
Abstract
Objective:
To evaluate kidney/adjacent organs positional changes in patients undergoing percutaneous nephrolithotomy (PCNL) using noncontrast computed tomography (NCCT) in prone and supine positions.
Methods:
Patients scheduled PCNL were prospectively enrolled in the study and underwent NCCT in supine and in prone position (with boosters). Two imaginary lines for the posterior calyx of upper/mid/lower poles of both kidneys in prone and supine decubitus were considered and compared. Line I (LI): drawn horizontally in the coronal plane in contact with the posterior edge of the kidney. Line II (LII): drawn from the antero-lateral edge of the vertebra through the middle of the posterior calyx (ideal puncture line). Renal depth (d) was measured from LI to the anterior extremity of the vertebra. The maximum access angle (a) considered the window available in the axial plane to perform a secure approach to each calyx.
Results:
Thirty-seven patients were analyzed; 56.7% were female; mean BMI was 28.3±4.9 kg/m2. For the right kidney, prone position was associated with more organs crossed by LI (54.1% vs 18.9%; p<0.01) and LII (56.8% vs 27%; p=0.03) in the upper calyx. For the left kidney, LII crossed more organs in prone in the upper calyx (54.1% vs 29.7%; p=0.03). Both kidneys showed a tendency to be deeper in the supine position, which provided a wider access angle.
Conclusions:
Supine NCCT is not accurate to plan PCNL access in prone position. Prone decubitus is associated with more potential organ injuries in the upper pole. In supine, the kidney situates deeper in the abdomen but the access angle is wider than in prone.
Introduction
P
Enthusiasts of the PCNL procedure in prone and supine positions have strong arguments to support one background over the other. Nevertheless, training and experience are the two most important determinants to improve outcomes while reducing morbidity. 4 Additionally, adequate preoperative planning is a potential contributor to reducing complications that cannot be overlooked. To date, the few studies comparing kidney parameters in prone and supine positions have particular methodological flaws and do not provide a practical overview of those changes when the patient is analyzed in both decubitus. 5 –8 Literature also lacks studies evaluating the exact influence of these bodily changes in patient safety and risk of adjacent organ injury during the percutaneous access.
The purpose of our investigation was to systematically evaluate positional changes of kidney and adjacent organs during NCCT in supine and in prone position and if the supine NCCT allows accurate prediction of basic surgical parameters when the patient is turned prone.
Materials and Methods
After IRB approval, patients with large or complex stones scheduled for PCNL were prospectively enrolled in the study. Exclusion criteria comprised pregnancy, previous renal surgery (except for shock-wave lithotripsy), and kidney malformations. All patients underwent NCCT in the supine position without boosters and subsequently NCCT in the prone position restricted to the kidney area with boosters by the shoulders and abdomen to accurately simulate the surgical setting. All NCCT were done according to the same protocol with a 64-detector row CT scanner (Siemens Medical Solutions, Germany; 120 kVp; 6 mm collimation; 3 mm slice thickness). The axial plane was used to compare radiological findings between the two positions. An experienced surgeon and a proficient radiologist reviewed all NCCTs to obtain pre-established measures as follows.
Ideally, the entry point for the kidney puncture is the posterior axillary line, a difficult point to determine exclusively with a NCCT. Prassopoulos et al. 7 described two imaginary lines to evaluate in a practical manner the safety of an ideal percutaneous access to the kidney in supine decubitus. Line I (LI) was horizontally drawn in the coronal plane in contact with the posterior edge of the kidney. Line II (LII) was drawn from the antero-lateral edge of the vertebra through the middle of the posterior calyx. LII was considered the ideal tract line for a PCNL access. We compared those two imaginary lines for each posterior calyx in the upper, mid - renal hilum level, and lower pole of both kidneys in prone (Fig. 1A) and supine decubitus (Fig. 1B). We evaluated whether there were organs crossed by or posterior to those lines (at risk during the PCNL access), and whether they were above or beyond the 12th rib.
