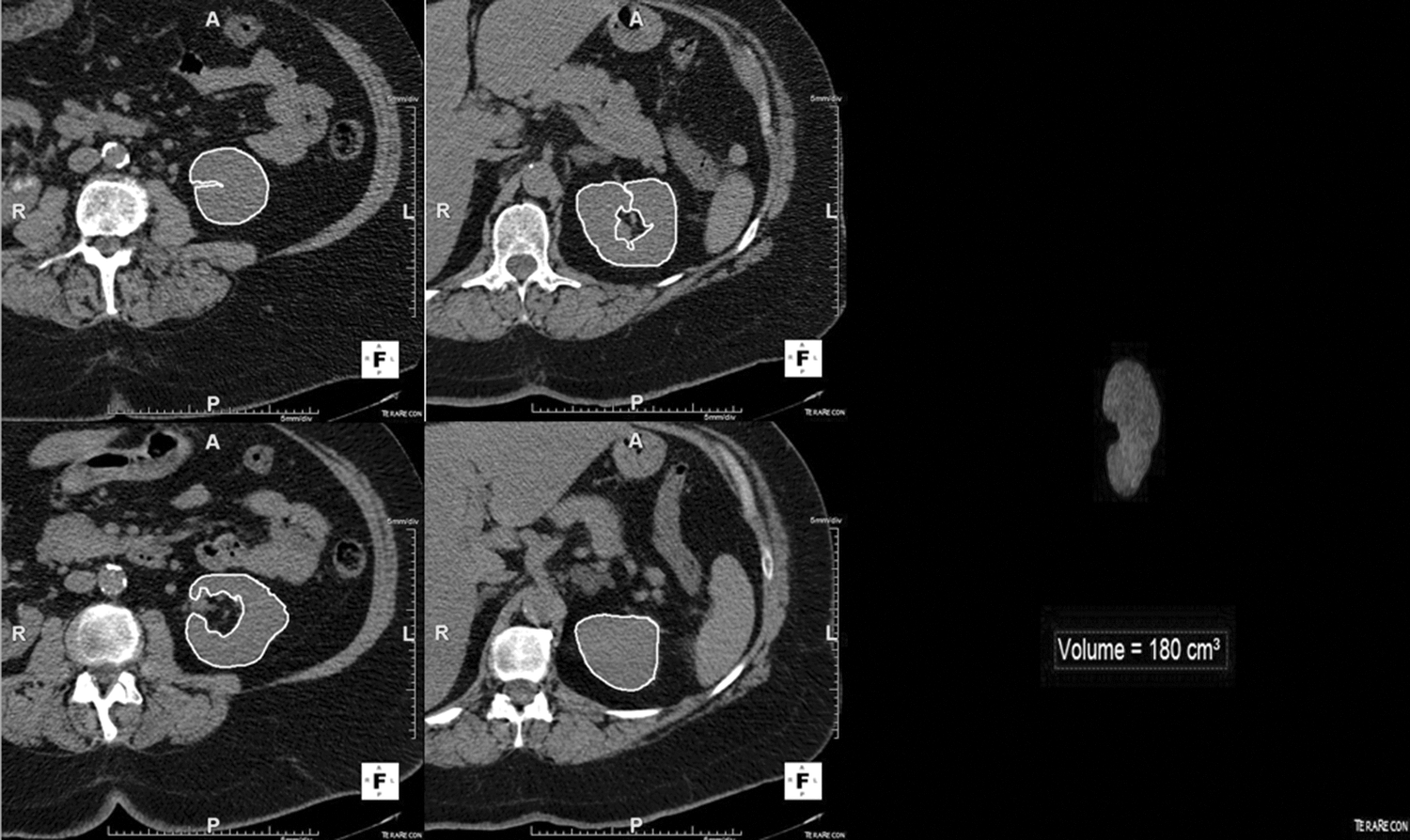
Measurement technique: regions of interest were drawn around renal parenchyma. Sinus fat and hilar vessels were excluded from these regions. A region was drawn for every slice of each scan. Three-dimensional volume rendering the then automatically calculated parenchymal volume from the regions drawn.
Statistical analyses
Linear regression analysis was used to analyze the relationship between RPV and renal function. IBM® SPSS® Statistics Version 20 (Chicago, IL) was used to perform all statistical analyses. Correlations between the two measures were evaluated using the Pearson coefficient.
