
Abstract
Introduction:
Recent advances in three-dimensional (3D) printing technology have made it possible to print surgical devices. We report our initial experience with the printing and deployment of endoscopic and laparoscopic equipment.
Materials and Methods:
We created computer-aided designs for ureteral stents and laparoscopic trocars using SolidWorks. We developed three generations of stents, which were printed with an Objet500 Connex printer, and a fourth generation was printed with an EOSINT P395 printer. The trocars were printed with an Objet30 Pro printer. We deployed the printed stents and trocars in a female cadaver and in vivo porcine model. We compared the printed trocars to two standard trocars for defect area and length using a digital caliper. Paired T-tests and ANOVA were used to test for statistical difference.
Results:
The first two generations of stents (7F and 9F) were functional failures as their diminutive inner lumen failed to allow the passage of a 0.035 guidewire. The third generation 12F stent allowed passage of a 0.035 guidewire. The 12F diameter limited its deployment, but it was introduced in a cadaver through a ureteral access sheath. The fourth-generation 9F stents were printed and deployed in a porcine model using the standard Seldinger technique. The printed trocars were functional for the maintenance of the pneumoperitoneum and instrument passage. The printed trocars had larger superficial defect areas (p<0.001) and lengths (p=0.001) compared to Karl Storz and Ethicon trocars (29.41, 18.06, and 17.22 mm2, respectively, and 14.29, 11.39, and 12.15 mm, respectively).
Conclusions:
In this pilot study, 3D printing of ureteral stents and trocars is feasible, and these devices can be deployed in the porcine and cadaver models. Three-dimensional printing is rapidly advancing and may be clinically viable in the future.
Introduction
M
Disposable medical devices also represent a significant OR expense. In 2009, Park and colleagues estimated that supply costs represent 58% of the total budget of an OR and this figure has been increasing. 8,9 Much of the cost associated with disposable equipment is due to packaging, sterilization, transportation, storage, and administrative costs. 10 Packaging materials from instrumentation and surgical supplies such as paper and plastic packaging can account for up to 30% of the total waste collected within ORs. 11 OR equipment is expensive and results in the creation of a large volume of waste.
The cost and environmental impact of distant manufacturing, packaging, sterilization, and transportation of disposable equipment has engendered interest in the development of alternative strategies to reduce OR costs. Recent advances in three-dimensional (3D) printing technology have made it feasible to 3D print surgical devices. As a result, 3D printing technology is currently being implemented into a variety of medical fields with each manufactured product ranging in its potential application and purpose. 12 –16 Utilizing this technology, we explored the feasibility of 3D printing ureteral stents and laparoscopic trocars, and we report our initial experience.
Materials and Methods
Three-dimensional ureteral stents
We initiated ureteral stent and trocar development with the creation of computer-aided designs using SolidWorks Software (Dassault Systems, Concord, MA) (Fig. 1). The first-three generations (7F, 9F, and 12F, respectively) of stents were printed with an Objet500 Connex printer (Stratasys Ltd.©, Minneapolis, MN) using a rubber-like black material (Tango Black Plus FLX980, with a 70-shore value). During the PolyJet printing process, successive layers of a liquid photopolymer were built on top of one another in both the horizontal and vertical axis starting from the bottom up. These layers of material were fused solid with a UV light. To ensure that the stent maintained the proper structure and did not collapse during printing, a support material was simultaneously printed within the internal lumen of each stent. Following printing, the dissolvable support material located within the internal lumen of each stent was removed with a high-pressured water hose and a NaOH solution bath. Due to limitations in the cleaning process, we removed residual support material from the lumen by passing a 0.035 Amplatz Super Stiff™ guidewire (Boston Scientific Corp., Natick, MA) repeatedly through the stent (Fig. 2).

Computer-aided design (CAD) models created using SolidWorks.
Residual material (plasticized gel) poststent cleaning (first three generations).