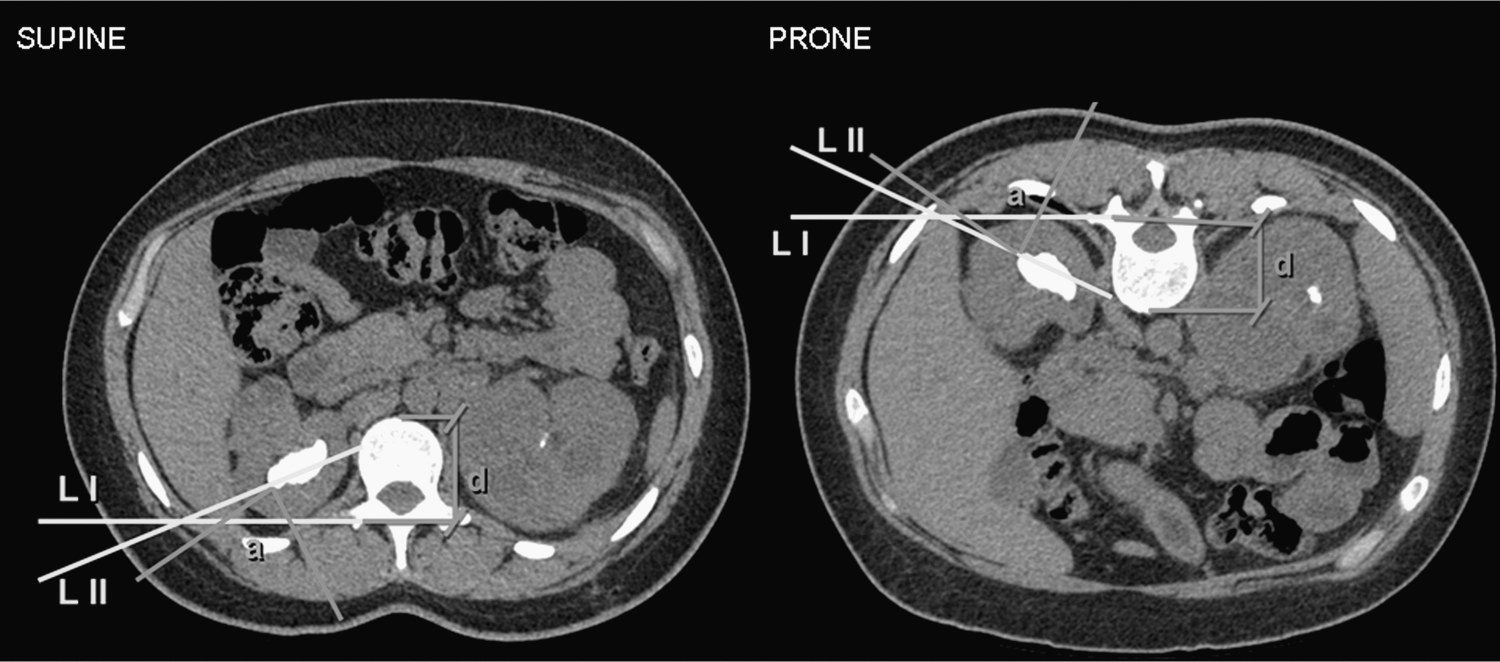
Primary (Line I and II) and secondary (depth–d; maximum access angle–a) end points acquired from noncontrast computed tomography on supine and prone positions.
Secondary end points (Fig. 1) considered the same posterior calyx marked to obtain LI and LII. To determine renal depth (d) for every calyx, the distance between the anterior edge of the vertebra body and the posterior edge of the kidney (LI) was measured. To evaluate the window available to perform a secure approach to all calyces, the maximum access angle (a) was traced with the vertex in the posterior edge of each calyx, one leg at the lateral border of paraspinous muscles, the other at the first adjacent organ.
After acquiring all four measures (LI, LII, d, and a) for all three renal poles of both kidneys in both positions, results were compared between the two decubitus. Statistical analysis was performed using SPSS® version 20 (SPSS, Inc., Chicago, IL). Results were expressed as mean±standard deviation and range. Groups were compared using Student t-test and Chi-square/Fisher's exact test. Significance was set at p<0.05.
Results
Demographic data
From May/12-Mar/13, 37 patients met the inclusion criteria. Twenty-one (56.7%) were female; mean age was 44.0±12.2 (17–72) years old; mean body mass index (BMI) was 28.3±4.9 (16.8–42.0) kg/m2.
