
Abstract
Background and Purpose:
Patients with urinary tract abnormalities are at an increased risk of stone formation. Percutaneous nephrolithotomy (PCNL) plays an important role in the treatment of this patient population; however, outcomes are less well defined compared with patients with normal urinary tract anatomy. Our objective was to evaluate the influence of urinary tract abnormalities on intraoperative and postoperative outcomes with PCNL.
Patients and Methods:
We report on a single-center prospective database of 2284 consecutive PCNLs in 1935 patients from 1990 to 2012. For the purposes of this analysis, patients were categorized by the presence or absence of a urinary tract abnormality. Multivariable analyses were used to identify independent predictors of the length of hospital stay, operative time, complications, and residual stones at discharge and 3 months.
Results:
A urinary tract abnormality was present in 14.4% (n=330) of the cohort. On univariable analysis, patients with urinary tract abnormalities were more likely to present with urinary tract infection (28% vs 19%, P<0.001) and less likely to present with hematuria (13% vs 19%, P<0.02). On multivariable regression, a urinary tract abnormality was predictive of residual stone at discharge, need for a secondary procedure, but did not increase the risk of residual stone at 3 months or the development of complications. Operative time and hospital stay were only moderately prolonged.
Conclusion:
Patients with urinary tract abnormalities who undergo PCNL have a higher risk of residual stones at discharge and need for secondary procedures, but comparable complication rates, operative time, and hospital stay.
Introduction
U
Several small studies have demonstrated safe PCNL in these contexts with overall stone-free rates ranging from 75% to 93%. 2,9 –19 The largest reported cohort was based on the Clinical Research Office of the Endourological Society (CROES) PCNL Global Study database, which included 5542 patients who underwent PCNL of whom 3.6% had renal anomalies. The authors report similar unadjusted stone-free rates at 30 days for patients with renal abnormalities (76.6%) or normal anatomy (76.2%). 20 Likewise, they reported similar frequency of complications and a longer operative time among patients with renal abnormalities.
The impact of urinary tract abnormalities on outcomes of PCNL in the context of potential confounding factors has not been described. The objective of our study was to describe differences in the presentation, operative course, and postoperative follow-up of patients with and without urinary tract abnormalities who underwent PCNL at a single tertiary endourologic center. In addition, we aimed to evaluate the independent predictive impact of urinary tract abnormality on several key outcomes of PCNL: Residual stone, operative time, requirement for ancillary procedures, length of hospital stay, and incidence of perioperative complications.
Patients and Methods
We conducted a retrospective analysis of a large, prospectively collected observational database from a single academic tertiary referral center for all consecutive PCNLs performed between July 1990 and December 2012. The Ethics Review Board of Western University (103440) and Lawson Health Research Institute (R-13-056) approved our data collection protocol.
Data collected included patient characteristics (age, sex, presenting symptom, comorbidities, presence and type of urinary tract abnormality); stone characteristics (stone burden, location), operative characteristics (operative time, location and number of tracts, stent and nephrostomy tube placement); and outcomes (incidence of residual stone at discharge and 3 months, occurrence of secondary procedure, perioperative complications).
Patient comorbidities were identified by preoperative medical assessment. These were assessed dichotomously as either having or not having any of the following: Hypertension, diabetes; cardiac, pulmonary, orthopedic, gastrointestinal, thyroid, neurologic disorders; gout, or renal failure. Urinary tract abnormalities were identified on cross-sectional imaging and included bifid renal pelvis, caliceal diverticulum, ureteral duplication, ectopic kidney, horseshoe kidney or malrotation, previous partial nephrectomy, urinary diversion, or neurogenic bladder (Table 1). Stone burden was calculated as the sum of (length×width×pi)/4 for each stone present and then categorized into the following quartiles (<500 mm2, 500 to 1000 mm2, 1001 to 1500 mm2, >1500 mm2) for the purposes of analysis. 21
Patients with multiple urinary tract abnormalities were only counted once in total.