Results
Of the 47 patients who underwent surgical repair of urinary tract obstruction, 19 were identified as having both preoperative helical CT scan images of the kidneys and MAG3 lasix renal scans. The mean age of our cohort was 45, with a nearly even split of male and female patients (10 female, 9 male). Two patients underwent ureteroneocystostomy, 1 underwent ureteroureterostomy, and 16 underwent dismembered pyeloplasty. Of the pyeloplasties, two were performed using an open technique, while the remaining were performed laparoscopically. The three patients who underwent ureteroneocystostomy and ureteroureterostomy had obstruction from iatrogenic causes and were repaired using an open technique. All patients who underwent dismembered pyeloplasty had radiologic evidence of ureteropelvic junction obstruction.
Mean serum Cr on presentation was 1.07±0.26 mg/dL with a mean estimated GFR (eGFR) of 69.43±18.90 mL/minute. Mean SDF was 37.32%±11.66% in the obstructed renal units based on nuclear renography (Table 1). All patients had T ½ >20 minutes in the affected kidney. Mean percent of total RPV was 48.33%±6.6%. There was a statistically significant correlation between percent of total RPV and SDF (R 2=0.28, p=0.02) in obstructed kidneys (Fig. 2).
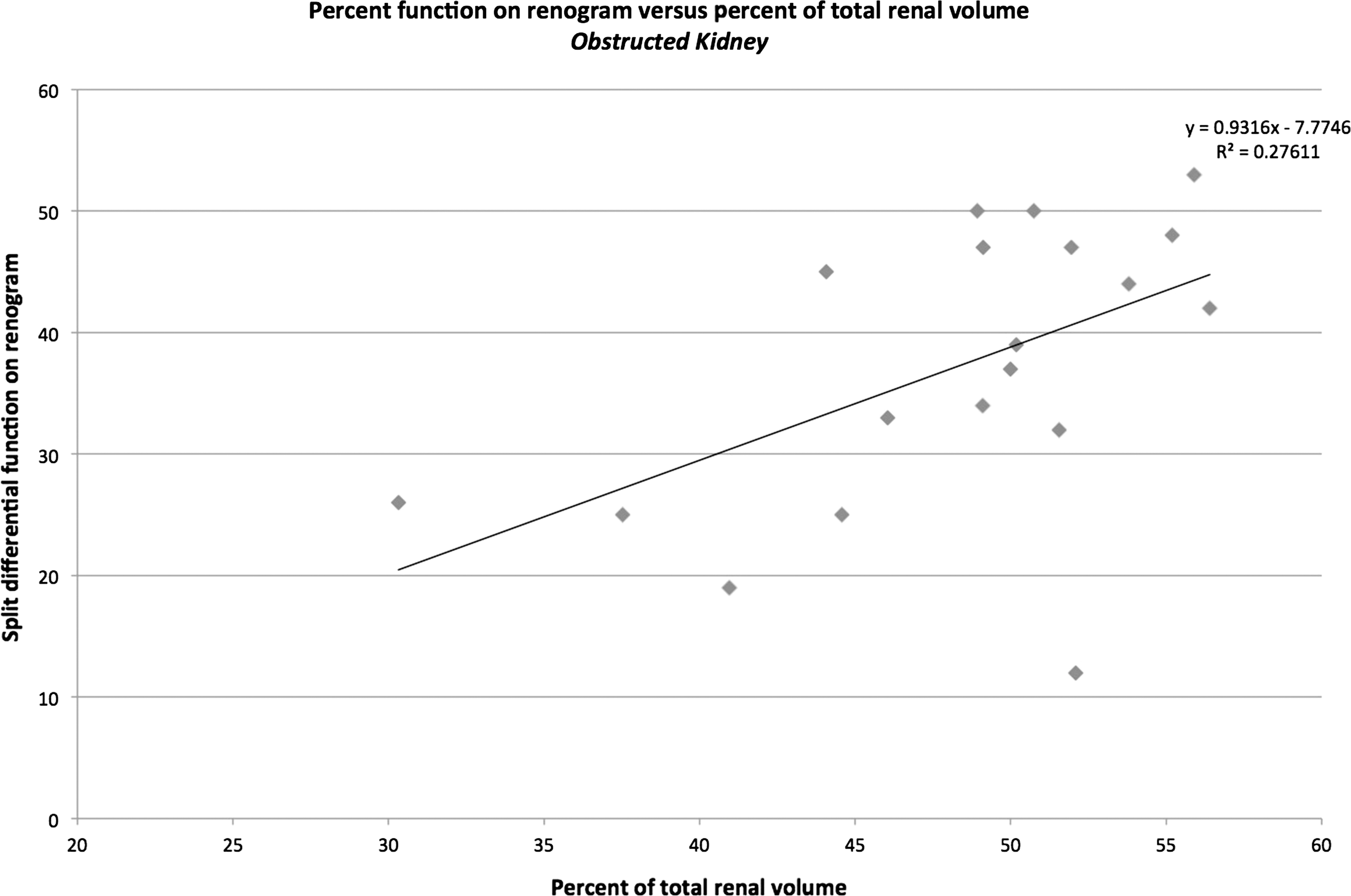
Linear regression of the percent of total renal parenchymal volume with split differential function on renogram. For this regression, R 2=0.28 and p<0.02.