Primary end points
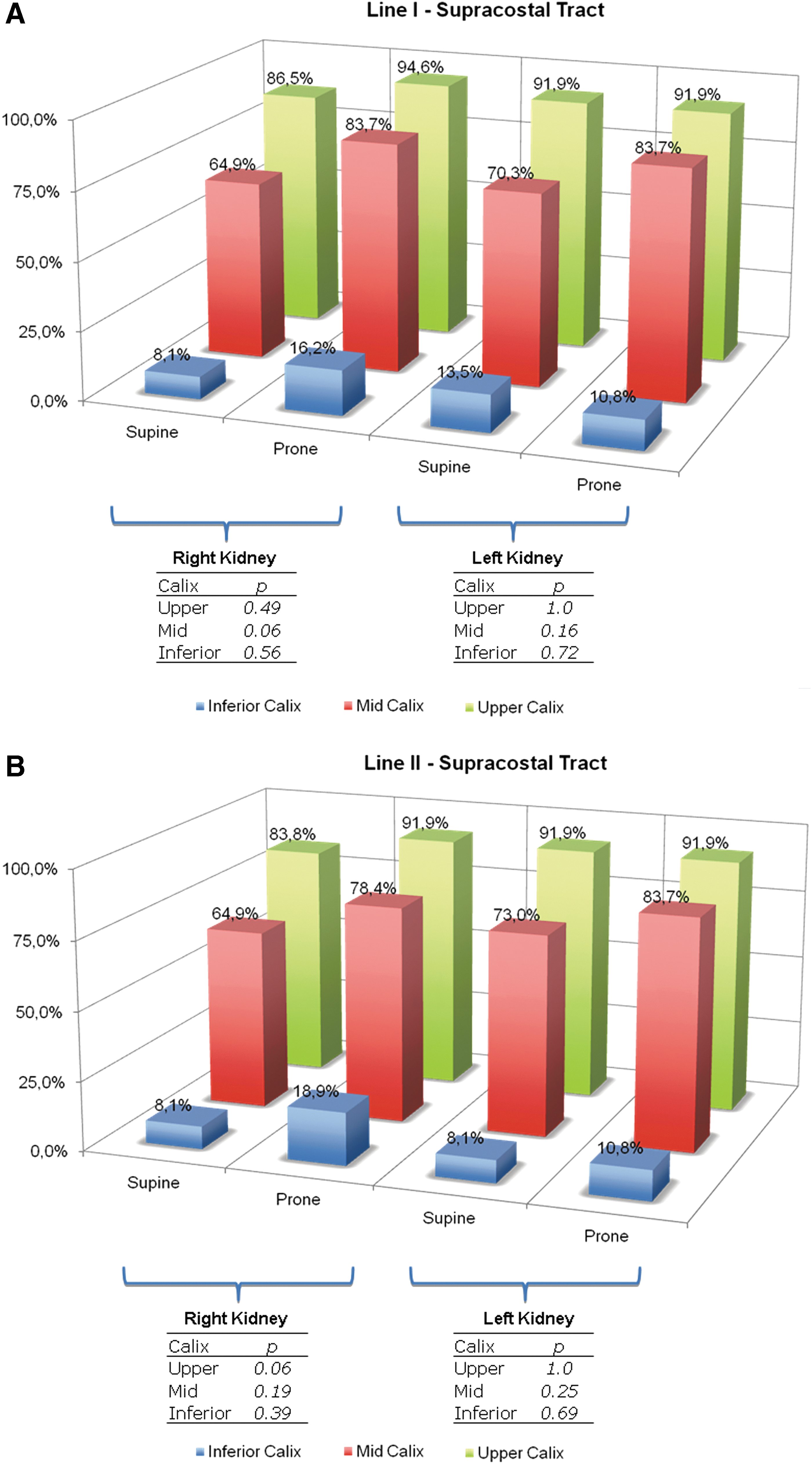
In the right kidney, the prone position was associated with more organs crossed by LI in the upper calyx (54.1% vs.18.9%, respectively; p<0.01) (Table 1, A). When prone, the most common organ to be traversed by LI was the pleura, 18 times (48.6%) in the upper pole and four times (10.8%) in the mid pole. The liver was the most common organ to be potentially injured when supine, being crossed in seven (18.9%) patients in the upper pole and in 1 (2.7%) case in the mid pole. Retrorenal colons potentially crossed by LI were noted only in the prone decubitus, particularly in the lower pole (n=3; 8.7%). The incidence of a supracostal LI was high (86.5% and 94.6% in the upper pole when supine and prone, respectively) and statistically similar between positions (Fig. 2A). Figure 3 depicts significant kidney dislodgment when the patient is turned supine to prone.
