
Abstract
Objectives:
To evaluate the learning curve of robot-assisted partial nephrectomy (RAPN) and laparoscopic partial nephrectomy (LPN) between two surgeons at a single institution.
Methods:
A prospectively maintained, Institutional Review Board (IRB)-approved kidney surgery database was reviewed retrospectively and the first 116 consecutive LPNs performed by one surgeon (Hyung Kim) and 116 consecutive RPNs performed by a second surgeon (Thomas Schwaab) were identified. The learning curve was evaluated by examining the operative times, warm ischemia times (WITs), estimated blood loss, the postoperative estimated glomerular filtration rate (eGFR), and intra- and postoperative complications in the quartiles of 29 patients. The LPNs performed by Hyung Kim were done following completion of a minimally invasive fellowship. Thomas Schwaab had minimal experience with LPN and no fellowship training before starting RAPN.
Results:
The RAPN and LPN groups had similar patient and tumor characteristics. The RAPN group had a higher preoperative eGFR (74.1±22.04 vs. 80.95±21.25 mL/minutes, p=0.015) and a worse Eastern Cooperative Oncology Group (ECOG) performance status (ECOG 1+ in 12% vs. 2.6%, p<0.001) compared with the LPN group. Rates of intraoperative (p=0.203) and postoperative (p=0.193) complications were similar. In the RAPN group, operating room (OR) time (161±51 vs. 203±55 minutes, p<0.001) and WIT (17.7±14.8 vs. 21.8±9.1 minutes, p<0.001) were shorter. Postoperative stay was longer in the RAPN group (2.4±2.2 vs. 1.67±1.1 days, p<0.001). The percentage decrease in postoperative eGFR was lower in the RAPN group versus the LPN (9.6% vs. 10%). The learning curves differed for log tumor size, log WIT, and postoperative complications.
Conclusions:
The variables of the learning curve for RAPN can be obtained earlier than the same variables for LPN. RAPN had a shorter OR time and WITs. The shorter WITs, earlier in the series, led to consistently lower fluctuations in GFR and preservation of the renal function. The learning curves for each procedure need to be re-evaluated at longer intervals to ensure their accuracy.
Introduction
M
Nephron-sparing surgery (NSS) has become the standard of care for small renal masses demonstrating improved overall patient survival and superior preservation of kidney function when compared with traditional radical nephrectomy. 2 In recent years, the use of laparoscopic partial nephrectomy (LPN) and robot-assisted partial nephrectomy (RAPN) has increased. 3,4 The technical challenges of LPN limit its use to highly experienced laparoscopic surgeons. 5
Several retrospective studies have shown shorter learning curves for RAPN compared with LPN. However, a meta-analysis of these studies has demonstrated a majority of the learning curve literature, for NSS consists of retrospective reviews of small case numbers (<30 patients/series) with multiple surgeons with varying experience. 4,6 –9 We aimed, therefore, to define the learning curve of RAPN compared with LPN while attempting to minimize the amount of confounding factors by analyzing two surgeons with different training backgrounds in MIS at the same institution over a large number of consecutive cases.
Patients and Methods
A prospectively maintained, Institutional Review Board (IRB)-approved kidney tumor database was analyzed. Out of a total of 650 patients, we identified the first 116 patients to consecutively undergo LPN by one surgeon (Hyung Kim) and the first 116 to consecutively undergo RAPN by a second surgeon (Thomas Schwaab) were analyzed and compared. The LPNs performed by Hyung Kim were the first cases preformed after completing a minimally invasive fellowship. Thomas Schwaab did not undergo fellowship training nor have experience with LPN before starting RAPN, but did have prior robotic prostatectomy experience.