Perioperative complications assessed included minor bleeding, need for blood transfusion, embolization, fever >38.5°C, urosepsis, urine leak, pneumothorax, hydrothorax, pyelocutaneous fistula, colon perforation, thromboembolic event, or death. Complications were categorized according to the Clavien classification system and analyzed as a dichotomous outcome. 22
PCNL was performed with patients in the prone position. Single-stage PCNL with renal access obtained using fluoroscopic guidance in the operating room was used in the majority of cases (97%). On occasion, tracts were placed in the interventional radiology department using ultrasonography or CT guidance (3%). The reasons for radiology obtained access included: Inability to access the ureter in a retrograde fashion for urinary tract opacification or when anatomic factors necessitated ultrasonography or CT-guided percutaneous access. Our technique of PCNL has previously been published in detail. 23
The primary end points were incidence of residual stone at discharge defined as presence of stones >3 mm (determined by various imaging modalities including plain radiography and ultrasonography, 52%; nephrotomography, 32.5%; CT 9.1%; nephrostography or intravenous urography (IVU), 6.4%); and at 3 months (determined by plain radiography or ultrasonography, 86.3%; IVU, 7.9%; CT, 4.2%; nephrotomography, 1.6%). Secondary end points included the requirement for a secondary procedure (second-look nephroscopy, ureteroscopy, shockwave lithotripsy [SWL]), operative time, length of hospital stay, and incidence of complication.
Statistical analyses were performed using SPSS v.20 (IBM Corp., Armonk, NY). Univariate analyses were assessed using chi-square for categorical variables and Student t test for continuous variables. Multivariate logistic regression was used to assess the independent influence of urinary tract abnormality on the incidence of residual stones at discharge and 3 months, requirement for secondary procedure, and incidence of complications. Multivariate linear regression was used to describe the contribution of a urinary tract abnormality on operative time and length of hospital stay. Secondary post hoc univariable and multivariable regression analyses were additionally conducted using specific urinary tract abnormalities as independent variables for each outcome of interest. These post hoc analyses were conducted in an effort to further clarify possible associations with specific abnormalities and should be considered exploratory.