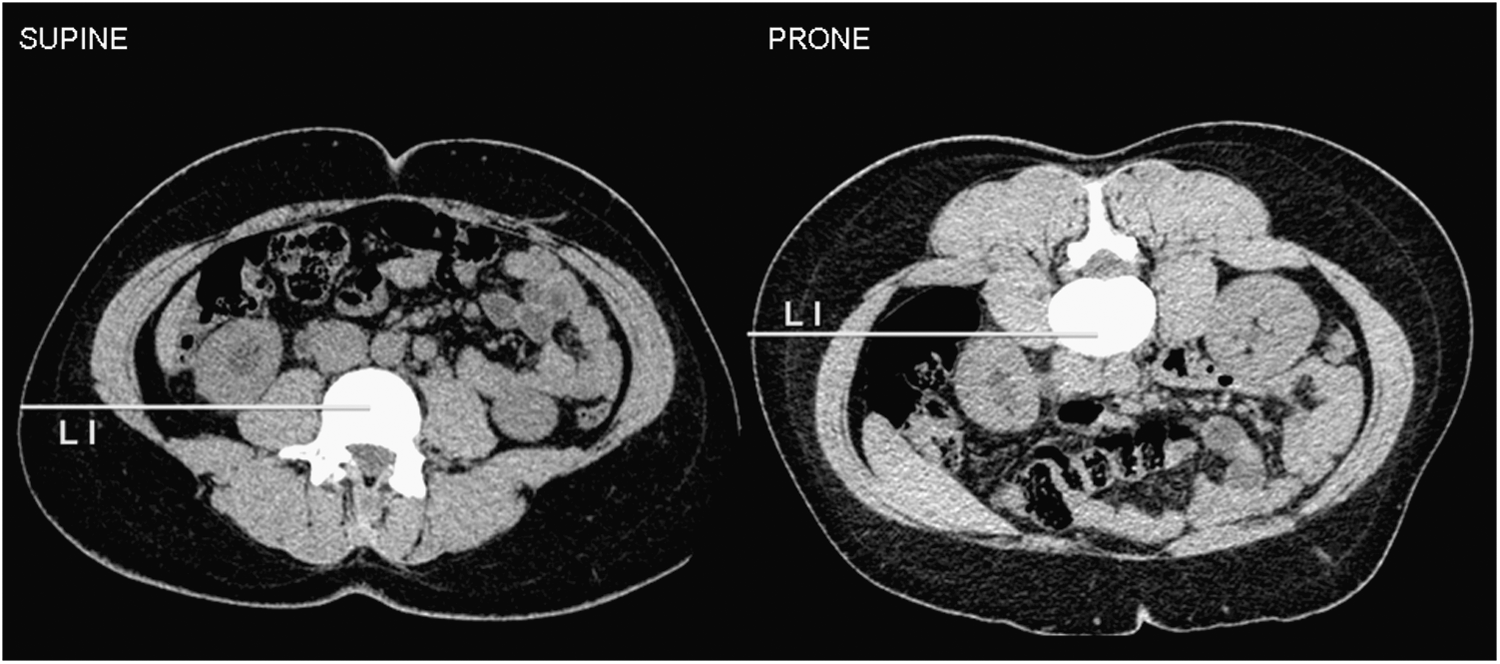
Noncontrast computed tomography acquired in supine and prone positions bring to light expressive kidney displacement with colonic progression to the posterior aspect of the kidney (Line I defines the retrorenal colon in prone but not in supine position).
Statistically significant values are highlighted in bold.
NCCT=noncontrast computed tomography.
When considering LII for the right kidney, there was a higher potential incidence of organ injuries in the upper pole in prone (56.8%) compared with supine position (27%) (p=0.03; Table 1, A). A nonsignificant higher incidence of potential injuries to the colon was noted in the prone position for LII in the lower pole (16.2% vs 2.7%, respectively; p=0.14). There was a complete discordance between the colons crossed by LII in both decubitus. A higher nonsignificant incidence of supracostal tracts for LII was seen in the prone decubitus (Fig. 2B).
For the left kidney, three (8.1%) potential colonic injuries by LI (retrorenal colons) were noted in the lower pole when prone, while none when supine (p=0.30; Table 1, B). There was a nonsignificant trend for more potential organ injuries and supracostal tracts in the prone position (Table 1, A and Fig. 2A).
