
Abstract
Introduction and Objectives:
Patients with urolithiasis are exposed to significant amounts of radiation during their initial work-up, surgical treatment, and follow-up. The purpose of this study was to determine the feasibility of performing ureteroscopy without fluoroscopy. In addition, we compared patients treated using a completely fluoroless ureteroscopic technique with a cohort of conventional ureteroscopies performed using fluoroscopy.
Materials and Methods:
A retrospective review of 50 consecutive patients undergoing fluoroless ureteroscopy was performed. These procedures were performed by inserting guidewires and instruments using tactile feedback, direct visualization, and external visual cues to substitute for fluoroscopy. In addition, this cohort was compared with 50 conventional, fluoroscopy-guided ureteroscopies performed in the same time period.
Results:
Fifty ureteroscopies were performed without image guidance. For this cohort, the mean operative time was 59.2 minutes, overall stone burden was 91.53 mm2, complication rate was 4%, and repeat procedure rate was 8%. Compared with conventional ureteroscopy the fluoroless ureteroscopy patients had a larger stone burden (p=0.042; 91.53 vs 56.58 mm2), but similar age, gender, American Society of Anesthesiologists (ASA) score, body–mass index, operative time, complication rate, and repeat procedure rate.
Conclusions:
This study demonstrates the feasibility and efficacy of the completely fluoroless ureteroscopic treatment of calculi throughout the entire upper urinary tract while completely removing radiation exposure to the patients and staff. Although this fluoroless technique may be most applicable in patients at highest risk for radiation exposure, such as pregnant women, children, and recurrent stone formers, it offers an alternative for reduction of radiation in all patients.
Introduction
I
Fluoroscopic imaging routinely plays an integral role during ureteroscopic lithotripsy. It is commonly used to identify stones, assist in renal mapping, and verify placement of guidewires, stents, and ureteral sheaths. A limitation of fluoroscopy is the potentially significant radiation exposure to the patient, physician, and operating room staff. There is no lower limit of radiation exposure below which potentially harmful biologic effects do not occur; therefore, any exposure has the possibility to induce malignancy. 2,3 All ionizing radiation carries with it the potential to cause cancer. 4 In an attempt to reduce radiation for patients, we developed a novel technique for ureteroscopy. The purpose of this study was to determine the safety and feasibility of ureteroscopy without image guidance and to compare outcomes of a cohort of fluoroless ureteroscopy patients with a cohort of conventional ureteroscopy patients performed using fluoroscopy.
Materials and Methods
Between January 2009 and December 2012, 50 cases of simple ureteroscopic lithotripsy of renal and ureteral stones performed at a single institution, by a single surgeon, without the use of fluoroscopy or ultrasound were retrospectively evaluated. Exclusion criteria for consideration for a fluoroless technique included ureteroscopy for malignancy, duplicated collecting systems, previously documented strictures, and treatment of nonurolithiasis-related conditions. Demographic and perioperative information recorded included age at time of surgery, gender, American Society of Anesthesiologists (ASA) score, laterality, body–mass index (BMI), presence of preoperative stent, stone location, and mean operative time. Stone size was calculated by multiplying the two largest cross-sectional dimensions to obtain a stone area in millimeters squared. Outcomes analyzed included complication rates, stone-free rates (defined as no residual stone >4 mm), and repeat procedure rates.
We then compared these patients with a similar cohort of 50 patients who underwent ureteroscopy for urolithiasis with conventional fluoroscopic guidance by other academic urologists in our institution in the same time period. The same demographic, perioperative information, and outcome measures were collected. Groups were compared with a Mann–Whitney U test or Student's t-test for continuous variables and Fisher's exact test for categorical variables. Significance was set at p<0.05.