The fourth-generation (9F) stents were printed with an EOSINT P 395 printer (EOS e-Manufacturing Solutions, Krailing, Germany), using a Nylon powder material (Elasto Plastic; Shapeways, Eindhoven, Netherlands). The 3D printer employs laser energy to scan a bed of powder to solidify a bottom foundation layer. The new layer of Nylon powder is then laid over the previous layer in an additive process. Over time, the successive layers of Nylon powder are melted and solidified into the existing 3D stent structure. As the ureteral stent was printed, the laser energy did not fuse the Nylon powder that resided within the inner lumen. The fourth-generation stents were void of the plasticized support material in the inner lumen and did not require high-pressure cleaning. However, we performed a manual cleaning of the inner lumen of the stent with a 0.035 Amplatz Super Stiff guidewire.
The third generation 12F stents were tested in a female cadaver urinary system. We performed cystoscopy using a rigid cystoscope. After locating the ureteral orifice, we deployed a 5F open-ended ureteral catheter (Cook® Medical, Bloomington, IN) and then performed bilateral retrograde ureteropyelogram to define the urinary system anatomy. Next, we advanced a 0.035 guidewire (Boston Scientific Corp.) into the renal pelvis under fluoroscopic guidance. We deployed a 12F to 14F ureteral access sheath over the guidewire to dilate the ureter to facilitate stent insertion. We then removed the access sheath and advanced the stent over the Amplatz Super Stiff guidewire until it was effectively positioned in the right renal pelvis.
The fourth-generation 9F stents were tested in a female porcine model. Using a rigid cystoscope, we introduced a 5F open-ended ureteral catheter into the left ureter. Next, we deployed a 0.035 standard guidewire through the catheter and into the left renal pelvis. The correct position of the guidewire was confirmed through fluoroscopic imaging. Next, we removed the cystoscope and open-ended catheter while the guidewire remained in the correct position. The fourth-generation stent was then advanced over the guidewire and into the renal pelvis using the standard Seldinger technique. We performed a ureteropyelogram to evaluate any contrast extravasation and proper stent placement in the renal pelvis.
Three-dimensional trocars
The trocars were printed with an Objet30 Pro printer (Stratasys Ltd.) using a rigid opaque material (Vero White Plus RGD835). We modeled our printed trocar after a nondisposable, Karl Storz, 6-mm Ternamian EndoTip Cannula trocar (Karl Storz, Tuttlingen, Germany). The trocar body and screw-shaped insufflation port were effectively recreated using a 3D printer. The silicon insufflation stopcock (Karl Storz) and the valve used to control the flow of carbon dioxide through the insufflation port could not be printed. As such, we used the standard silicon insufflation stopcock from a standard, 6-mm Ternamian EndoTip Cannula trocar. After gaining permission from our institutional IACUC, we performed testing of initial prototypes in four in vivo domestic pigs. A total of 30 trocar insertions were recorded for each trocar type. We anesthetized each 25 kg pig with a mixture of telazol and xylazine. After Veress insufflation to 15 mm Hg, a standard, 12-mm Ethicon Endopath® Xcel® trocar was inserted into the peritoneal cavity and a laparoscope was introduced for visualization. Ninety identical 5 mm incisions were made in the abdominal wall in a uniform manner allowing for the entry of each trocar. We tested the 3D printed trocar, the 6-mm Karl Storz Ternamian EndoTip Cannula (Karl Storz), and the 5-mm Ethicon Endopath Xcel Trocar (Ethicon Endosurgery, Inc., Cincinnati, OH) (Fig. 3). Using a metric digital caliper, we measured the inner and outer diameter of each laparoscopic trocar.

Three different trocars evaluated.
For each trocar, we recorded the ability to maintain constant pneumoperitoneal pressure. Following the removal of each trocar, we used a digital caliper to measure the maximal superficial defect length and the mean superficial defect area according to the technique described by Tarnay and colleagues. 17 Additionally, the trocar insertion site outlines were photographed, scanned, and uploaded onto a computer. ImageJ, an image-processing software developed by the National Institute of Health (National Institutes of Health, Bethesda, MD) was used to calculate the superficial defect area.