Demographic and patient characteristics were recorded, including patient age, gender, body–mass index, Charlson comorbidity index, Eastern Cooperative Oncology Group (ECOG) performance status, pre- and postoperative estimated glomerular filtration rate (eGFR), and tumor size. R.E.N.A.L nephrometry scores were determined by a retrospective review of imaging and were available for 99 of the LPN group and 111 of the RAPN group. Patient characteristics were compared between LPN and RAPN using the Mann–Whitney U and Fisher's exact tests for continuous and categorical variables, respectively. 10
Perioperative outcomes were compared between the two groups, including operative time, estimated blood loss, transfusion rate, length of stay, positive margin rate, and complications. Operative time was defined as the amount of time elapsed from the patient entering the operating room (OR) to exiting the OR. Conversions to open surgery or radical nephrectomy were recorded. Complications were recorded as any deviation from the normal postoperative course within 30 days of operation. Complications were categorized according to the Memorial Sloan-Kettering system and graded using the Clavien–Dindo grading system. 11,12 Anemia was defined as the need for postoperative blood transfusion, and ileus was defined when delay in bowel function prolonged the hospital stay or required placement of a nasogastric tube.
Renal function outcomes were compared using postoperative change in eGFR. This was calculated using the Chronic Kidney Disease Epidemiology Collaboration formula. 13 Postoperative change in eGFR was calculated at the latest postoperative visit within 12 months of surgery.
Cohort comparisons, between surgery types and experience levels, were made using the Wilcoxon rank-sum and Fisher's exact tests for continuous and categorical variables, respectively. Confidence intervals are obtained for complication rates, associated surgery experience groups, using the Wilson method. The association between continuous perioperative outcomes and both surgery and experience was evaluated using linear regression models, with all assumptions verified graphically and transformations applied, as appropriate. The association between complication rates and both surgery and experience was evaluated using logistic regression models; fit using Firth's penalized likelihood method. The interaction terms in the regression models allow for comparison of the learning curves between surgery types and for other comparisons across surgery types and experience levels, as appropriate. The Holm–Bonferroni method was used to obtain adjusted p-values. All analysis was conducted in SAS v9.3 (Cary, NC) at a nominal significance level of 0.05. Therefore, a p-value <0.05 is considered statistically significant.
Results
The patient characteristics for the 232 patients included in this analysis are listed in Table 1. Demographics were similar between the two groups. Notably, the RAPN group had a poorer ECOG performance status (ECOG 1+ in 21.6% vs. 12%, p<0.001) and a higher preoperative eGFR (80.95±21.25 vs. 74.1±22.04 mg/mL, p=0.015) compared with the LAPN group.
BMI=body–mass index; CCI=Charlson comorbidity index; ECOG=Eastern Cooperative Oncology Group; GFR=glomerular filtration rate.
Patient demographic and clinical characteristics were summarized by quartiles (n=29 surgeries/quartile) and compared between the RAPN and LPN. In the first quartile, we observed differences between the RAPN and LPN: ECOG, preoperative and postoperative GFR, OR time, and percent change in GFR at last follow-up (Table 2). The RAPN group had shorter OR times (172±53 vs. 228±50 minutes, p<0.001) compared with the LPN group. Both groups had significant decreases in eGFR: RAPN −14.5% (−11.3 mg/mL, p=0.03) versus LPN −15.2% (−11.9 mg/mL, p=0.8) at last follow-up, respectively (Fig. 1).

Change in glomerular filtration rate (GFR) per quartile.
EBL=estimated blood loss; OR=operating room.
In the second quartile (Table 4), the RAPN cohort had larger tumors (4±2 cm vs. 2.9±1.1 cm, p=0.012) and shorter warm ischemia times (WITs; 19.6±17.8 vs. 22.1±8.4 minutes, p=0.032), but there was no significant difference in the OR time (p=0.225) (Table 3). However, the RAPN patients had a higher rate of intraoperative complications (21% vs. 0%, p=0.023), transfusions (3.4% vs. 25%, p=0.67), and a longer postoperative stay (2.8 vs. 1.9 days, p=0.034). The RAPN group had a larger decrease in eGFR [−15.4% (−11.9 mg/mL, p=0.3)] versus the LPN group [−6.5% (−4.56 mg/mL, p=0.35)], respectively (Fig. 1).