Technique for fluoroless ureteroscopy
The procedure begins with a thorough assessment of preoperative imaging. While the patient was under general anesthesia, the patient was placed in the lithotomy position. A rigid cystoscope with a 30-degree lens was introduced to inspect the bladder for any abnormalities. After locating the desired ureteral orifice, a 6F end-hole catheter at the ureteral orifice was used to advance an angle-tipped glidewire (Terumo Medical Corporation, Irvine, CA) up the ureter (Fig. 1A). If a previous stent was in place, this wire was placed beside the existing stent before removal. Using tactile feedback, the glidewire was gently manipulated proximally until the resistance of the stone could be felt. With gentle back and forth movements, the wire was advanced beyond the stone and up until resistance from contact with the kidney was encountered. The external length of the wire was then compared with Yellofins Elite Stirrups (Allen Medical Systems, Acton, MA) used to hold the patient in the lithotomy position. In our previous reduced fluoroscopy protocol, we learned that regardless of patient height, the internal tip of the wire was correctly located in the kidney when the external tip of the wire was within 10 cm of the end of the stirrup. 5
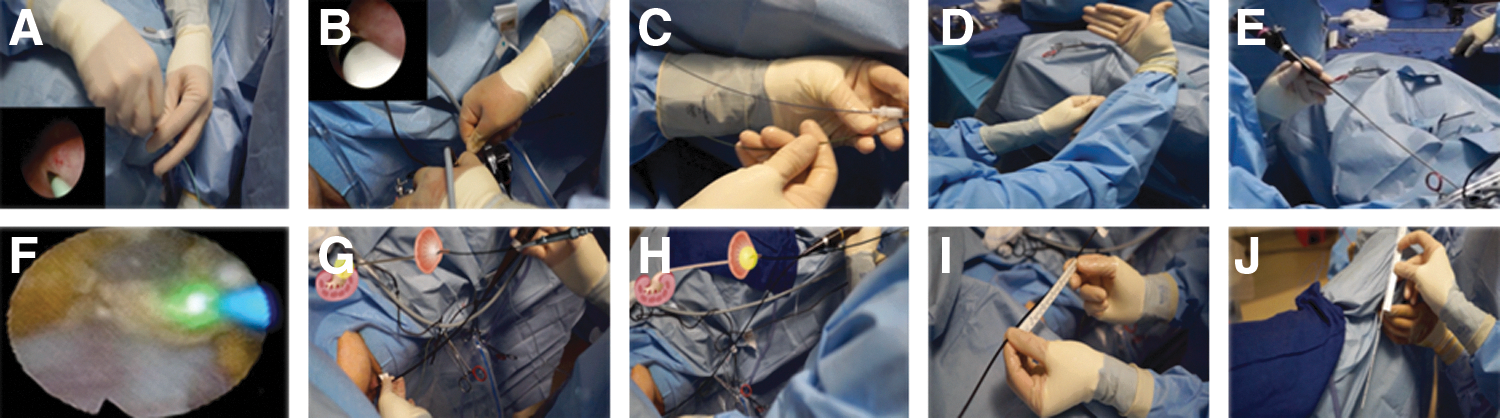
Fluoroless ureteroscopy technique.
Using tactile manipulation, a 6F end-hole catheter was then advanced over the glidewire proximally until the end-hole catheter tip was 1 to 2 cm past the stone. With distal stones requiring only semirigid ureteroscopy, the glidewire was exchanged for a standard guidewire to be used as a safety wire. The open-ended catheter was removed and the cystoscope was used to empty the bladder, while the safety wire was left in position. The semirigid ureteroscope was advanced under direct vision until the stone was encountered.
For flexible ureteroscopy, a dual lumen ureteral access catheter was used to gently dilate the ureteral orifice (Fig. 1B) and place a second guidewire (Fig. 1C); one as a safety wire and the other as the access for ureteroscope insertion. The two wires were compared for appropriate length confirming correct placement in the kidney (Fig. 1D). No ureteral access sheaths were used. During ureteroscope insertion, the two main locations where resistance that provides tactile feedback occurs are when the ureteroscope passes the prostate/bladder neck and the ureteral orifice. The flexible ureteroscope was advanced beyond the ureteral orifice while the assistant held the guidewire taut (Fig. 1E). The guidewire was then removed and the flexible ureteroscope was navigated under direct vision until the stone was identified. All stones were fragmented using a holmium laser (Fig. 1F) with selective extraction of smaller fragments based on the surgeon's preference. A systematic endoscopic renal mapping was performed to ensure complete stone fragmentation.
