
Abstract
Background and Purpose:
Treatment of patients with prostate cancer has evolved considerably in the last decade, especially in terms of minimization of the negative impacts on erectile function and continence to ensure good quality of life for treated patients. New surgical devices, such as dissectors and hemostatic scalpels, allow precise definition of the surgical field with finer dissection of the anatomic structures, with subsequent reductions in operative times and better oncologic and functional outcomes. Although monopolar scissors (MS) are still widely used, radiofrequency (RF) and ultrasound (US) scalpels have been introduced recently in laparoscopic radical prostatectomy (LRP). Despite the widespread use of these scalpels, however, few studies have compared these devices in terms of oncologic and functional outcomes after radical prostatectomy. The present study aimed to prospectively assess the impact of MS, RF, and US scalpels on margin status at apex, and recovery of urinary continence and erectile function in patients undergoing extraperitoneal LRP.
Patients and Methods:
A total of 150 men were prospectively enrolled between September 2009 and April 2013 and postoperatively evaluated for continence and clinical factors.
Results:
There were no differences in terms of operative times (P=0.9433), blood loss (P=0.9681), apical margin positivity (P=0.3965) or postoperative hospital stay (P=0.9257) among the groups. Moreover, no differences in the functional outcome scores, as evaluated by the International Consultation on Incontinence self-administered Questionnaire, at 1, 3, and 6 months postsurgery were observed.
Conclusion:
Our study represents the first evaluation of continence recovery in LRP with respect to different devices used for prostatic apex dissection. We found that the oncologic, functional, and operative outcomes were similar between these different devices during LRP, with no scalpel demonstrating superiority in continence recovery.
Introduction
T
It is commonly believed that optimal dissection of the prostatic apex with preparation of a urethral stump of a greater length is associated with earlier continence recovery. 2 For this reason, it becomes necessary to perform the dissection as close as possible to the apex of the prostate. This is associated with an increased risk of positive surgical margins, however; therefore, the choice of the specific devices used during the surgical procedure becomes critical to ensure a clear field of dissection, to reduce mechanical manipulation, to avoid excessive bleeding, and to obtain the most precise section of the urethra.
Although monopolar scissors (MS) are still widely used to cut the Santorini plexus and to dissect the urethra from the apex after having passed a hemostatic stitch on the plexus itself, radiofrequency (RF) and ultrasound (US) scalpels have been recently introduced in LRP and demonstrated to be effective for achieving both dissection and hemostasis, and for minimizing the operative time and perioperative blood loss. Despite the widespread use of these scalpels in laparoscopy, there are currently few studies comparing these devices in terms of oncologic and functional outcomes after radical prostatectomy (RP). The present study aimed to prospectively assess the impact of MS, RF, and US scalpels on margin status at apex, and recovery of urinary continence and erectile function in patients undergoing extraperitoneal LRP (ELRP).
Patients and Methods
A total of 150 men were prospectively enrolled between September 2009 and April 2013 after providing written informed consent. Patients were recruited at the Urology Unit of Sapienza University of Rome. The study was conducted in accordance with the Declaration of Helsinki and was approved by the local Medical Ethical Committee (ASL LT CE approval n. 2009/78690). All patients had a histopathologic diagnosis of prostatic adenocarcinoma, as determined by transperineal ultrasound-guided biopsy after preliminary clinical evaluation involving digital rectal examination (DRE) and assessment of serum prostate-specific antigen (PSA) levels (total PSA, free-PSA, and ratio). The clinical stage of the disease was determined in all patients by abdominopelvic magnetic resonance and whole-body bone scintigraphy.
All patients who met the following preoperative criteria, as defined in the European Association of Urology guidelines, 3 underwent bilateral nerve-sparing ELRP: PSA ≤10 ng/mL, life expectancy >10 years, no extraprostatic extension, negative DRE, no more than two positive cores per lobe, and a primary Gleason pattern=3.
Postoperative (90 and 180 days post-ELRP) evaluation of continence was performed for all patients using the self-administered International Consultation on Incontinence Questionnaire–Urinary Incontinence Short Form, a condition-specific, quality of life questionnaire developed by the International Continence Society for patients with urinary incontinence. 4 The presence of urethral strictures was excluded by flexible urethroscopy at the 3-month follow-up.
