
Abstract
Objective:
To evaluate if statin medications (3-hydroxyl-3-methylglutaryl coenzyme A [HMG-CoA] reductase inhibitors) improve either oncologic or renal functional outcomes for patients undergoing robot-assisted partial nephrectomy (RPN).
Patients and Methods:
Patients undergoing RPN between March 2008 and October 2013 were evaluated from a prospectively maintained database for statin usage. The rate of perioperative acute kidney injury (AKI), as defined according to the RIFLE criteria, and the progression of chronic kidney disease (CKD) were compared between users and nonusers. Oncologic outcomes and rate of progression were compared between users and nonusers.
Results:
One hundred four (31%) of 339 patients were on statin therapy preoperatively and continued this medication peri- and postoperatively. Statin patients were older and had higher rates of comorbidities, including coronary artery disease, diabetes, and hypertension (p<0.0001 for all).The rate of AKI in the statin (16%) and nonstatin patients (14%) (p=0.60) and CKD progression based on Kaplan–Meier estimates (p=0.57) were similar between both the groups. Subgroup analysis of the 271 (80%) patients with hilar clamping also had similar rates of AKI, in statin users 10% vs 12% in nonusers (p=0.50). Multivariate analysis of factors affecting CKD progression confirmed these findings. Oncologic progression was not affected by statin therapy (p=0.90).
Conclusion:
Statin medications do not appear to influence perioperative renal function following RPN, in either clamped or unclamped procedures. Continuation of these medications may be continued perioperatively, but any effect on renal functional or oncologic outcomes was not elucidated in this study.
Introduction
T
Several studies have discussed the fact that the 3-hydroxyl-3-methylglutaryl coenzyme A (HMG-CoA) reductase inhibitors (statins) may have a renoprotective effect for patients with either ischemic- or contrast-induced renal injury. 6 –8 In population-based studies, these are associated with decreased risk of acute kidney injury (AKI) and need for dialysis postoperatively. 9,10 Statins have noted antioxidant, anti-inflammatory, and antithrombotic effects and thus may assist in endothelial recovery. 11 Statin therapy has also been associated with improved oncologic outcomes in several different cancers, including colon, breast, and gynecologic cancers. 12 –14
We hypothesized that the use of statins may provide an improved early return of renal function, less long-term renal functional decline, or reduced oncologic recurrence in a consecutive cohort of patients undergoing RPN.
Subject/Patients and Methods
Patients who were on a statin medication undergoing RPN at our institution between March 2008 and October 2013 were identified. This was accomplished by querying our institutional review board approved prospectively maintained database evaluating preoperative medications. Patient charts were rereviewed to determine demographic data, operative parameters, renal and oncologic outcomes, and follow-up.
Surgical technique has been described in previous publications. 15 –17 We used a mostly a transperitoneal approach and infrequently retroperitoneal or single-incision procedures with the 4-arm daVinci Surgical System (Intuitive Surgical, Mountain View, CA). Subtle changes are often made in technique, based on tumor and patient characteristics. 15,16 Intraoperative surgeon-controlled ultrasound, indocyanine green dye with near infrared fluorescence imaging, and excision of tumor with sharp dissection using robotic scissors without electrocautery are some of the highlights of our technique. After anatomical identification and understanding the spatial relationship of the tumor to renal vasculature and the pelvicaliceal system, the decision to perform clamped or unclamped partial nephrectomy was at the discretion of the attending physician. Specimen extraction was performed after entrapment into an Endocatch I bag (Covidien, Mansfield, MA). Resident or fellow involvement in the case was based on experience and level of training at different steps of the procedure.
Perioperatively, all patients were continued on their home dosage of statin medications at their regular dosing interval. Patients were also maintained on any perioperative antihypertensive with the exception of diuretics or angiotensin-converting enzyme inhibitors or androgen receptor blockers. To assess the development of AKI, we assessed the lowest glomerular filtration rate (GFR) recorded in the perioperative period. We assigned patients as developing AKI if they had a 25% worsening of renal function at any time perioperatively (<14 days following the procedure) based on the RIFLE criteria. 18 We assessed the role of statin therapy in long-term renal function and oncologic outcomes. The risk of long-term chronic kidney disease (CKD) development defined as progression to de novo CKD stage III or greater, or increase from stage III to IV, or IV to V disease from base line.
