
Abstract
Purpose:
To evaluate the safety and efficacy of a novel robotic tissue ablation system (PROCEPT Aquablation™ System), in performing prostate ablation in a survival canine model.
Materials and Methods:
This novel technology uses a high-velocity saline stream that aims to selectively ablate prostatic glandular tissue while sparing collagenous structures such as blood vessels and capsule. Once the ablation is complete, a laser beam is captured by a low-pressure water jet to produce surface hemostasis. The extent and depth of ablation is predetermined by endoscopic and transrectal ultrasonography guidance. The procedure was performed in eight noncastrated male beagles aged 6 years or older (Acute 2, Chronic 6) through a previously created perineal urethrostomy.
Results:
Aquablation time ranged from 40 to 84 seconds (mean 60.5 sec). There was no active bleeding in any of the dogs during or after Aquablation. Water jet-guided laser coagulation was used for purposes of monitoring its safety and efficacy. Five of the six dogs reached the predetermined 6-week mark. Complications included two dogs with infection successfully treated with antibiotics, a false passage created during catheter placement, and two bladder neck perforations (from mechanical insertion), one leading to euthanasia. Histologic evaluation at 6 weeks revealed a normal cellular architecture and full reepithelialization of the treatment cavity.
Conclusions:
We report the initial survival data in the animal model of a novel robotic device developed for managing symptomatic benign prostatic hyperplasia (BPH). Aquablation produces ablation of adenomatous elements while preserving collagenous structures and is a promising technology for surgical management of symptomatic BPH.
Introduction
B
In this study, we evaluate a novel image-guided ablation device of prostatic tissue (PROCEPT Aquablation™ System, PROCEPT BioRobotics, Redwood Shores, CA). This integrated system delivers a high-pressure water jet under precise electromechanical control. The water jet selectively ablates prostatic glandular tissue preserving collagenous structures such as blood vessels and prostatic capsule, a process called aquablation. A surgical laser unit delivers laser energy, as needed, through a column of water, resulting in precise and energy efficient surface hemostasis. Aquablation may result in rapid removal of prostate tissue, thereby allowing it to be used for management of small to large prostates.
We evaluate the safety and efficacy of aquablation as a prostatic ablation technique in an acute and chronic survival animal model.
Materials and Methods
Aquablation device
The PROCEPT Aquablation System consists of two major components, the Aquablator™ handpiece and the Aquablator console (Fig. 1A, B, C). The Aquablator handpiece is composed of a reusable, sterilizable handle as well as a single use, sterile, disposable cutting probe, the AquaBlade.™ The handpiece enters the patient's urethra via a custom rigid cystoscope of approximately 24F in diameter with an integrated fiberscope for real-time visualization. The cystoscope has an inflatable balloon at the tip, which can be expanded inside the bladder for anchoring and isolation.
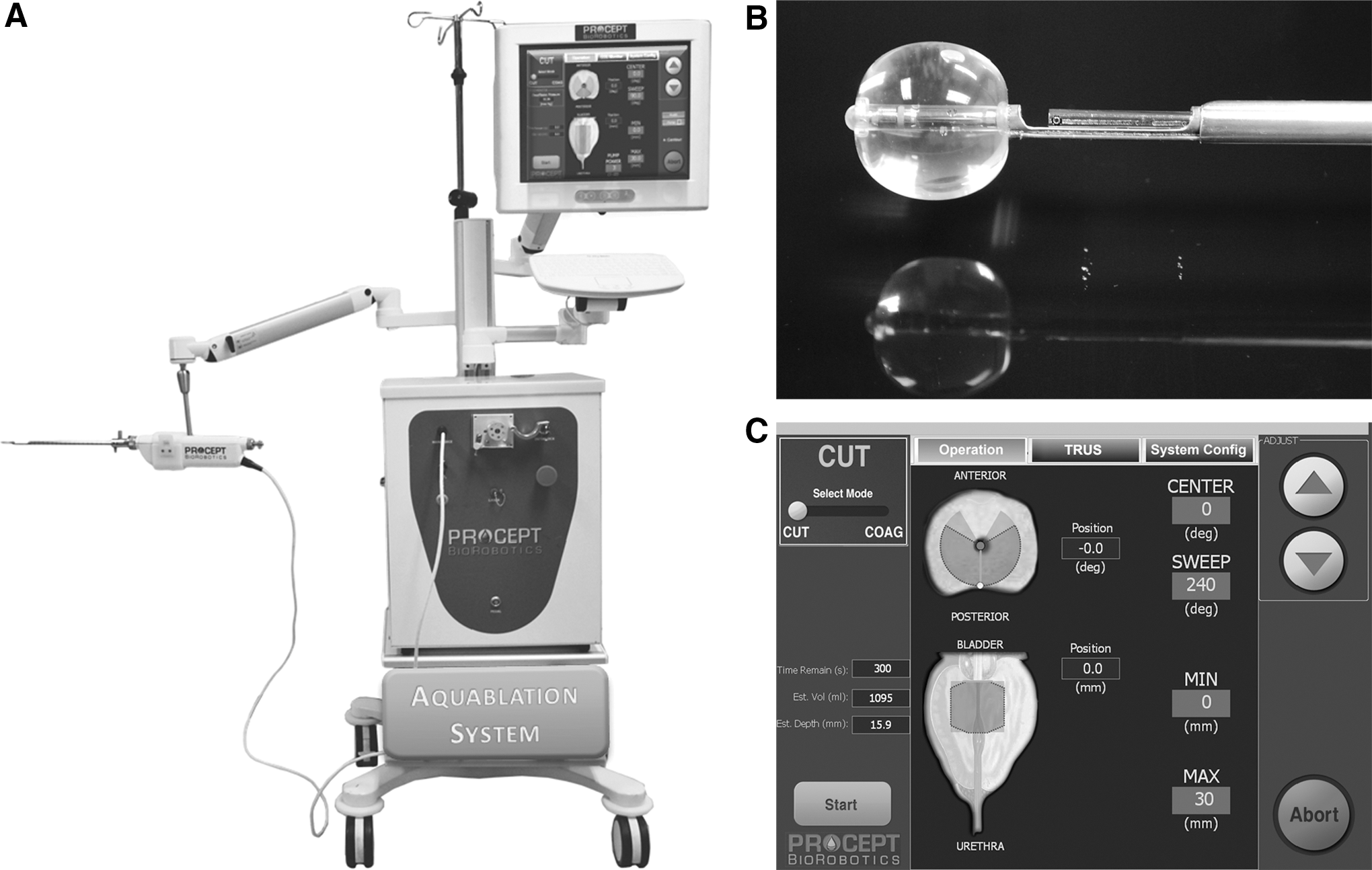