After a stratified randomization to control for baseline covariates was made, the patients were randomly assigned, using a computer table generation of random numbers, to group A (RF; n=50), group B (US; n=50), or group C (MS; n=50). All patients underwent ELRP under general anesthesia. In group A, the dissection of the prostatic apex was performed with the use of an RF scalpel (LigaSure-8 generator with LigaSure RF scalpel, vessel-sealing system V 5-mm forceps; Valley Lab, Tyco Healthcare®). In group B, the dissection was performed with the use of a US scalpel (UltraCision Harmonic scalpel generator 300 with 5-mm 36p Harmonic Ace forceps; Ethicon Endo-Surgery, Inc.®), and in group C, the dissection was performed using MS (Aesculap, Inc.®). The surgeons performed all surgeries using the bilateral standard (interfascial) nerve-sparing technique, as originally described by Stolzenburg and associates. 5
RF, US, and MS were used to seal the pelvic lymphatic tissues and dorsal vein complex and to dissect the bladder neck, vasa deferentia, seminal vesicles, lateral pedicles from the base to the apex of the prostate, and the puboprostatic ligaments.
Regarding the dissection of the prostatic apex, in group A, the surgeon performed the procedure using an RF scalpel without any previous hemostatic stitches, and the urethra was cut using cold blade scissors.
In group B, the surgeon initially sutured the dorsal vein complex with a 3-0 barbed self-cinching suture (Filbloc-, Assut® Europe SPA, Magliano dei Marsi–AQ, Italy) and dissected the prostatic apex using a US scalpel until getting to the urethral stump, which was subsequently cut using cold blade scissors. In group C, the surgeon sutured the dorsal vein complex similar to that in group B, and then dissected the prostatic apex from the urethral stump using an MS scalpel; the urethra was cut with cold blade scissors. Urethrovesical anastomosis was performed as described by Simone and colleagues. 6
Postoperatively, the days of catheterization, presence of positive margins at the prostate apex, and the recovery of postoperative continence were evaluated. The catheters were always removed after a cystography control to ensure the absence of any leakage.
All patients were clinically evaluated 15 and 30 days postsurgery. Patients who did not spontaneously recover continence at the first evaluation (15 days postoperatively) underwent a pelvic floor rehabilitation protocol (three sessions/week, up to 8 weeks).
We therefore performed a retrospective analysis of these prospectively collected data. To achieve this goal, statistical analysis was performed to compare the self-administered questionnaire scores using the Student t test and SPSS software (version 12.0; SPSS Inc., Chicago, IL). P values <0.05 were considered statistically significant.
Results
Patient age, PSA levels, clinical stage, body mass index (BMI), baseline urinary function, and perioperative data were similar in all groups (Table 1).
RF=radiofrequency; US=ultrasound; MS=monopolar scissors; SD=standard deviation; PSA=prostate-specific antigen; BMI=body mass index.
Focusing on the intraoperative data, there were no differences regarding the operative times (mean: 155.8±29.3 min; range: 108–202 min) and blood loss (mean 184.6±25.6 mL; range: 157–223 mL) between the groups (P=0.9433).
Surgical complications were evaluated based on the Clavien classification system, 7 with 8%, 10%, and 8% grade I, II, and III complications, respectively, observed for group A; 8%, 12%, and 10%, respectively, for group B; and 10%, 14%, and 8%, respectively, for group C (Table 2).
RF=radiofrequency; n=number; US=ultrasound; MS=monopolar scissors; pts=patients.
The bladder neck stricture rate was 4% (two patients) in group A, 6% (three patients) in group B, and 4% (two patients) in group C. All these patients were treated with transurethral incision of the bladder neck within 3 months postsurgery. The urinary leakage rate was 4% (two patients) in each group, and all these patients were treated with 8 weeks of pelvic floor rehabilitation. One patient in group B was treated also with artificial sphincter implantation.