Patients were followed routinely with office visits consisting of physical examinations, radiologic imaging of the chest and abdomen, and renal functional outcomes. Recurrence was defined as any abnormality in the renal parenchyma on postoperative imaging, appearance of a new pulmonary nodule on imaging, further renal cell treatment, or cancer found on completion nephrectomy specimen. Renal functional estimate was performed using the Chronic Kidney Disease Epidemiology Collaboration (CKD-Epi) equation. 19
Categorical variables were summarized as percentages. Continuous variables are displayed as a mean and standard deviation or median with an interquartile range as appropriate. The association between categorical variables and treatment groups was investigated by the chi-squared or Fisher's exact test. The parametric unpaired t-test or the analogous nonparametric test (Wilcoxon/Mann–Whitney test) was applied to evaluate differences for continuous variables between the statin and control group. Univariate analysis of risk factors for CKD development was created using proportion hazard analysis with patients censored at the time of CKD progression. All the analyses were carried out using JMP Version 10 (SAS International, Cary, NC).
Results
Out of 339 robot-assisted partial nephrectomies performed during the study period, 104 patients (31%) were included in this study (Table 1). Patients who were on statin therapy were older (65 vs 56 years, p=0.001) and had an increased rate of comorbities including coronary artery disease (CAD) (25% vs 7%, p=0.001), diabetes (38% vs 16%, p=0.001) or hypertension (88% vs 55%, p=0.001).
eGFR=estimated glomerular filtration rate.
Statin therapy was similar in both the AKI and non-AKI cohort (Table 2). Only the duration of ischemia (but not ischemia as a categorical variable) and preoperative GFR were different between the patients who experienced AKI following RPN. No patient developed progression to dialysis, either perioperatively or at any point postoperatively.
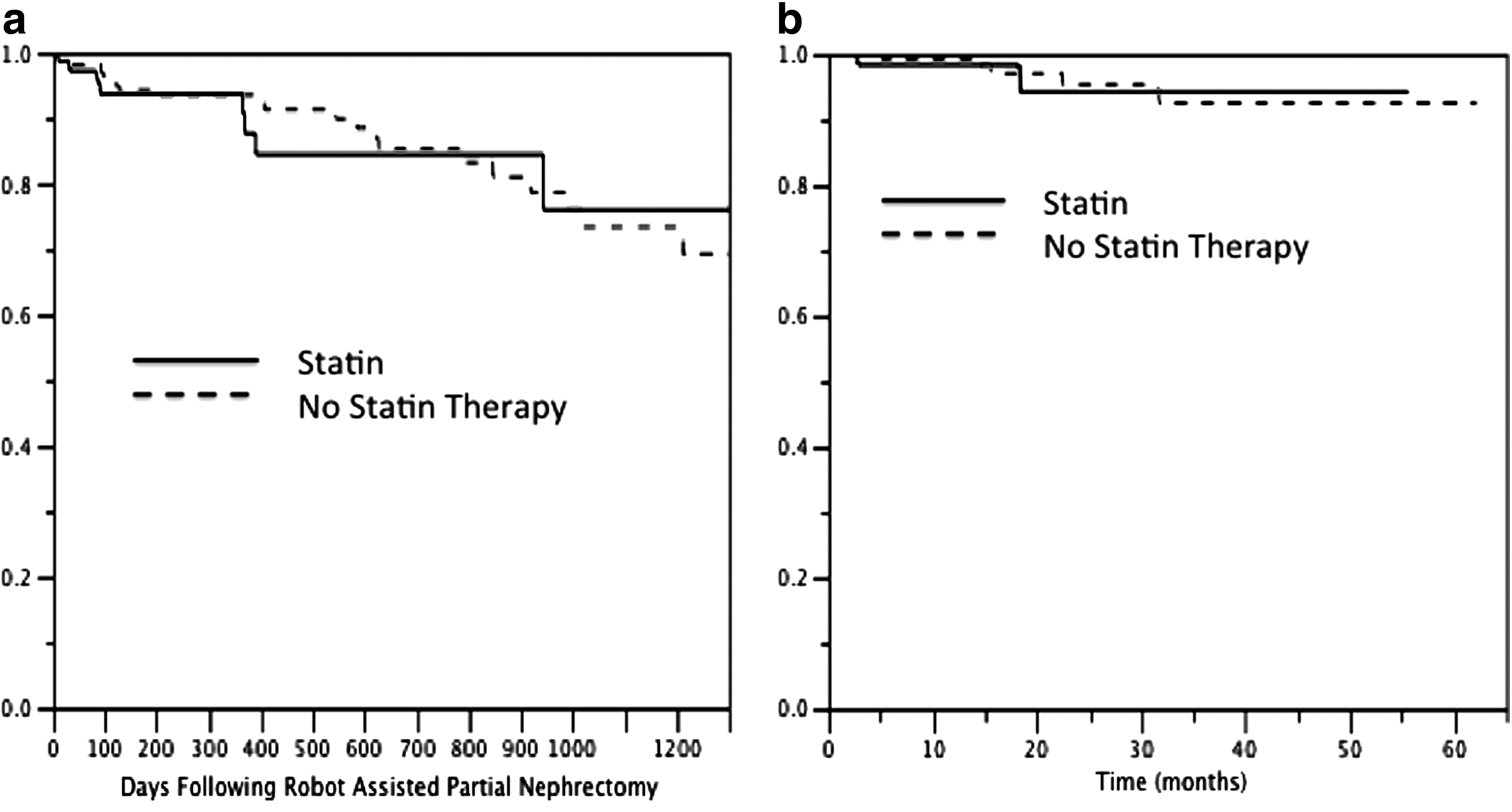
We evaluated long-term risk of CKD progression. Kaplan–Meier estimates of the development of de novo CKD stage III, or progression from stage III to IV or stage IV to V is noted. No patient developed the need for dialysis therapy. Figure 1a demonstrates the Kaplan–Meier estimate between statin users and nonusers with a p-value of 0.57. A proportion hazards model assessing risk factors for CKD progression is noted in Table 3. Increasing age and history of hypertension requiring medication were associated with long-term renal dysfunction. A high nephrometry score (as compared to low) was also found to increase the risk of long-term CKD progression. In the CKD analyses, we also excluded patients undergoing unclamped procedures and this did not alter the statistical significance associated with statin therapy. Data analysis with only the subset of CKD stage III or greater patients did not demonstrate any statistically significant association with long-term renal dysfunction for statin therapies either (data not shown).