Results
A total of 2283 consecutive PCNLs in 1935 patients were included for analysis of which 330 PCNLs were performed on 276 patients with urinary tract abnormalities. The average age of the entire cohort was 53.6±15.2 years with a male predominance (56%) (Table 2). Patients with urinary tract abnormalities tended to present more frequently with urinary tract infection (28% vs 19%, P<0.001) (Fig. 1) and at a slightly younger age (54.1 vs 51.0 years, P=0.001). Medical comorbidities were common, affecting 45% of the cohort, but were more common among patients with urinary tract abnormalities (52% vs 44%, P=0.007). This difference was largely driven by increased neurologic, orthopedic, and gastrointestinal conditions (Table 3).
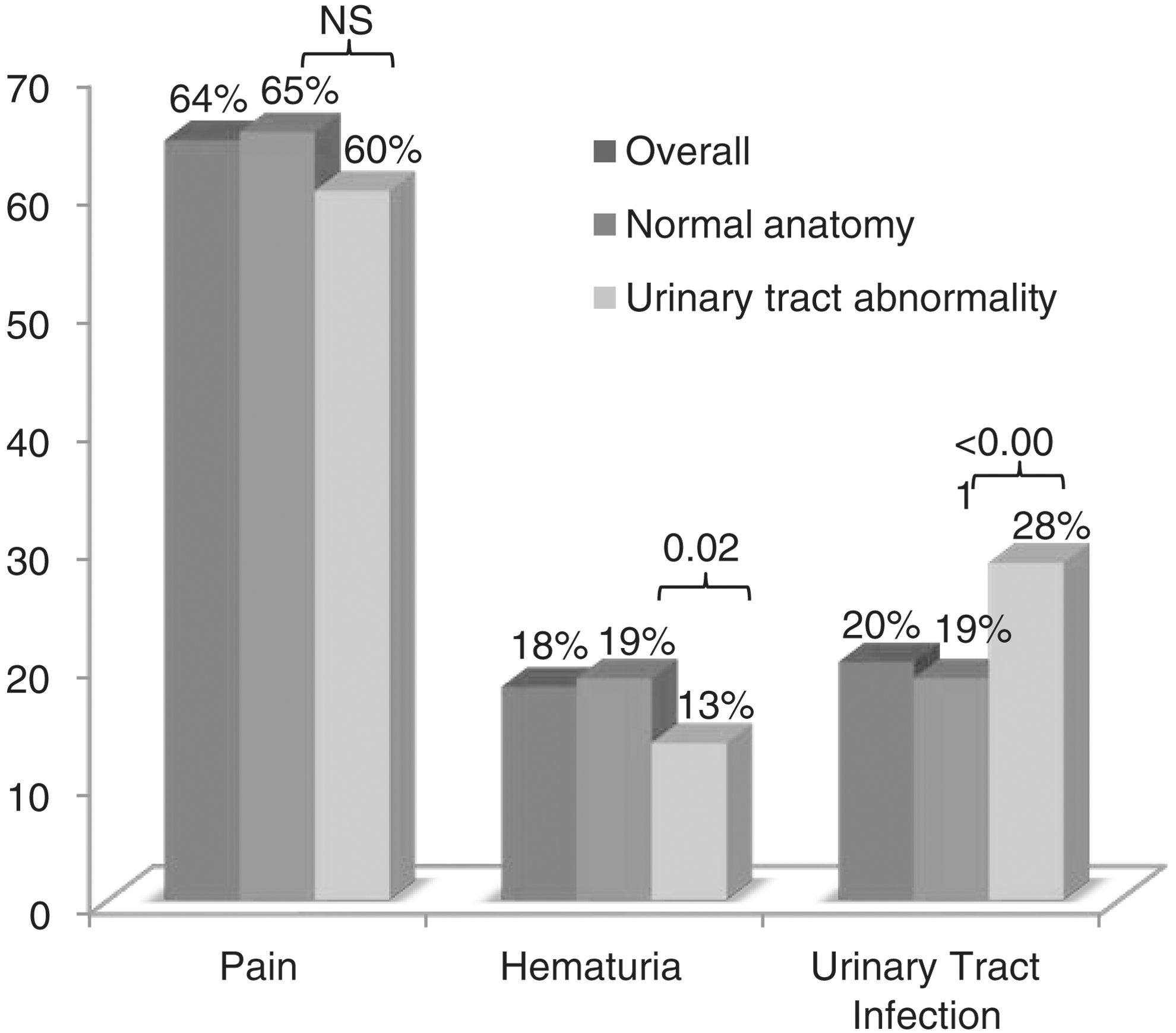
Presenting symptom (as a %).
Based on a subset of cases for which stone location was available, n=2135.
Based on a subset of cases for which stone analysis was available, n=1739.
SD=standard deviation; BMI – body mass index.
Patients with multiple comorbidities were only counted once.
Stone size and configuration were similar between both groups with a comparable incidence of complete staghorn and partial staghorn (Fig. 2, Table 2). Patients with abnormalities were more likely to have infectious stones compared with patients with normal anatomy. Likewise, patients with urinary tract abnormalities were more likely to need an upper pole access (27% vs 10.5%, P<0.001) and to have the tract placed by an interventional radiologist (9.2% vs 1.6%, p<0.001) but did not need a greater number of tracts (Table 4). When comparing tract placement by specific urinary tract abnormality, patients with urinary diversions (26.6% vs 2.1%, P<0.001) and neurogenic bladder (17.6% vs 2.3%, P=0.009) were more likely to need an access placed by an interventional radiologist.
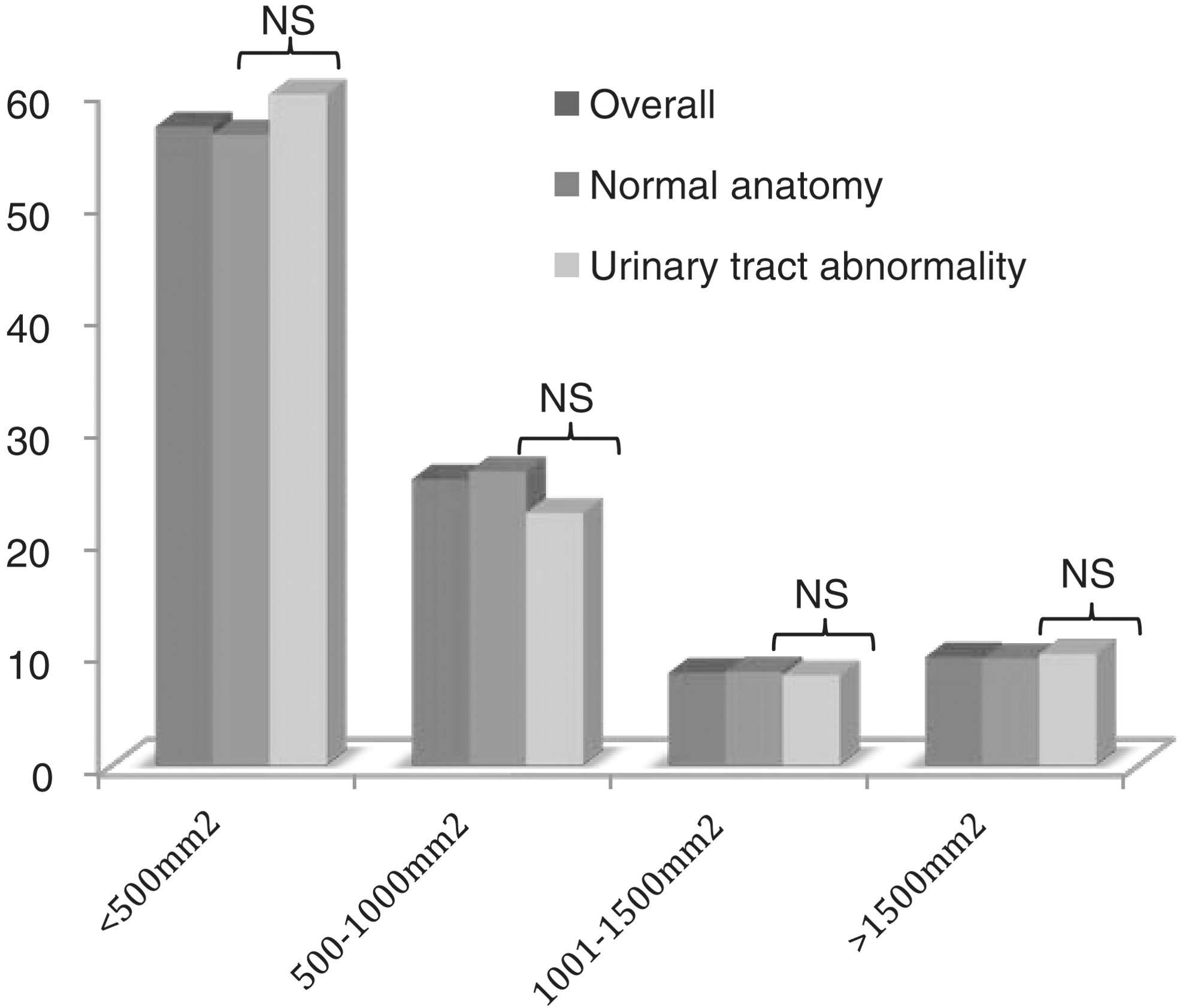
Distribution of total stone burden (as a %).
Based on subset of patients for whom data were available (n=2279).
Based on subset of patients for whom data were available (n=2230).