Following completion of stone treatment, a stent was placed in all patients using a previously described technique. 6 The length of the ureter was determined by marking the location of the ureteropelvic junction (UPJ) externally on the ureteroscope with an adhesive tape (Fig. 1G). We then pulled the ureteroscope back to the ureterovesical junction (UVJ) while inspecting the ureter to evaluate mucosal integrity and assess for residual stones. The level of the UVJ was also marked on the ureteroscope (Fig. 1H), and the difference between the two marks corresponded to the ureteral length measured under direct vision (Fig. 1I). During semirigid ureteroscopy, if the ureteroscope would not pass up to the UPJ, the ureteral length could be estimated using the preoperative CT. A 6F multilength stent was then advanced proximally over the safety wire into the ureter under direct visualization. After advancing the stent proximally to the appropriate ureteral distance (Fig. 1J), the guidewire was pulled back 10 to 15 cm and the stent was then advanced under direct vision within the bladder until the distal end was at the mid bladder neck. The wire was removed and a proper bladder coil was endoscopically confirmed.
At any point during the procedure, if excessive resistance was encountered during guidewire or ureteroscope insertion, if wire lengths were not appropriate following placement, or if a tightly impacted stone was not amendable to passing the guidewire, the patient was converted to an ultralow-dose fluoroscopy-guided technique.
Results
Between 2009 and 2012, 50 ureteroscopies to treat urolithiasis were performed without intraoperative image guidance. Patient characteristics are labeled in Table 1. Renal units were predominately from male patients (70%) and laterality was equally distributed. The average patient was obese with a BMI of 30.19 and age was 54.62 years (16–83). Intraoperative characteristics included 18 patients (36%) with prior indwelling ureteral stents at the time of ureteroscopy. Overall stone burden was 91.53 mm2 (14–480 mm2). Stone locations were characterized as follows: isolated renal 17 (34%), isolated proximal ureter 5 (10%), isolated mid ureter 2 (4%), isolated distal ureter 14 (28%), and multiple locations 12 (24%). The mean operative time was 59.2 minutes (25–121 minutes). No intraoperative complications were observed.
Continuous data are shown as mean (range) and categorical data as number (%).
ASA=American Society of Anesthesiologists; BMI=body–mass index.
Postoperative outcomes included a complication rate of 4%, with both occurrences in the same patient who was a pregnant woman with a large bilateral renal stone burden secondary to bilaterally entombed nephrostomy tubes. We performed bilateral fluoroless ureteroscopies for removal of nephrostomy tubes and insertion of bilateral ureteral stents because of her pregnancy status. Postoperatively, she developed fever and bilateral Steinstrasse requiring retreatment. There were two more incidents of repeat procedures (8%) for residual stone >4 mm, both electing for shockwave lithotripsy.
When compared with conventional ureteroscopy with image guidance, there was no statistical difference in age (p=0.771), BMI (p=0.620), ASA (p=0.918), or operative time (p=0.806). Logistic regression multivariate analysis was performed with all study parameters in relation to the repeat procedure rate. It was found that stone size >75 mm2 was significantly predictive (p=0.049) of repeat procedures with an odds ratio of 5.8 in both groups. There was no association between the fluoroless technique and gender (p=0.518), laterality (p=0.689), previous stent (p=0.387), complication rate (p=1.00), or repeat procedure rate (p=0.678) (Table 1).