As depicted in Figure 2, the disposable probe is placed into the cystoscope and into the prostatic urethra. The cystoscope has a cutaway portion, allowing exposure of the distal end of the probe. Driven by the motors within the handpiece, the probe can rotate axially and move longitudinally (in and out) along the length of the prostate. The distal tip of the energy probe has a nozzle that emits a jet of saline orthogonal to the probe. Precise axial and longitudinal motion allows the jet to be directed toward any part of the inner prostatic urethra. At high pressure, the water jet emanating from the probe's distal end resects tissue via tissue-selective ablation, also called aquablation. At low pressure, the water jet forms a collimated stream of water, thereby acting as a wave guide for the delivery of highly focused laser energy to the inner wall of the prostate, which can be used for precise surface cauterization after ablation. Moreover, the column of water acts as a simultaneous rinsing system, allowing laser energy to be applied directly to isolated tissue. For the surgeon's convenience, the handpiece is mounted on a fully adjustable articulating arm system as shown in Figure 1A.

Prostate ablation using the PROCEPT Aquablation System. Purple arrow shows the cystoscope. Green arrow shows high-pressure water jet emanating from the energy probe aimed at the inside of the prostate The jet can be rotated axially and moved in and out between the distal (verumontanum) and proximal (bladder neck) ends of the prostate. Blue arrow shows illumination ports; red arrow, the camera port.
The sterile, single-use probe consists of tubing to route the sterile fluid from the saline bag to the console's pump as well as a fiberoptic connector to connect to the console's laser unit. Sterilization of the probe is performed using ethylene oxide. When removed from its sterile packaging, the probe is inserted and locked into the handpiece from its rear port. On completion of the aquablation procedure, the AquaBlade can be unlocked, removed, and disposed. The handpiece is designed to be cleaned and disinfected via steam sterilization.
The console is an integrated system designed to precisely control the probe's movement, laser output, and fluid pressure during the aquablation procedure. The handpiece connects to the console via a detachable, water-resistant electrical cable. The probe within the handpiece is directly connected to the console's fluid pump as well as its laser unit. To maintain the sterile fluid path between the saline bag, the probe attaches to the console's pump via its inline disposable cartridge. The cartridge can be locked to and removed from the pump with a turn of a latch. As an extension of the console, a touch screen provides the user a graphic control interface, as seen in Figure 1C.
During the first phase of aquablation (i.e., the cutting mode) the user has the ability to adjust angle, length, contour, and depth of tissue penetration. On pressing start, the console activates the pump that drives physiologic saline (0.9%) through the probe's nozzle at pressures ranging from 500 to 8000 pounds per square inch (PSI) to cut and dissect soft tissue at the predetermined system parameters. During the coagulation phase, the console drives the pump at low pressure (∼5–15 PSI) and activates the 2 W green light laser (532 nm) to allow for cauterization after resection. At 2 W, the Aquabeam has a power density of 6366 W/cm2. This is well within coagulation range.