Cr=creatinine; eGFR=estimated glomerular filtration rate.
Discussion
Urinary tract obstruction is multifactorial and if left untreated often leads to renal impairment in the affected unit. Urolithiasis, ureteral stricture, iatrogenic ureteral obstruction, and ureteropelvic junction obstruction are the most frequently encountered etiologies for ureteral obstruction. Patients undergoing procedures for ureteral or ureteropelvic junction obstruction typically have cross-sectional imaging and estimation of renal function that may impact surgical decision-making. Split differential renal function as determined by diuretic nuclear renography is commonly used by urologists to counsel patients toward surgical repair versus nephrectomy. Obstructed renal units with a SDF of less than 15% in the setting of a normally functioning contralateral kidney are often counseled to undergo nephrectomy, as the chance of recovering meaningful function in adults is minimal. 4 Contemporary studies have even suggested that the chance of recovering meaningful renal function is minimal in kidneys with a differential function <30%. 8 Nuclear renography is also commonly used in the postoperative period for assessment of obstruction alleviation. 9
We have previously reported that RPV can be assessed easily and accurately using automated 3D reconstruction. 7 This method is yet to be used to evaluate function in obstructed renal units that subsequently underwent surgical repair. The ease of being able to directly send CT scans from image storage to the software server for automatic 3D rendering makes this method efficient in the preparation of making the necessary measurements. Our values for total RPV and individual RPV as stated above are in line with values previously reported by those using other methods. 1,10 –12
The relationship between RPV and function is an area of active research. The correlation between the renal parenchymal area on computed tomography and function has been previously established. 13 Computed volumetry was also proposed as a surrogate for function in the kidney donor population for unobstructed renal units. 14,15 Sarma et al. recently reported a strong correlation between percent renal volume and percent renal function in obstructed units (r=0.828, p<0.001) as well as in nonobstructed units (r=0.827, p<0.001). 16 This study corroborates our results using an automated volume-rendering software. Semiautomated volume rendering with manual editing of parenchymal boundaries has also been used to correlate PRV with function in chronically obstructed kidneys with suspected impairment. 3 Estimation of differential renal function based on renal parenchymal thickness on preoperative CT has been shown to correlate well with postoperative differential renal function on nuclear renography following laparoscopic pyeloplasty in a recent series. 2 In a similar study, absolute RPV was an independent factor that determined recoverability of renal function following relief of obstruction. Renal function was shown to stabilize or improve after relief of urinary obstruction with preoperative RPV values ≥58.2 mL. 17
To our knowledge, this is the first study to utilize a 3D volume rendering software with manual boundary delineation to correlate percent total RPV with SDF based on nuclear renography in obstructed renal units that subsequently underwent surgical repair with dismembered pyeloplasty, ureteroureterostomy, or ureteroneocystostomy. Our study was subject to the known limitations of retrospective studies. The cohort also represents a series of patients seen at a tertiary academic medical center introducing the possibility of selection bias. The small sample size also limits the study and would require further validation with a larger series for clinical application. Patients with undiagnosed renal disease could potentially have been analyzed and may have impacted our data. In addition, the use of nonenhanced CT scans could have obscured the distinction between hilar vessels and renal parenchyma. It should be noted that this represents a preliminary study with the intention of validating the concept in a larger cohort before suggesting clinical impact. If validated as a functional assessment tool in larger studies, the absolute necessity of renography in the diagnostic algorithm for all patients considering surgical repair may be called into question.
Conclusion
This preliminary study demonstrates a significant correlation between percent total RPV determined by 3D reconstruction of CT scan images and SDF, as determined by the nuclear renal scan in obstructed renal units that subsequently underwent repair. CT-based percent RPV has the potential as a functional assessment tool in kidneys with ureteral or UPJ obstruction that are candidates for repair. With further validation, it may be used to counsel patients considering surgical repair of ureteral or ureteropelvic junction obstruction.
Footnotes
Disclosure Statement
No competing financial interests exist.