The results are stated as the mean values with standard deviations. Paired T-tests and ANOVA tests were used to test for statistical difference between the three trocars in terms of defect area (mm2) and defect length (mm). A p-value of <0.05 was considered statistically significant.
Results
Three-dimensional ureteral stents
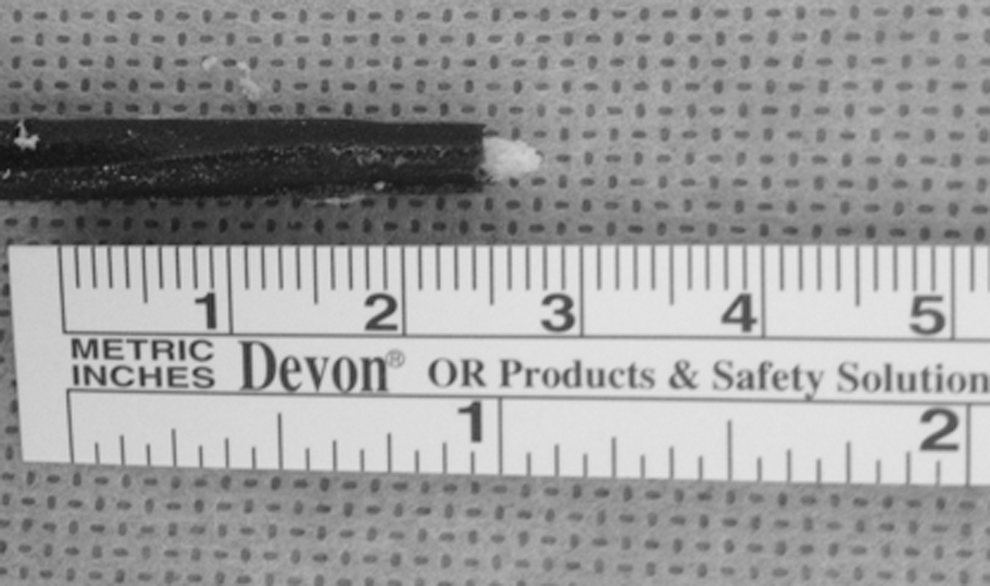
The first (7F) and second (9F) generations of stents had inadequate inner lumens and did not allow the passage of a 0.035-inch guidewire. The reduced wall thickness of the 7F and 9F stents compromised the structural integrity and strength of the stent wall (Table 1). All attempts to pass a guidewire through the inner lumen failed and resulted in a rupture at the stent pigtail. The third-generation 12F stent had a larger lumen, which allowed passage of a 0.035 standard guidewire. Initial attempts to deploy the 12F, 3D printed (Fig. 4) stent over the guidewire with the standard Seldinger technique failed. However, after dilation of the ureteral orifice with a 12F to 14F access sheath, we deployed the 12F, 3D printed stent in a female cadaveric torso over a 0.035 Amplatz Super Stiff guidewire. The fourth-generation (9F) stent had a larger wall thickness (Table 1) and was easily deployed in a female porcine model over a 0.035 standard guidewire using the standard Seldinger technique. The stents were not radiopaque and deployment was confirmed cystoscopically distally and through open dissection of the renal pelvis proximally. A retrograde ureteropyelogram confirmed that there was no evidence of contrast extravasation confirming the integrity of the collecting system. In addition, the models were dissected to confirm that there was no gross damage to the collecting system.

Three-dimensional printed ureteral stent.