Similar to the overall surgical margin positivity, there were no significant differences between the groups in terms of apical margin positivity, with 3, 1, and 1 patients in groups A, B, and C, respectively, reporting positive apical margins (P=0.4424, Fig. 1).
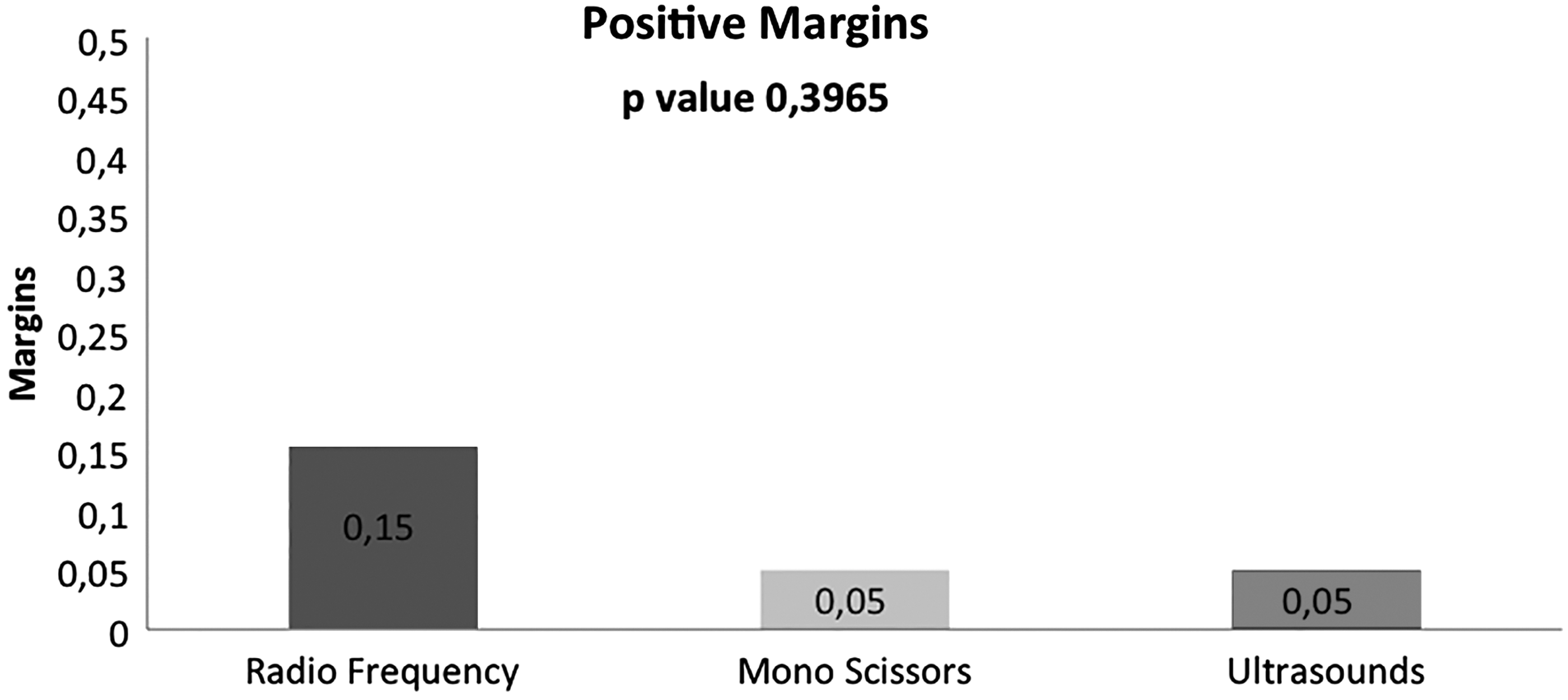
Differences between the groups in terms of apical margin positivity.
The mean number of days of catheterization was 6.69, 8.25, and 8.86 days in groups A, B, and C, respectively (Fig. 2). Moreover, no differences regarding the functional outcomes evaluated by the ICIQ scores at 1, 3, and 6 months postsurgery were observed. At the 3-month follow-up, the median ICIQ scores were 6, 6.57, and 5.36 in groups A, B, and C, respectively (P=0.7456), whereas at the 6-month follow-up, they were 3.38, 5.14, and 2.73, respectively (P=0.1782, Fig. 3).

