
Abstract
Purpose:
To report our experience and evaluate the efficacy and safety of real-time ultrasonography-guided percutaneous nephrolithotomy (PCNL) using SonixGPS navigation in patients with kidney stones.
Materials and Methods:
From December 2012 to May 2013 in our hospital, the SonixGPS needle tracking system was used for real-time ultrasonography-guided puncture during PCNL in 25 patients with kidney stones. All the patients were under general anesthesia, in prone position; holmium laser lithotripsy was used in all patients after renal access was established. The time needed to perform puncture and the success rate of PCNL were recorded as two most important outcomes of this study.
Results:
All 25 patients underwent PCNL successfully with the help of SonixGPS navigation. The mean puncture time was 5.5 minutes (range 3–9 min), and the mean operative time was 74 minutes (range 30–100 min), respectively. The primary stone clearance rate of PCNL was 92% (23/25); no major intraoperative or postoperative complications occurred.
Conclusion:
The results of this study indicate that puncture under SonixGPS navigation is safe and efficacious in PCNL, which may provides a new choice for PCNL.
Introduction
P
The SonixGPS (Ultrasonix, Medical Corp Richmond, BC, Canada) is a novel electromagnetic needle tracking system for ultrasonography-guided needle interventions. It can help clearly predict and observe the trajectory of the needle before and during puncture, thus facilitating needle-beam alignment and guidance to the target. Previous studies 5 –7 reported that the use of SonixGPS for real-time ultrasonography-guided spinal anesthesia and vascular access was effective with low failure and complication rates.
This article summarizes our initial clinical experience with real-time ultrasonography-guided PCNL using SonixGPS navigation and discusses the safety and efficacy of this technique.
Materials and Methods
From December 2012 to May 2013, we performed PCNL with real-time ultrasonography-guided puncture using the SonixGPS needle tracking system in patients with kidney stones in Xinhua Hospital (Shanghai, China). Twenty-five consecutive candidates were enrolled in this study after routine preoperative evaluations. Inclusion criteria were patients with pelvic or caliceal calculi >2.0 cm in diameter or multiple or staghorn stones. Patients with a horseshoe, pelvic kidney, or urosepsis were excluded from this study. Informed consent was obtained from all eligible participants before the procedure.
Demographic and clinical characteristics of the patients are shown in Table 1. Renal anatomy and stone location and size were evaluated by intravenous urography (IVU) or CT before surgery. The stone size was measured at the maximal diameter on the preoperative IVU or CT with a mean stone size of 34.8 mm (range 24–56) mm. Infection and anemia were treated preoperatively. All the operations were performed by the same surgeon.
BMI=body mass index; PCNL=percutaneous nephrolithotomy.
With the patient under general anesthesia, a 5F ureteral catheter was inserted retrogradedly into the pelvicaliceal system via a cystoscope with the patient lying in the lithotomy position. After that, the patient was turned into a prone position, and the pyelocaliceal system was distended using saline injection. The easy-to-maneuver GPS arm transducer was placed near the patient, with the GPS transducer adjusted for good signal strength. To determine the renal access path and evaluate the stone size, location, and renal anatomy, ultrasound scanning was performed with the SonixGPS ultrasound probe (Ultrasonix Medical Corp Richmond, BC, Canada) in the area of rib 11 or 12 costal margin before PCNL (Fig. 1). The ultrasonographic image on the screen of SonixGPS allows for attaining an excellent needle direction and position at all times. The direction, depth, and angle of needle insertion could be adjusted from time to time when necessary according to the real-time information retrieved by the needle sensor (Fig. 2).