In the third quartile, there were significant differences in the OR time, WIT, and percent change in eGFR postoperatively in favor of RAPN patients: shorter OR time (142±47 vs. 200±58 minutes, p<0.001), shorter WIT (13±9 vs. 19.2±7.8 minutes, p=0.015), and smaller decrease in eGFR at last follow-up [−4% (−3.03 mg/mL, p=0.5) vs. −15% (11.1 mg/mL, p=0.04)] of LPN, respectively (Fig. 1).
In the fourth quartile (Table 5), RAPN patients had a shorter OR time (143±41 vs. 176±47 minutes, p=0.019), shorter WIT (13.4±6 vs. 19.6±9 minutes, p=0.005), as well as a smaller decrease in eGFR at last follow-up [−4.5% (−3.5 mg/mL, p=0.4) vs. −6% (−4.1 mg/mL, p=0.5)] in comparison with the LPN (Fig. 3).
A total of 82 patients experienced intra- or postoperative complications. Rates of complications were similar between the RAPN and LPN groups, including intraoperative (13.8% vs. 7.8%, p=0.203) and postoperative complications (32.8% vs. 25%, p=0.193) (Fig. 2). Of those patients, 28 and 25 experienced a single postoperative complication and 10 and 4 experienced multiple postoperative complications in the RAPN and LPN groups, respectively. High Clavien grade (III and IV) complications were seen in six patients in each group.
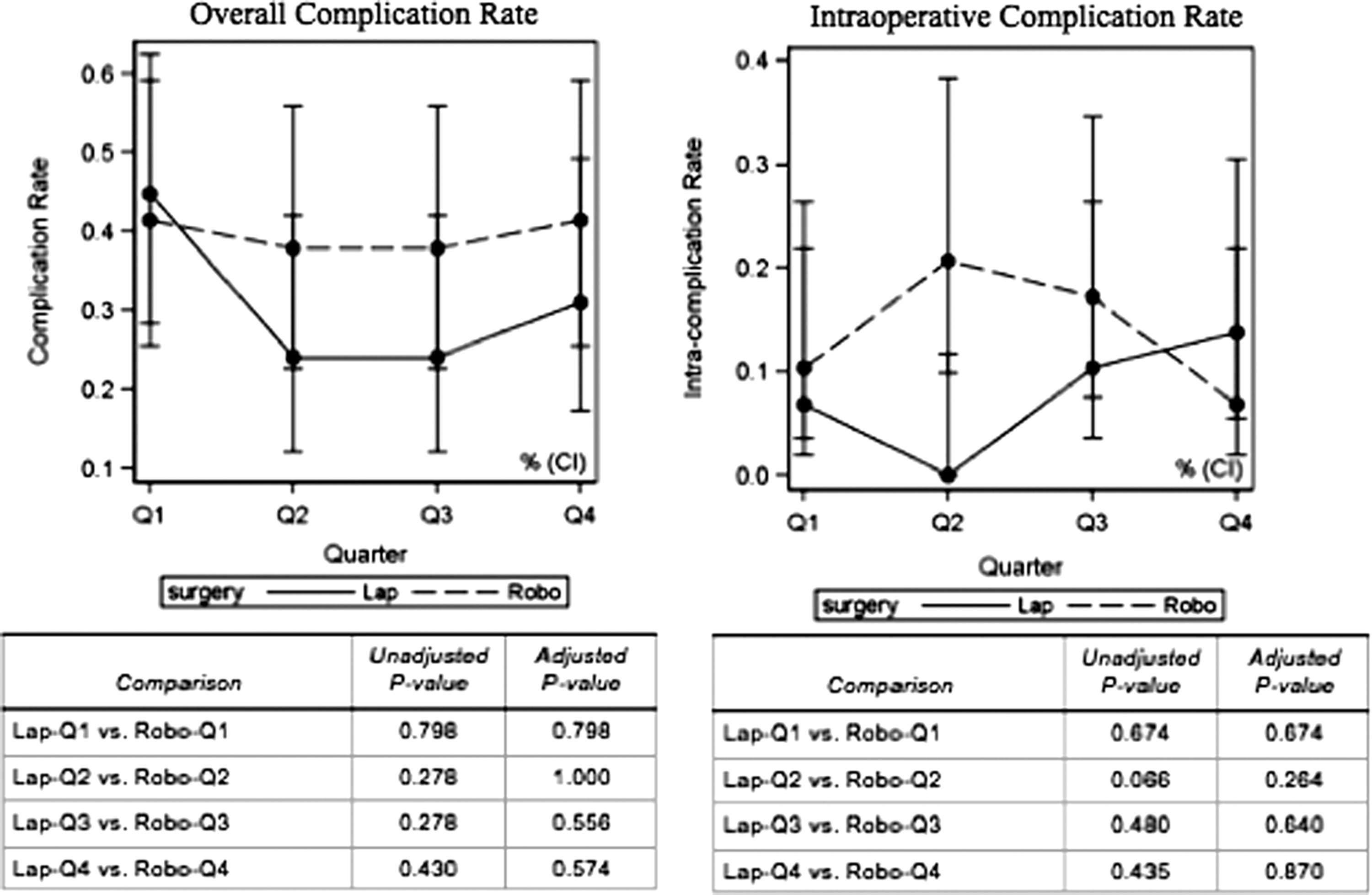
Complication rate.