Mean number of days of catheterization.

International Consultation on Incontinence Questionnaire (ICIQ) scores at 3 and 6 months after operation.
Discussion
The increased number of young men with a diagnosis of early-stage prostate cancer has resulted in a growing need to preserve continence and erectile function after RP. Substantial attention is currently being paid to an early urinary continence recovery after RP, 8 because this remains the most feared complication. 9,10 As a result, several technical modifications have been attempted to achieve better postoperative functional outcomes. Because the incidence of incontinence at 1 year postoperatively is relatively low, efforts are instead being directed at achieving an earlier recovery. Factors negatively affecting postoperative urinary continence have been previously described in the literature, and include increasing age, shorter preoperative and postoperative urethral length, anastomotic strictures, obesity, low surgeon volume, vesicourethral anastomosis location below the pubic symphysis as seen in postoperative cystography, and previous prostate surgery. 11,12
Several surgical modifications have been described in the literature, including preservation of the urethral rhabdosphincter length, posterior reconstruction of the Denonvilliers musculofascial plate, preservation of the bladder neck and internal sphincter, bladder neck intussusception, posterior and anterior fixation of the urethra, bladder neck mucosal eversion, preservation of the puboprostatic ligaments, preservation of the endopelvic fascia, and several combinations of these. 13 –16 Techniques reconstructing the pelvic anatomy have been reported to achieve mixed results, 17 whereas surgical modifications aimed at preserving the natural urinary continence mechanism appear to effectively promote early recovery of continence. 18 Simone and coworkers 6 reported favourable continence recovery outcomes describing a ‘‘single knot–single running’’ suture vesico-urethral anastomosis with posterior musculofascial reconstruction in 155 patients who underwent laparoscopic transperitoneal RP. 6 Rocco and colleagues 17 popularized rhabdosphincter posterior reconstruction during RPs. This technique reconstructs the posterior musculofascial plate by suturing the median raphe of the urethra to the remnants of the Denonvillier fascia posterior to the bladder. The authors conclude that this reconstruction allows restoring anatomic length of the rhabdosphincter and posterior support by fixing the structure into its natural position.
The precise etiology of postprostatectomy incontinence remains unknown. The reported incidence rates of urinary incontinence after RP range from 2.5% to 87.0%, and differ considerably according to the exact definition, follow-up duration, and surgical technique used. 19 There are many known causative factors for the occurrence of postprostatectomy incontinence, with a number of objective clinical characteristics, the surgical technique used, and the absence or presence of postoperative pelvic floor muscle therapy being the most important ones.
Yang and associates 20 tried to identify the risk factors associated with urinary incontinence after radical retropubic prostatectomy (RRP) in a total of 263 patients in their study. The authors reported that the continence recovery rates after RP were 14.8% and 94.7% at the 4- and 16-week follow-up sessions, respectively, and multivariate analysis showed that age (P=0.015), blood transfusion status (P=0.017), previous transurethral resection of the prostate (TURP) (P=0.006), and neoadjuvant hormonal therapy (P=0.005) were the most important independent risk factors for urinary incontinence. Accordingly, they concluded that optimized preservation of the urethral rhabdosphincter length, nerve sparing, and early postoperative functional exercises could improve urinary continence recovery.
In a recent literature review, Srivastava and coworkers 16 evaluated the technical advances aimed at optimizing continence recovery after robotic prostatectomy. Most of the authors who reviewed studies suggested that several technical nuances during robotic prostatectomy could result in earlier continence recovery without compromising any e oncologic outcome. The most important features appeared to be delicate tissue handling with surgical preservation of support structures and a complete restoration of the preoperative anatomy, and standardization in the assessment of continence recovery. Moreover, despite the bladder neck not directly contributing to voluntary continence, bladder neck preservation and reconstruction are two key surgical points. Curto and colleagues 21 reported a series of 425 men undergoing LRP with bladder neck sparing, with complete urinary continence achieved in 95% of the patients at 6 months. Moreover, Freire and associates 22 retrospectively compared 348 men undergoing RARP with bladder neck sparing vs 271 men undergoing standard RARP, and noted significantly improved urinary continence recovery at 4 and 24 months in the bladder neck sparing group.