Percutaneous nephrolithotomy puncture using SonixGPS with the patient in the prone position. The electromagnetic transmitter (
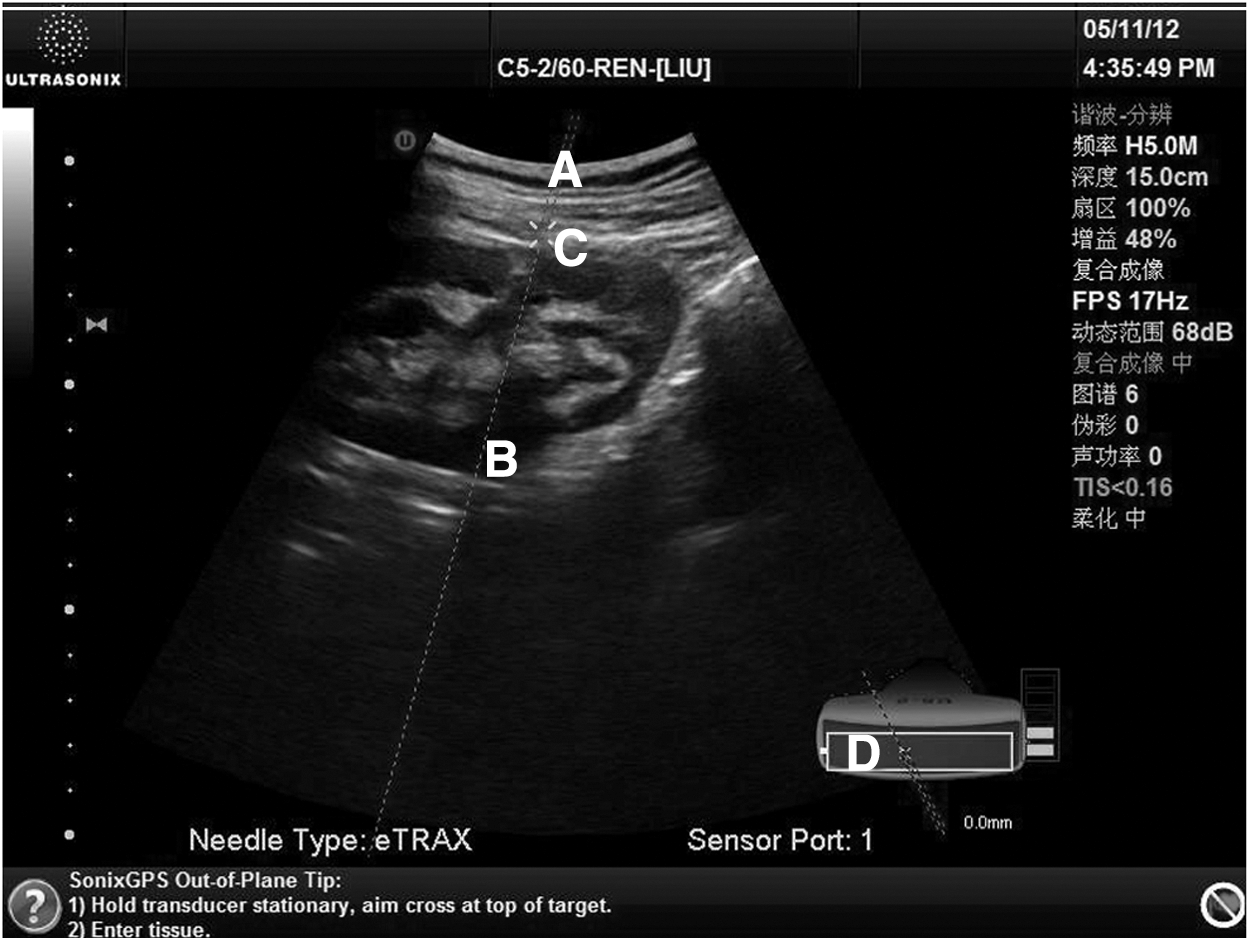
Ultrasonography image showing real-time needle advancement into kidney. The outline (
With the help of the SonixGPS needle tracking system, an 8-cm, 18-gauge SonixGPS needle was inserted in the target kidney calices. After that, the inner stylet containing the needle sensor was removed, and a zebra guidewire was inserted into the collecting system through the introducer needle. With the help of the guidewire, the tract is dilated with a 9F metal dilator. During subsequent dilation with a metal coaxial dilator, the ultrasound probe was held with one hand while the dilator was advanced with the other hand. The position of the ultrasound probe was maintained there during dilation to monitor the depth and location of the dilator. Next, the percutaneous tract was dilated up to 16F with a metal coaxial dilator, and a 16F peer-away sheath (uroVision GmbH) was passed to the collecting system. All these steps including tract dilation were performed under SonixGPS guidance.
Stone fragmentation was performed with a F8/9.8 rigid ureterscope (Richard Wolf, Knittlingen, Germany) using a 550-um holmium laser fiber, and the fragments were removed using grasping forceps. After nephroscopy and ultrasonography confirmed that all the stones had been removed clearly, a 6F Double-J stent and a 16F nephrostomy tube were placed for internal drainage. No fluorosocopy was used in any PCNL procedure in our series.
All the patients were followed up with kidneys, ureters, and bladder (KUB) radiography at 48 hours postoperation. The nephrostomy tube was removed 5 to 6 days postoperation when KUB ultrasonography showed no residual calculus, and the Double-J stent was removed 3 to 4 weeks postoperation. Patients were followed up in the outpatient clinic of our hospital at 1 month and 4 to 6 months afterward using KUB radiography for determining the stone-free rate.
Results
Using SonixGPS navigation, PCNL was performed successfully by a single puncture in all 25 patients. Twenty patients were approached through an upper-pole percutaneous access, and the remaining 5 were accessed through the midpolar (n=3) and lower-pole (n=2) calices. The mean puncture time from puncture to successful establishment of the working tract was 5.5 (3–9) minutes, and the mean operative time was 74 (30–100) minutes. The complete clearance rate of PCNL was 92% (23/25) as shown by KUB radiography and ultrasonography 48 hours postoperation.