To gauge surgeon improvement, the learning curves for each parameter were assessed. The learning curve for WIT demonstrated a significant difference in the third and fourth quarter. RAPN showed a superior WIT in both the unadjusted and adjusted p-value. The incidence of intraoperative complications demonstrated no significant difference, despite an initially higher incidence in the RAPN group (Fig. 2).
The learning curves for both surgery types were assessed using linear and logistic regression models. There was an overall beneficial effect of time observed from the first surgery for both surgical approaches, which showed an increased tumor size, decreased WIT, and decreased postoperative complications (Figs. 2 and 3). Comparing the learning curves for the RAPN and LPN log tumor size showed a decreased difference over time, RAPN decreased faster for log WIT and LPN decreased faster for postoperative complications (Figs. 2 and 3).
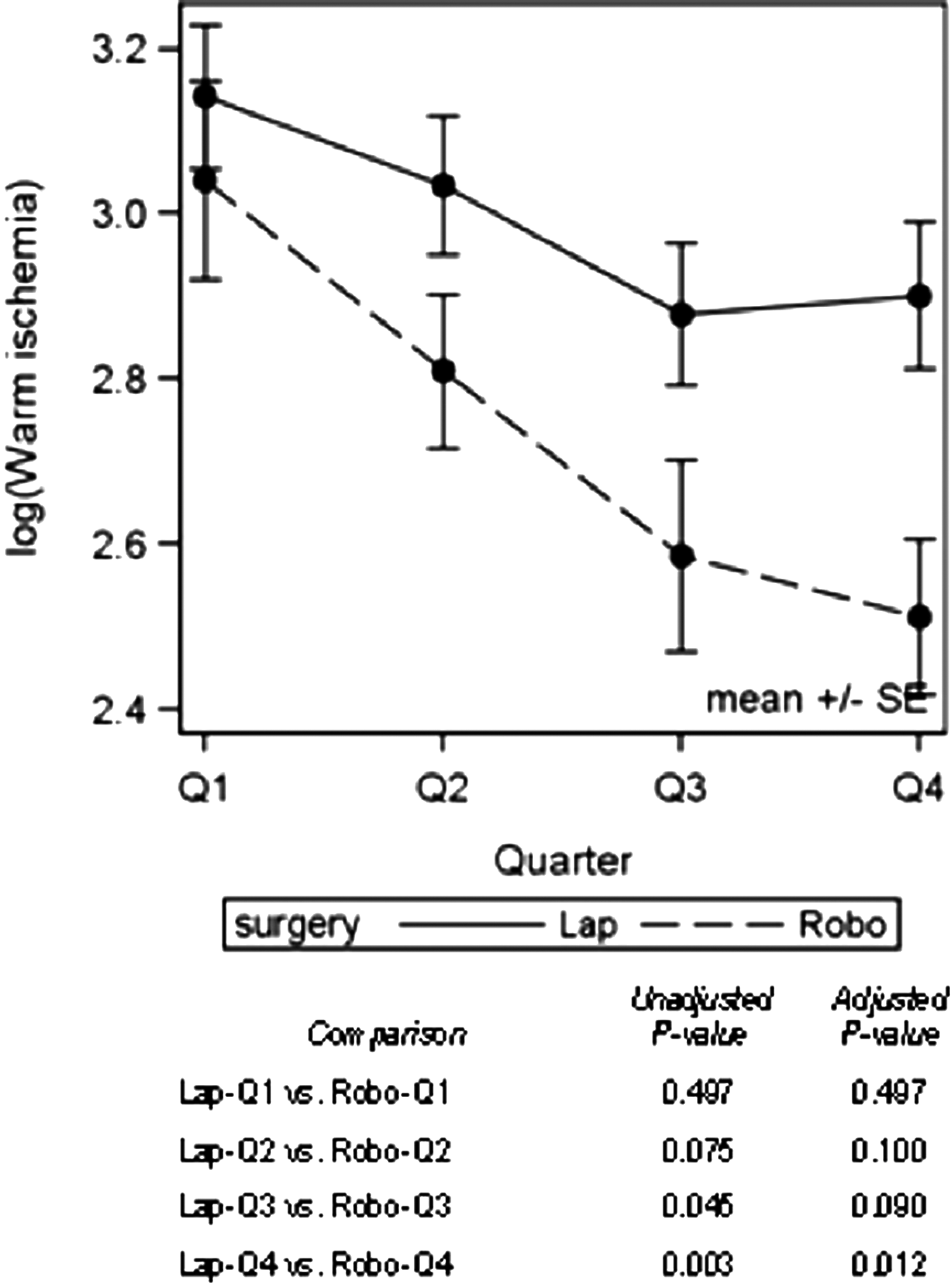
Warm ischemia time.
Discussion
Minimally invasive partial nephrectomy has gained increased acceptance over the past years. However, LPN is a technically challenging procedure that is, in most facilities, limited to highly trained and experienced laparoscopic surgeons. The advent of robotic technology has eased the transition from open surgery to a minimally invasive approach, but its acceptance in minimally invasive partial nephrectomy has been significantly slower. We set out to investigate the benefits of robotic technology for a surgeon with minimal LPN experience by comparing his first 116 cases with the first 116 cases of a fellowship trained, experienced laparoscopic surgeon during his learning curve, following fellowship training.
Proficiency at LPN, obtained through experience or fellowship training, portends a benefit in a shorter learning curve for RAPN. 7,8,14 We demonstrated that the RAPN learning curve was significantly shorter than the LPN learning curve, even with a lack of minimally invasive fellowship training. In the first quartile of the learning curve, RAPN provided a shorter overall OR time, despite the need to dock the robot, and a shorter WIT; this is mirrored by superior long-term renal function for RAPN patients. Traditionally, robotic surgical series account only for the console time when calculating the OR time, however, we felt as part of the learning curve, we needed to incorporate the total amount of time the OR staff would take to set up and dock the robot to accurately reflect the differences between the two cohorts.