Furthermore, urinary continence after RP may be directly correlated with postoperative urethral length. 23 Hammerer and Huland 24 used urodynamic evaluation and confirmed a significantly longer urethral length in continent compared with incontinent men after RRP. More recently, von Bodman and coworkers 25 performed an anatomic study measuring preoperative urethral length, urethral volume, and proximity of the levator muscle and membranous urethra by MRI in 967 men undergoing RRP. They found that urethral length, urethral volume, and an anatomically close relationship between the levator muscle and membranous urethra were all significantly positively associated with recovery of urinary continence at 6 and 12 months.
It has been speculated that the urethra is deeply involved in the development of incontinence because of the existence of the urethral sphincters, and, accordingly, Coakley and colleagues 26 reported that the duration of recovery of continence decreased as the membranous urethral length, as measured on MRI, increased. Multiple factors have been implicated in early continence recovery, including patient characteristics (age, BMI) and benign prostatic hyperplasia history (prostate volume, previous TURP), which cannot be modified and which can merely be considered to refine the indication for RP or to improve preoperative and postoperative counseling.
In the present study, we demonstrated that the use of RF, US, and cold scissors were similar with respect to operative time, blood loss, and postoperative hospital stay, while a shorter catheterization time was noted in the RF group. Moreover, blood transfusions are rarely needed, with only 11/150 patients needing blood transfusions in this study. In addition, in our case series, recovery of continence was reported by 71.7% of patients 3 months postoperatively, reaching 94.7% at the 6-month follow-up.
Regarding the extraperitoneal or transperitoneal approach, Eden and coworkers 27 have reported the superiority of the former with respect to operative time, hospitalization time, and recovery of continence. Few studies, however, have compared the functional outcomes of energy-free ELRP with those obtained using various hemostatic devices.
Gill and Ukimura 28 compared potency outcomes in 76 patients undergoing LRP using either the harmonic scalpel-based or energy-free technique. To our knowledge, however, there is only one previous study, which was conducted by our group, comparing the effects of different surgical devices with respect to dissection and hemostasis in ELRP. In our previous study, we compared the functional outcomes of RF and US during ELRP focusing on dissection of lateral spread into the neurovascular bundles. 29 To the best of our knowledge, the present study is the first prospective randomized study focusing on the LRP functional outcomes (i.e., early continence recovery) related to the use of different devices during apex dissection and urethral stump preparation.
Most surgeons choose the surgical device based on practical aspects, particularly their confidence with the instrument, its ergonomic features, and, consequently, its simplicity of use. Ideally, the preference of one device over another should first depend on technical aspects and objective data.
The LigaSure and UltraCision devices used here present different technical features. The LigaSure vessel-sealing device uses both electrical energy and pressure to liquefy and reform collagen and elastin in the vessel walls and tissues (up to 7 mm in diameter) to provide hemostasis. The device incorporates feedback control, which automatically terminates energy transmission once a seal has been achieved. In contrast, the UltraCision scalpel uses US technology to denature proteins within vessel walls and tissues (up to 5 mm thick), leading to coagulation. Both the LigaSure device and UltraCision scalpel have been demonstrated to be safe and effective in numerous studies, 30 –32 and both devices have been shown to reduce operative times and make the procedure easier for the surgeon.
The main limitation of this study is the relatively small sample size and the follow-up duration. A larger, multi-institutional analysis with a longer follow-up period is needed to assess other scalpel devices and to encourage surgeons to select a particular device based on an objective demonstration of its superiority.
Conclusion
Oncologic, functional, and operative outcomes are similar between MS and RF and US scalpels during LRP, with no device demonstrating superiority in terms of continence recovery. This is the first study in the literature focusing on continence recovery with respect to different scalpels used in LRP, and our findings confirm the efficacy and safety of these devices.
Footnotes
Acknowledgment
We would like to acknowledge the patients and their families for their willingness to collect questionnaire data.
Disclosure Statement
No competing financial interests exist.