LII evaluation revealed a higher incidence of potential organ injuries in the upper pole when prone (54.1%) compared with supine (29.7%)(p=0.03; Table 1, B). A higher nonsignificant incidence of potential injury to the colon was found for the prone position for the lower pole (16.2% vs 5.4%, respectively; p=0.21). Of the two colons at risk when supine, one (50%) was still at risk when prone. Conversely, of the six colons at risk when prone, only one (16.7%) was crossed by LII when supine. The incidence of supracostal tracts was similar between the two positions (Fig. 2B).
Secondary end points
The right kidney was more superficial in the prone position, particularly in the upper (32.7 vs 41.3 mm, respectively; p=0.007) and mid poles (37.7 vs 43.3 mm, respectively; p=0.03) (Table 2, A). The maximum access angle to the upper pole was wider in the supine decubitus (42.3° vs 25.8°, respectively; p=0.05).
Statistically significant values are highlighted in bold.
The left kidney was deeper in the supine position in the mid (43.8 vs 37.6 mm, respectively; p=0.01) and lower pole (35.7 vs 27.9 mm, respectively; p=0.03) (Table 2, B). A wider access angle was found in the supine decubitus for the lower pole (92.9° vs 77.8°, respectively; p=0.03).
Discussion
The Clinical Research Office of the Endourological Society recently stated that 80% of PCNLs are performed in the prone position worldwide. 3 Shorter operative time and higher stone-free rates were found with prone PCNL, this being outbalanced by increased patient safety with the supine decubitus. The recommendation made was to tailor PCNL position to individual patient characteristics and surgeon's preference. High volume centers achieve better outcomes and the safety of PCNL improves with the number of surgeries performed in a given center per year. 4 However, complications occur even in experienced hands. They are frequently associated with the percutaneous access and inadequate tract planning might play an important role. Routine preoperative workup usually comprises a supine NCCT even if the procedure is programmed in prone. Kidney relation to other intra-abdominal organs changes with the decubitus and a close insight of the impact on potential organ injury during the percutaneous access has never been established. Supine PCNL is underperformed worldwide mainly because of an unfounded fear of increased risk for potential adjacent organ injury. Our study analyzing the ideal tract in a comparative matter between the two positions is the largest series and indicates the safety of supine access to the kidney in an academic standpoint.
Prassopoulos et al. 7 studied 1708 abdominal NCCT in supine position. To estimate the position of parts of the colon in the pararenal space, NCCT images of the retroperitoneum were chosen and LI and LII were drawn. The descending colon in relation to the left kidney was posterior to LI and LII most frequently at the level of the lower calyces (3.6% and 10.4%, respectively), less frequently at the level of the renal pelvis (0.8%; 6.4%), and seldom at the level of the upper calyces (0.4%; 1.2%). For the ascending colon in relation to the right kidney, this normal variant was observed in smaller percentages at the lower calyces (LI 1%; LII 2.8%), seldom at the mid calyces (0.2%; 0.6%), and never at the upper calyces. The authors, however, did not evaluate potential injuries to other organs and did not compare supine and prone findings. Their figures are similar to ours in prone and we found no retrorenal colons in the supine.
Our findings clarify that when the patient is supine and the colon is located latero-posteriorly to the kidney, it is erroneous to infer that it would change to a more favorable position when the patient is turned prone (Fig. 3). Clinically, PCNL in prone is associated with 0.3% to 0.8% risk of colonic injury, 1,2 while there are no reported cases of colonic injuries with the supine position. 9 –19 Hopper et al. 19 analyzed 500 supine and 90 prone NCCT and found the bowel positioned posterior to the kidney in 1.9% and 10% of cases, respectively. Nevertheless, the authors did not evaluate the colonic position in relation to the percutaneous access tract. We found a potential risk for colonic injury in supine and prone by considering LII of 2.7% and 16.2% for the lower pole of the right kidney respectively, and 5.4% and 16.2% for the lower pole of the left kidney, respectively. When the colon is at risk on preoperative NCCT and the PCNL is planned in supine, the use of intra-operative ultrasound is preferred over turning the patient prone. 9,17
Duty et al. 5 evaluated 20 patients who underwent prone and supine computed tomography urograms. The overall mean supine and prone tract lengths were 108.3 and 82.6 mm (p<0.001) on the right and 103.7 and 85.4 mm (p<0.001) on the left, demonstrating a more superficial kidney in the prone position. Our data showing an overall higher renal depth in the supine position is in accordance to their findings. In theory, the longer the access tract, the less maneuverable the distal end of the sheath will be within the collecting system and the more challenging is the nephroscopy. The use of flexible nephroscopy might in part help overcome this issue. Their overall mean access angle was 87.7° and 89.4° for the right and left kidney, respectively, in the supine position in contrast to 99.7° and 104° in the prone position (p=0.018 and p=0.007). This is in disagreement with our findings and although the methodology to attain the angle from NCCT was exactly the same, they did not use boosters during the prone NCCT. The authors found a higher nonsignificant difference in the position of the renal hilum relative to the anterior border of the lumbar vertebral body between both decubitus. 5 However, they used the renal hilum, a relative fixed structure of the organ, to evaluate antero-posterior differences. Instead, we used LI, which takes in account the posterior border of the kidney, probably its most movable portion. In fact, our intercalyx sub analysis between supine and prone positions (data not shown) suggests that the mid calyx tends to move less than the others. In addition, we found that the kidney tends to displace more with the positional change in patients with MBI<30 kg/m2 compared with obese individuals.