Only two (8%) patients had residual calculi after operation, including one who had residual fragments ≥8 mm, which were removed by flexible ureteroscopy 5 days after the initial operation. The other patient with residual fragments <8 mm was followed up. The mean length of postoperative hospital stay was 5.4 (4–11) days, and the mean decline in hemoglobin level was 6.18 (0–27) g/L. Four patients had transient postoperative fever, which responded well to antibiotics. No blood transfusion was needed in any patent. No patient had urine leakage for more than 1 day after nephrostomy. There was no injury to the adjacent organs or vessels.
Discussion
PCNL is the treatment of choice for large renal stones at present. 3,8 Ultrasonography and fluoroscopy are the two most commonly used image-driven treatment modalities in PCNL puncture. 2 Proper primary access to the renal collecting system can highly influence the complication rate of PCNL and clinical outcomes of the patients. 9 Nevertheless, obtaining an appropriate renal access remains the most difficult step of PCNL for many urologists. In the United States, 62.4% of urologists need percutaneous access to be performed in the radiology department before PCNL, and 33.8% of urologists obtain percutaneous access with the help of radiologists. 10
Ultrasonography as a common technology for puncture guidance and planning has been widely used with an overall success rate of 88% to 99%. 11 The primary advantages of ultrasonographic guidance include no ionizing radiation, no invasiveness, a short operative time, real-time visualization of surrounding structures, and detection of nonopaque stones. 12 Nevertheless, ultrasonographic guidance puncture is strongly operator dependent. In addition, it only offers two-dimensional images, and it is difficult to observe the whole length of the puncture needle. The urologist, especially the beginner, may misjudge the position of the needle tip under ultrasonographic guidance, easily causing a deeper puncture than anticipated.
Several new methods are reported to improve PCNL puncture efficacy, including electromagnetic field navigation of the puncture needle 13 and renal collecting system puncture with the help of the real-time electromagnetic tracking system using a sensor at the tip of the ureteral catheter in an in-vivo model of porcine ureter and kidney as reported by Rodrigues and colleagues. 14
The SonixGPS needle tracking system can display current and predict needle tip position at all times on the ultrasonography screen, thus enabling the operator to optimize the ultrasonographic image for the highest confidence in target visualization during advancement. The SonixGPS has two position sensors, including one embedded in the GPS arm transducer and the other in the tip of the GPS needle, allowing for inserting the GPS needle at any direction either in plane or out of plane with the transducer. As shown in our practice, the operator can keep track of the needle tip consistently during the procedure even when the needle and needle tip are not in-plane with the ultrasonographic image, knowing that the in-plane procedure is easier to perform, especially for the beginner, because the whole length of needle and needle tip are displayed on the screen and the orientation bars on the lower right side of the screen will help guide the needle and hand position.
Brinkmann and associates 5 and Wong and coworkers 6 believe that the SonixGPS can reduce the technical difficulty of real-time ultrasonography-guided spinal anesthesia. Kopac and colleagues 7 compared the SonixGPS needle-tracking ultrasonography technique with traditional ultrasonography for vascular access in a phantom gel model and found that the mental demand and effort were lower for the SonixGPS compared with the traditional ultrasonography-guided technique. These results indicate that puncture under SonixGPS can be performed with more ease and confidence compared with the traditional ultrasonography approach.
Our initial clinical experience and practice show that real-time ultrasonography-guided PCNL using SonixGPS navigation has many advantages. First, we can clearly predict and design the trajectory of the needle before PCNL puncture by means of the dotted lines that can display the expected depth, location, and angle of needle insertion, thus enabling the operator to select a perfect needle angle and direction that are safest and most comfortable for the patient. In addition, unlike normal ultrasonography puncture, the image of the trajectory of the needle and needle tip position are precisely displayed on the screen and will not be influenced by the puncture angle and depth.
Tanriverdi and coworkers 15 suggested that the window for surgical competence of PCNL with the help of fluoroscopy is about 60 cases. Our experience has shown that it is easier to perform puncture under SonixGPS navigation than normal ultrasound or fluoroscopy. Conventional ultrasonography puncture can be difficult for a beginner because the kidney seems moving with the patient's respiration during PCNL. The SonixGPS system can clearly show the trajectory of the needle and the location of the needle tip in a real-time manner so that he or she can adjust the puncture angle and depth to get excellent puncture.
This study had some limitations. We had no patient with a body mass index (BMI) >35 kg/m2 in this study, knowing that it is difficult for ultrasonography to image the kidney in patients with significant obesity or ectopic kidneys. In such patients or other difficult cases, fluoroscopic guidance is still needed. Because we have achieved access in all patients with a BMI <35 kg/m2, we believe that SonixGPS ultrasonography-guided PCNL is safe and feasible.
Conclusion
PCNL under the SonixGPS electromagnetic needle tracking system is safe, reliable, effective. and easy to follow, especially for beginners.
Footnotes
Disclosure Statement
No competing financial interests exist.