95% CI=95% confidence interval; RR= relative risk.
An additional logistic regression analysis was included to assess the risk of a >25% decrease in estimated GFR at the last follow-up (Table 4). We noted that the predictors remained similar, with the exception that a history of CAD developed a statistically significant predictive value (relative risk [RR]: 2.64 95% CI: 1.17, 5.43). Statin medications once again did not predict long-term renal function.
Oncologic results of partial nephrectomy specimens are demonstrated in Table 1. Kaplan–Meier estimates for recurrence following RPN in patients on and off statin therapy are demonstrated in Figure 1b. Three- and 5-year progression-free survival was 93%. There were a total of seven episodes of cancer progression in the cohort, two with metastatic disease and five with loco/regional disease.
Discussion
RPN is becoming a standard modality for treatment of small renal masses with aims of preserving maximum nephrons and oncologic control. 20 The role that statin medications may play in the prevention of renal dysfunction and in prevention of cancer progression has been reported promisingly in the literature, which leads to this analysis.
Statin therapies have pleotropic effects many of which are not associated with lipid lowering. Statins may also play a role in renal perfusion and downregulate angiotensin receptors or decrease endothlin-1 production. These are vasodilators through endothelial nitric oxide release. Statins also act as an anti-inflammatory agent to decrease the toxic damage to the tubular cells by oxygen-free radicals and proinflammatory cytokines. This is potentially through an inhibition of tissue factor expression on macrophages and decreased nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) activation. All these may provide a beneficial effect following partial nephrectomy.
The role of statins in preventing contrast-induced nephropathy is well established. Li and colleagues performed a recent meta-analysis of statin therapy and noted a decreased risk of 49% of development of contrast-induced nephropathy in a short-term high-dose therapy. They did not note a significant difference in dialysis requirements, however, 6 Quintavelle and investigators found that atorvastatin was effective in preventing contrast-induced nephropathy. In their analysis, this protective effect was limited to patients with a GFR between 31 and 60. In this analysis, only 68 patients (20%) of the cohort had a GFR in this range. Subset analysis of these patients in our study did not demonstrate that there was a difference in long-term rates of progression of renal disease.