Azhar et al. 6 enrolled 16 candidates for PCNL with lower pole stones to undergo preoperative supine and prone (with bolsters) NCCT. They found a significant decrease in skin-to-stone distance from 9.0 to 7.6 cm (p<0.001) in prone positioning, similar to previous studies. 5 Furthermore, visceral organ-to-tract distance significantly decreased from 3.5 cm in supine to 2.8 cm in the prone position (p=0.04), which may indicate a safer percutaneous access with the supine position. Although we did not evaluate this particular parameter, a parallel can be made by the wider maximum access angle found in our patients in supine compared with prone position. A wider angle provides a greater margin of safety when the surgeon is targeting a particular calyx. They also found the colon to be the organ most frequently closest to the percutaneous access (84%), followed by the liver (16%). 6 When considering LII for the upper pole, we found the liver (27% supine and 13.5% prone) and pleura (2.7% supine and 51.3% prone) to be the most common organs at risk in the right kidney, and the spleen (18.9% supine and 21.6% prone) and pleura (10% supine and 29.7% prone) in the left kidney. For the lower pole, we found the colon to be the major organ at risk for the right (2.7% supine and 16.2% prone) and left (5.4% supine and 16.2% prone) kidneys. In agreement, Tuttle et al. 8 compared axial and reformatted computed tomography scans in supine and prone positions and found the risk of organ injury associated with lower pole puncture on axial images to be 6% in supine and 15.1% in prone. Cormio et al. 20 reported that the colon is pushed against the lateral surface of the kidney along the path of the percutaneous access tract when the patient is in the prone position. Conversely, the colon falls anteromedially when the patient is positioned in the supine position. The exact mechanism causing this variability is unclear.
Our study is not without limitations. First, the number of patients enrolled is small and a few tendencies observed remained nonsignificant. Nevertheless, in its kind, it is the largest reported series and we could provide a comprehensive view of the abdominal organ changes and respective consequences to the percutaneous access planned for PCNL. A second potential limitation relies in the fact that we used NCCT and not tomography urograms. Although the exact calyx region of interest might be more difficult to determine, NCCT remains the gold standard preoperative image modality for PCNL, being the ideal model to be studied. Furthermore, the risk of excessive radiation is a concern and newer tomography softwares allow accurate definition of calyceal anatomy without need for contrast infusion. Finally, we must consider that the number of potential organ injuries found in this study is much higher than those seen in clinic. The use of ultrasound and oblique punctures allow the surgeon to access in an infracostal manner a calix considered supracostal in the axial plane of NCCT. Also, the number of subclinical lesions is unknown. Lines I and II symbolize two potential entry sites for PCNL. Nevertheless, they are not always the exact representation of the ideal percutaneous tract for every patient. Our main goal was not to prove they should be blindly used in every case, but simply to compare prone and supine access in a standardized matter with two previously defined lines. Our findings help understand why the number of reported colonic injuries is higher in the prone compared with the supine position and prove that both positions have pros and cons in terms of anatomical variations. Ideally, if the patient is a candidate for PCNL, NCCT acquisition should be tailored to the decubitus the surgeon is used to position the patient in.
Conclusion
The supine noncontrast computed tomography is not accurate to plan percutaneous access in the prone position. Prone decubitus is associated with more potential organ injuries in the upper pole when considering an ideal tract line. In supine position, the kidney situates deeper in the abdomen but the access angle available for the puncture tends to be wider than in prone position with boosters.
Footnotes
Disclosure Statement
The authors declare that they have no conflict of interest.