Discussion
The prevalence of urinary calculi is 2% to 3% in the general population, 7 and over a lifetime, urinary calculi are expected to afflict greater than 12% of men and 6% of women with a recurrence rate of 30% to 40% within 5 years. 8 The prevalence of urinary calculi appears to be increasing in the United States. 9 Radiographic imaging is necessary to confirm or exclude urinary calculi, 7 and those patients with recurrent abdominal or flank pain are at risk for multiple doses of diagnostic radiation. Furthermore, this dose effect is increased when intervention is warranted. Although the doses are not routinely high enough to cause the deterministic effects of radiation such as skin burns, the stochastic effects of radiation may result in the creation of malignancy. 4 Certainly, the reduction of the radiation exposure will reduce the risk of radiation-associated morbidity.
Fluoroscopy is routinely employed to guide the surgeon during upper tract stone treatment. Performing the procedure with reduced amounts of fluoroscopy represents a significant departure from the conventional endoscopic technique. In the field of interventional cardiology, Georges et al. 10 reported a 50% reduction in radiation exposure with a 15-hour educational course and standardized radiation reduction technical recommendations. This fluoroless ureteroscopic technique was undertaken cautiously only following extensive experience with reduced fluoroscopy protocols. 5,6,11 We have previously reported a reduced fluoroscopy protocol that allowed us to reduce the fluoroscopy time from 82 to 15.5 seconds for simple uncomplicated ureteroscopy. 5
As we became comfortable with these reduced fluoroscopy techniques, we realized that ureteroscopy could be performed entirely without fluoroscopy in carefully selected patients. We are not the first discipline to omit fluoroscopy from previous image-guided procedures. Interventional cardiologists are now performing cardiac ablations for the correction of atrial fibrillation and tachycardia using a completely fluoroless technique in children, pregnant women, and obese patients. 12 –14 In gastroenterology, studies have shown that endoscopic retrograde cholangiopancreatography can be performed without fluoroscopy. 15 Spinal surgeons are now performing craniosacral posterior spinal instrumentation using a fluoroless technique with similar outcomes to the conventional technique. 16
In urology, there have been three previous studies that described a fluoroless technique for ureteroscopy. Mandhani et al. 17 showed that complete clearance of distal ureteral stones, below the sacroiliac joint, could be achieved without the use of fluoroscopy in 99 out of 110 patients. Their study also showed that fluoroless balloon dilatation of the distal ureter can also be achieved under direct vision. Tepeler et al. performed ureteroscopy in 93 consecutive patients, avoiding immediate intraoperative fluoroscopy in 92% of their patients, but obtained a kidney, ureter, and bladder (KUB) film on postoperative day 1 in all patients with an estimated radiation dose of 1.1 millisievert (mSv). However, they did not perform flexible ureteroscopy in any of the patients. 18 In another study, Hsi and Harper avoided the need for a KUB by using two taps of fluoroscopy at the time of the procedure, thus getting real-time evaluation of stent placement and reducing the median effective dose to 0.05 mSv. 19 In their technique, no fluoroscopy was used for the ureteroscopy, but limited fluoroscopy was required for stent placement. Although their study continued on the logical progression of dramatically reducing radiation, the study did not provide follow-up for the patients or any comparison with conventional ureteroscopy patients.
These previous innovative studies have significantly reduced radiation exposure to patients. Our technique of completely fluoroless treatment of renal and ureteral stones further expands the potential application of fluoroless ureteroscopy. Our study is the first to perform proximal and distal ureteroscopy, renal mapping, and stent placement without any form of image guidance. Our series also demonstrates equal stone-free rates between our two cohorts (92%) despite the fluoroless patients having a significantly larger stone burden 91.53 vs 56.58 mm2. Thus, this study demonstrates that a fluoroless technique is feasible and effective for treatment of both ureteral and renal stones.