Three-dimensional trocars
With contemporary technology, the time to print four trocars using an Objet30 Pro printer using Vero White Plus RGD835 is estimated to be 5 hours. The dimensions of all trocars tested are presented in Table 2. We recorded 30 trocar insertions with each trocar type. All the tested trocars were effectively inserted on initial attempts in in vivo porcine models. All trocars evaluated were able to maintain the pneumoperitoneum at 15 mm Hg. The 3D printed trocars demonstrated comparable performance to the contemporary trocars examined with regard to ability to deploy and pass standard laparoscopic instrumentation. The maximal superficial defect lengths, measured after trocar removal using metric digital calipers, were comparable on all porcine models. In the porcine model, the mean superficial defect length was 14.3 mm (±0.85) for the 3D printed trocar, 11.4 mm (±1.17) for the Karl Storz trocar, and 12.1 mm (±1.24) for the Ethicon trocar (p<0.001). The mean superficial defect areas were 29.41, 18.06, and 17.22 mm2 (p<0.001) for the 3D printed, Karl Storz, and Ethicon trocars, respectively.
3D=three dimensional.
Discussion
Three-dimensional printing has previously been described in orthopedics, and oral and maxillofacial to create prosthetics, dental implants, and for facial and mandibular reconstruction. 12 –16,18 These studies document the unique ability 3D printing technology has to improve complex reconstructive procedures. In contrast, we directed our efforts toward the design and production of frequently utilized disposable medical equipment. We believe that the continued advancement of 3D printing technology may make it possible to print surgical devices in the operating theater. While not evaluated in the current study, future application of 3D printing equipment in the OR may include the opportunity to print customized disposable equipment.
The initial two generations of 3D printed stents created were functional failures as the diminutive or incomplete inner lumen failed to allow the passage of a 0.035 guidewire. Thus, we created a 12F outer diameter third-generation stent design, which had a functional lumen. During the 9 months in which this study was conducted, several significant advances were made in 3D printing technology. The fourth-generation stent was created with a new material (Shapeways introduced a plastic elastomer material, Elasto Plastic). This material allowed the creation of a fourth-generation stent, which was 9F and had improved wall thickness. This stent possessed the ability to withstand the insertion of a 0.035 guidewire and was deployed with the standard technique.
We also explored the feasibility of 3D printing and deploying laparoscopic trocars. Despite the availability of nondisposable trocars, many centers continue to use a robust number of disposable trocars. We demonstrated that the 3D printed trocars have comparable performance to the modern trocars examined with regard to the ability to maintain the pneumoperitoneium and pass standard laparoscopic instrumentation.
There remain a number of limitations to 3D printed technologies. Currently, we cannot print a stent with a tapered end, as typically seen in contemporary ureteral stents. The 3D printed stents created to date remain radiolucent, and we have not addressed the biocompatibility, sterility, durability, and encrustation characteristics of printed stents. Additionally, the tensile characteristics of contemporary 3D printing materials are limited and needs to be improved. The printed trocars did have limitations, including a larger outer diameter, which yielded an increased defect area and length. Another limitation of this study is that we have not evaluated important stent characteristics such as surface composition, tensile strength, elasticity, and memory of the printed stents as compared to contemporary technologies. All of these metrics will have to be considered in subsequent evaluations. As with our printed stents, multiple issues still need to be addressed before clinical application of 3D printed trocars.
Despite the observed limitations, our results are encouraging and demonstrate the possibility of integrating 3D technology into the operating theater in the manufacturing of medical devices. Additionally, while not evaluated in this study, patient-specific customized equipment could be printed. The application of this technology is currently fueling innovation and has the potential to fundamentally alter product manufacturing and distribution within the healthcare system.
Conclusions
Three-dimensional printing of ureteral stents and trocars is feasible, and these devices can be deployed in a porcine and cadaver model. Contemporary technology has limitations, including radiopacity, the reduced tensile nature of the material, which limits deployment and sterilization.
Footnotes
Acknowledgments
The authors would like to thank Benjamin Dolan (Director of Design and Engineering Projects at UC Irvine RapidTech, Irvine, CA), Purple Platypus: Precision 3D Printers, Software, & Service (Irvine, CA), and Shapeways (Eindhoven, Netherlands) for their continued efforts and contributions throughout our study.
Disclosure Statement
No competing financial interests exist.