Based on subset of patients for whom data were available (n=688).
Based on subset of cases for which these data were available (n=2269).
Based on subset of cases for which these data were available (n=677).
Overall, on univariable analysis, surgical outcomes and complications were similar between the two groups (Tables 5 and 6). Patients with urinary tract abnormalities had a modestly longer hospital stay and needed significantly more secondary procedures (25.1% vs 19.7%, P=0.02). Additional procedures were predominantly second-look PCNL, with no significant differences in the need for secondary ureteroscopy or SWL. Of the patients with available imaging at discharge (n=2128), patients with urinary tract abnormalities were significantly more likely to have a residual stone (17.2% vs 12.7%, P=0.03). This difference was not observed among patients with evaluable imaging at 3 months (n=1694), however.
Based on subset of patients for whom data were available (n=2284).
Based on subset of patients for whom data were available (n=2282).
Based on subset of patients for whom data were available (n=2011).
Based on subset of patients for whom data were available (n=1233).
Based on subset of patients for whom data were available (n=2128).
Based on subset of patients for whom data were available (n=1694).
PCNL=percutaneous nephrolithotomy; SWL=shockwave lithotripsy.
On multivariable analysis, urinary tract abnormality remained an independent predictor of residual stone at discharge, odds ratio (OR) 1.64 (1.15, 2.34) P=0.007 (Table 7), but not at 3 months follow-up, OR 1.39 (0.88, 2.21) P=0.16. Regarding secondary outcomes, a urinary tract abnormality was found to be an independent predictor of the need for a secondary procedure, OR 1.55 (1.14, 2.10) P=0.005, operative time, OR 6.2 (1.9, 10.6) P=0.005, and hospital stay, OR 0.43 (0.13, 0.72) P=0.005 (Tables 8 –10).
Additional post hoc secondary analyses were conducted to evaluate whether specific urinary tract abnormalities were predictive of incidence of residual stone. On univariable analysis, the presence of urinary diversion and ureteral duplication modestly increased the odds of residual stone. When controlling for other known predictors of residual stone, however, presence of urinary diversion or ureteral duplication both dropped out of the multivariable model.