In the second quarter, the RAPN group maintained a shorter WIT, but overall OR times were similar to LPN. This may be a result of increasing comfort of the LPN surgeon with the procedure or increased comfort of the RAPN surgeon in the participation of fellows, thus prolonging the surgical procedure. During this portion of the learning curve, the RAPN group also comprised larger tumors and higher intraoperative complication rates and transfusion rates. Again, this may be due to the RAPN surgeon's increased comfort with this technique, which may have led him to approach more complex tumors. The second half of the learning curve demonstrated persistent superior WIT and long-term renal function in favor of RAPN. It is important to note that the overall intra- and postoperative complication rates were similar, although the intraoperative complication rate was higher for the RAPN in the second quartile. This may again be reflected by the robotic surgeon's desire to push the envelope, as evidenced by the larger tumor size. In addition, during the second quartile, we see a significant decrease in postoperative eGFR that is maintained throughout the remainder of the RAPN series compared with the LPN series, which demonstrates a sigmoid curve.
The challenge in defining the learning curve of any procedure is identifying the exact number of times a task must be completed before mastery is established. Several previous authors have alluded to the learning curve, but yet there still remains no clear definition of how many number of cases must be done to obtain mastery. Mottrie and associates defined a completed learning curve for RAPN as a WIT of 20 minutes or less and a robotic console time of 100 minutes or less. 9 Nadu's commentary regarding these measurements of the robotic learning curve criticized the use of WIT and console time as soft parameters referencing surgeons bias to select for patients who would produce favorable outcomes. 15 The author suggested rather hard parameters such as the perioperative complication rate, which Nadu believes to be more difficult to select for. Taking this concept into consideration in our series, it is clear that the RAPN learning curve for WIT was reached earlier than the LAPN learning curve (between the first and second quartile for RAPN and second to third quartile for LAPN). Comparing complication rates (including intraoperative and perioperative), it would appear that our series could not definitively define the complication rate learning curve as it continued to vary with no significant drop-off between each quartile of either cohort. Operative times were better defined with a gradual decline in the robotic cohort while the laparoscopic continued to vary. Link and associates demonstrated the operative times continue to drop beyond 150 cases; thus, our laparoscopic cohort may have not hit their optimal operative times in our series. 16
This study uniquely reviews a large series of consecutive cases for only two surgeons, one fellowship trained in laparoscopy and one with no further training beyond residency. Aboumarzouk and associates preformed a meta-analysis of RAPN versus LPN comparing outcomes and one of the key flaws found in their review was the large number of surgeons with varying levels of experience who were used to compare RAPN and LPN. 6 The effects of the individual's experience could contaminate the overall results with advanced fellowship or operative experience by changing the outcomes. 6,17 The surgeon skill despite additional training, is an additional confounding factor that should be considered when closely examining the data. Despite additional fellowship training, the operative skills between two individual surgeons need to be considered. An additional flaw identified in a review of the meta-analysis was the low number of RAPN performed in each series. Only three retrospective series had more than 33 RAPN and the series with the greatest number of RAPN was 108, but included five surgeons. 6 One could argue that the NSS learning curve for MIS, as demonstrated by the robotic prostatectomy data, could not be completely elucidated by such a small number of cases and large number of multiple surgeons. 18,19
In summary, this is the first study to compare LPN and RAPN learning curves with a large consecutive patient cohort for only two surgeons. It is limited by its retrospective nature and its single institutional experience. These results demonstrate that RAPN provides the novice minimally invasive partial nephrectomy surgeon with the means to achieve adequate surgical and postoperative outcomes. The true learning curve for partial nephrectomy is still yet to be fully defined, a further prospective series with a large number of patients is needed to help clarify the learning curve to further improve training in RAPN.
Conclusions
RAPN is a safe and effective alternative to LPN with similar complication rates for surgeons without significant LPN experience. The RAPN learning curve reaches shorter OR and WITs earlier and preserves the eGFR 6 to 12 months postoperatively and more effectively.
Footnotes
Disclosure Statement
No competing financial interests exist.