The mechanism of renal dysfunction associated with ischemia/reperfusion injury are due to a hypoxic injury and subsequent reactive oxygen species creation and subsequent inflammatory response. The pleotropic effects of statin therapy are proposed to assist in ameliorating each of these outcomes. Statins have demonstrated an ability to increase nitric oxide availability to cells. This occurs not only by directly increasing the endothelial nitric oxide synthase mRNA expression but also by providing an increase in tetrahydrobiopterin (BH4), which prevents uncoupled oxygen-free radical production. 21 The anti-inflammatory effects of statins include not only the NF-κB activation but also through inhibiting oxidation of low-density lipoprotein (LDL), which is known to be a potent atherogenic molecule and leads to a proinflammatory cascade. Statins also directly inhibit MHC-II expression and blocking of β2 integrin, which is necessary for leukocyte adhesion and costimulation. 21
In nonurologic surgeries, statin therapy has been noted to decrease the risk of AKI or dialysis requirement postoperatively. In over 200,000 Canadian patients over the age of 65, the use of statin therapy had a 16% reduced risk of AKI development following elective surgery. 9 This effect was not apparent in the entire cohort or in the subset of patients undergoing vascular clamping. It is possible that using a transperitoneal approach, the pneumoperitoneum is known to decrease the overall renal perfusion and cause some degree of global renal ischemia, which may blunt the direct effects of statins in only the clamped procedures. Despite several subset analyses in this dataset, we could not identify a subset of patients who benefited from these medications.
Recent retrospective studies have demonstrated that usage of statin therapy may improve oncologic outcomes in patients undergoing nephron-sparing surgery for small renal masses. Hamilton and colleagues found in a retrospective cohort of 2608 patients, that the ever/never usage of statin therapy was associated with a 33% risk reduction of cancer progression. This association was no longer statistically significant when evaluating statin usage as a time-dependent covariate. 22 Other authors have discussed that differing dosages and strengths of statin medications are more potent and therefore would have a greater effect on patients, however, this was not prospectively recorded or included in our data analysis.
Our analysis demonstrates a lack of association between statin therapy and oncologic progression. It is possible in our cohort that this effect was not established due to the low rate of clinical progression and recurrence. Certainly the studies that have found the largest association of statin usage with renal dysfunction perioperatively have been in population-based studies 9 ; however, the scope of this study was to evaluate this effect particularly in RPN. There are several limitations that exist in this study. Baseline characteristics between statin users and nonusers were significantly different. They were older, had more comorbidities, and had lower estimated GFR. Others have proposed that patients who are on statin therapies may have differing health seeking behaviors, which may provide inherent selection bias in this cohort. This data set does not identify the difference in either dosage or in the type of statin. Lipophilic statins such as atorvastatin and simvastatin may provide more potent vascular effects than hydrophilic statins like pravastatin due to their ability to cross cell membranes. Additionally, several studies have evaluated a dose response indicating a more therapeutic effect at higher doses; however, this data set does not establish that parameter.
Patients were not randomized to hilar clamping, and therefore, intrinsic characteristics may not be fully elucidated in this cohort. This article may lack the power to identify small changes in renal function associated with usage of statin medications at the time of partial nephrectomy. Further combined analyses or datasets would be required to confirm this finding. Despite the data supporting the continuation of statin medications in patients undergoing other surgical procedures, this is the only report we could identify, which evaluates their usage during clamped procedures for renal extirpative surgery. Without any clear benefit or detriment identified, we cannot endorse nor recommend against the continuation of statins at the time of RPN.
Conclusions
Our study is the first to examine the relationship of statin therapy with renal function and oncologic outcomes in patients undergoing robot-assisted partial nephrectomy. Statin usage was not associated with improvements in either short- or long-term renal function as estimated by the CKD-Epi equation. We could not identify subsets where statins provided the renoprotective effect. The risk of cancer progression was similar between statin users and nonusers. Based on our study, we were unable to delineate any significant impact of statin on renal function and oncologic outcomes in patients undergoing robot-assisted partial nephrectomy in comparison to patients without statin. We encourage collaborations between other centers in data pooling or confirmatory studies to validate these findings.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.