Discussion
Patients with urinary tract abnormalities who are candidates for PCNL are a common patient group encountered by endourologists, whose condition is challenging to manage and who are relatively understudied. At our center, the incidence of a urinary tract abnormality was considerably higher (14.4%) than comparable series (3.6%). 20 This difference may be primarily attributed to our broad definition of a urinary tract abnormality, which aimed to capture anatomic factors that could define a significant subset of the population and have an impact on patient-relevant outcomes. Second, our population reflects the tertiary nature of our practice in which patients with complex stone disease are referred from a large catchment area, thus concentrating the proportion of patients with urinary tract abnormalities. In this context, we sought to evaluate the impact of renal anomalies on the outcomes of PCNL at a single site, using a standardized operative approach to this patient population.
Our study revealed that patients with a urinary tract abnormality had a higher incidence of residual stones at discharge (17.2% vs 12.7%, P=0.03) but this difference could no longer be detected at 3 months (10.5 vs 9.5%, P=0.6). Multivariable modeling confirmed the independent association between a urinary tract abnormality and residual stone at discharge, which could no longer be detected at 3 months.
There are several potential explanations for this observation. Because it appears that the prevalence of residual stone continues to decline from discharge to 3 month follow-up, it is possible that patients with urinary tract abnormalities are more likely to harbor residual stones at discharge that pass spontaneously. Alternatively, our observation may be explained by differential loss to follow-up. Given our tertiary referral base, many of our patients with complex conditions are treated at our site, then followed in their local community at 3 months. Overall, the incidence of residual stones reported in our study is comparable to other series of patients with renal abnormalities. 15 –17,19,20 Additional studies that include longitudinal follow-up and a standardized measure of stone recurrence are needed to determine the impact of PCNL among patients with urinary tract abnormalities in terms of eliminating residual stone burden.
The presence of a urinary tract abnormality increases the risk of undergoing additional procedures—most commonly, second-look nephroscopy, before discharge. This may be related to the increased complexity of obtaining access in the setting of abnormal anatomy, or a lower threshold for performing secondary interventions and considering a patient stone free. 2,15,16,19 This hypothesis is supported by the observation that patients with urinary tract abnormalities were more likely to need ultrasonography or CT-guided access performed by an interventional radiologist. In the CROES study, Osther and coworkers 20 noted a higher failure rate for the procedure (5% vs 1.7%, P=0.001) among patients with anomalies, which is most commonly related to difficulties with access.
We have shown that urinary tract abnormalities increase the risk of needing a secondary procedure with PCNL. Other factors including stone size and number of tracts also increase the risk of a secondary procedure and to a greater extent in our series. Interpreted together, this implies that urinary tract abnormalities may increase the need for a secondary procedure but to a relatively limited extent.
We have also demonstrated that the presence of a urinary tract abnormality is independently predictive of increased operative time and accounts for approximately 6 additional minutes per case. This is similar to the observation by Osther and associates 20 who reported an additional 12 minutes of mean operative time on univariable analysis, P=0.037. In both cases, we believe that the statistical significance of this observation is the result of analyzing a continuous outcome in a large cohort and is of little clinical implication. When accounting for other factors, such as stone burden, staghorn configuration, and number of tracts, the additional operative time associated with a urinary tract abnormality would seem inconsequential (Table 9).
We have demonstrated that the presence of a urinary tract abnormality impacts length of stay on multivariable analysis. A similar observation has been reported by Desai and Jasani, 7 among patients with ectopic kidneys; however, several other series have failed to show this association. 14 –17 When considered in conjunction with other relevant predictors of hospital stay, such as stone burden, staghorn configuration, number of tracts, and patient comorbidities, this information can be used to inform resource allocation and counsel patients regarding their hospital course.
Complications occurred in 18% of our patients, and the majority were minor according to the Clavien system. The presence of a urinary tract abnormality did not predict occurrence of complications on multivariable analysis. This finding is consistent with previous series, 7,14 –17,20,24 –29 and therefore we conclude that PCNL appears to have a favorable safety profile for patients with urinary tract abnormalities.
Conclusion
Overall, patients with urinary tract abnormalities who undergo PCNL are more likely to undergo a secondary intervention and have a longer length of hospital stay compared with patients without urinary tract abnormalities. There is no evidence that the presence of a urinary tract abnormality, as defined in our cohort, increases morbidity from PCNL when performed at a specialized tertiary endourologic center. The incidence of residual stone may be higher among patients with urinary tract abnormalities at discharge, but the impact of this observation on long-term stone-free rate or stone recurrence remains unclear.
Footnotes
Disclosure Statement
No competing financial interests exist.