One alternative to the use of fluoroscopy during ureteroscopy is the use of intraoperative ultrasound. 20 A prospective study by Deters et al. 21 randomized 50 patients who had been previously stented for symptomatic ureteral stone to either ultrasound or fluoroscopy-guided ureteroscopy. There was no difference in stone-free rates, operative time, or complication rates between the two study groups. However, ureteral stents may be difficult to identify using ultrasound. In addition, intraoperative ultrasound requires a unique skill set not possessed by all urologic surgeons. Finally, intraoperative ultrasound may require instruments and personnel not always available in the operating room. There are certainly some potential benefits of performing a completely fluoroless ureteroscopy. Because of the inherent dangers associated with radiation exposure, many institutions have incorporated an ALARA (as low as reasonably achievable) protocol for their medical procedures requiring radiation. We routinely have the fluoroscopy machine available in the room in the event that imaging should be required. With further experience and refinement of techniques, it is possible that eventually the C-arm technician and machine would not be required. This would potentially simplify these surgical cases and reduce their cost.
Another potential benefit of a fluoroless technique is a reduction in the risk of back pain and other skeletal-related disorders for the surgeon and staff. Surgeons who wear heavy lead aprons for protection from radiation exposure are known to have an increased incidence of spinal complaints. 22 Ross et al. coined the term, interventionalist's disc disease, when they found that cardiologists are at an increased risk of axial skeletal problems related to lead apron use. Interventionalists who wore lead aprons for longer periods of time had a substantially greater incidence of skeletal complaints with more cervical spine complaints, more multiple-level disc herniations, and more missed days from work due to back pain compared with those wearing aprons for shorter periods of time. 22 Performing procedures in an entirely fluoroless manner means that the surgeon is not required to wear lead shielding to protect against ionizing radiation.
This study has some limitations. One limitation of this article is that it is retrospective, and therefore unable to describe the patients in whom the fluoroless technique was converted to image guidance. There was also a significant difference in the amount of stone in the groups, with a larger stone burden in the fluoroless group 91.53 vs 56.58 mm2 (p=0.042). There was also a higher incidence of renal stones (p=0.002) in the fluoroless group. Although these differences do exist, both differences make the fluoroless group a clinically more challenging cohort.
We continue to revise and adjust our indications for a fluoroless approach as our experience increases. This technique is not appropriate for all patients. Patients who currently would not meet fluoroless criteria in our institution include those with ureteral strictures, entombed stents, significant anatomic abnormalities, and tightly impacted stones. In our center, we do not routinely employ ureteral access sheaths and subsequently this study does not determine the safety of the fluoroless technique when using a ureteral access sheath. If the surgeons do not feel that they can adequately endoscopically map the entire collecting system to ensure complete fragmentation of all stones, they should not hesitate to employ fluoroscopy.
While this study shows favorable patient outcomes in fluoroless ureteroscopy, it does not address the additional stresses that may be placed on physicians performing these procedures. Certainly, the fluoroless technique is a significant departure from the conventional technique and it should not be attempted until the surgeon has extensive experience with low radiation protocols for ureteroscopy. The intent of this study is not to suggest that fluoroless ureteroscopy should be routinely performed in all patients. Rather, the intent of this study was to determine whether ureteroscopy without fluoroscopy or other image guidance was feasible and whether it could be safely performed in carefully selected patients. Rigid application of this technique to all patients by surgeons unfamiliar with the technique could result in patient harm. In addition, even experienced surgeons should have a low threshold for employing fluoroscopy if any ambiguity is encountered. Although this cohort of fluoroless ureteroscopies was sequential, during this same period some more complicated cases were performed using fluoroscopy, introducing a potential selection bias for the less complicated cases. We strongly recommend that if there is any ambiguity in the case or uncertainty, the surgeon should not hesitate to employ fluoroscopy using a low-dose protocol. Future prospective randomized trials will be needed to delineate optimal patient candidates and to assess the risk–benefit ratio associated with specific patient profiles and surgeon experience levels. In addition, we will continue to maintain a low threshold for converting to a fluoroscopy-guided technique in the event of any uncertainties or intraoperative concerns.
Conclusion
This series represents the initial description of ureteroscopic lithotripsy without fluoroscopy or other form of image guidance performed in the entire upper tract with a comparison with a cohort of conventional ureteroscopy cases. This study demonstrates that ureteroscopy without fluoroscopy is technically feasible and can be performed safely in carefully selected patients.
Footnotes
Disclosure Statement
No competing financial interests exist.