Survival study
The chronic survival study was undertaken in eight noncastrated male beagles, at least 6 years of age or older after obtaining approval from the Institutional Animal Care and Use Committee (IACUC) at our institution. The dogs were allowed 2 weeks for habituation to the animal facilities at the University of Southern California, as per animal resources protocol. A veterinarian performed general anesthesia and monitored postoperative care. The experiment was conducted in two steps. Because the male dogs have a penile bone, step 1 necessitated surgical creation of a perineal urethrostomy to allow transurethral access to the prostate via rigid instrumentation. The technique of perineal urethrostomy in the dog has been described earlier. 1 The urethrostomy was created and allowed to mature for 2 weeks after which aquablation was performed. The first two dogs were euthanized immediately after aquablation, and the remaining 6 dogs survived for 6 weeks.
The Aquablation settings were based on the prostate dimensions. The length of the excursion was based on the length of the prostatic urethra, and the power (depth of penetration) and degree of rotation were based on the prostatic height and width. The AquaBlade was intermittently replaced with a flexible ureteroscope to monitor progress of the ablation. The ablation accuracy was also monitored by real-time TRUS imaging in the transverse and sagittal planes. In general the tip of the probe and depth of ablation were better appreciated in the sagittal view, and the rotation angle was better monitored in the transverse view. When satisfied with adequacy of the ablation based on endoscopic visualization (Fig. 3) and TRUS (Fig. 4), the prostatic fossa was surface-coagulated using the 2W GreenLight laser, following the same axial and longitudinal direction as the ablation.
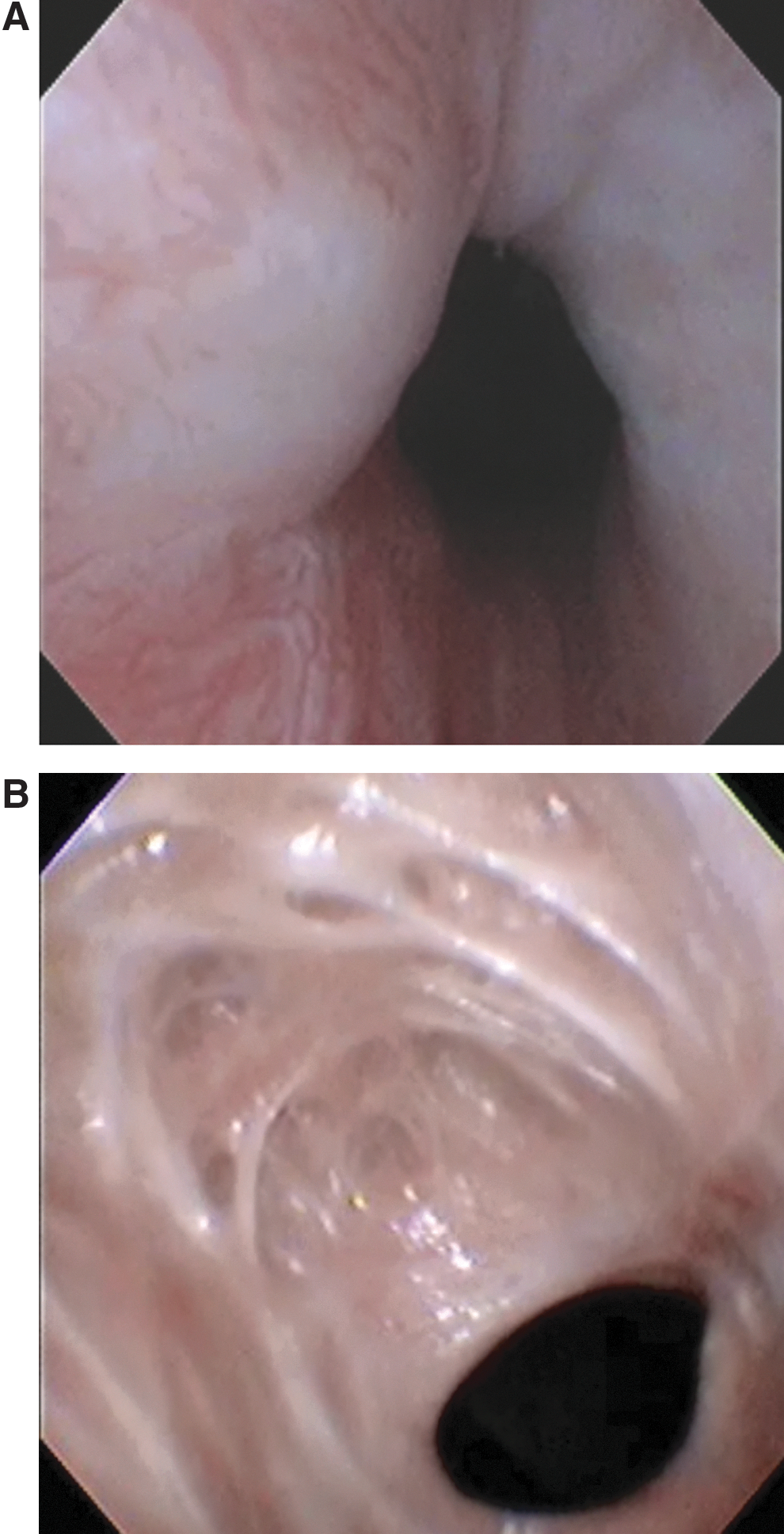
Cystoscopic view (
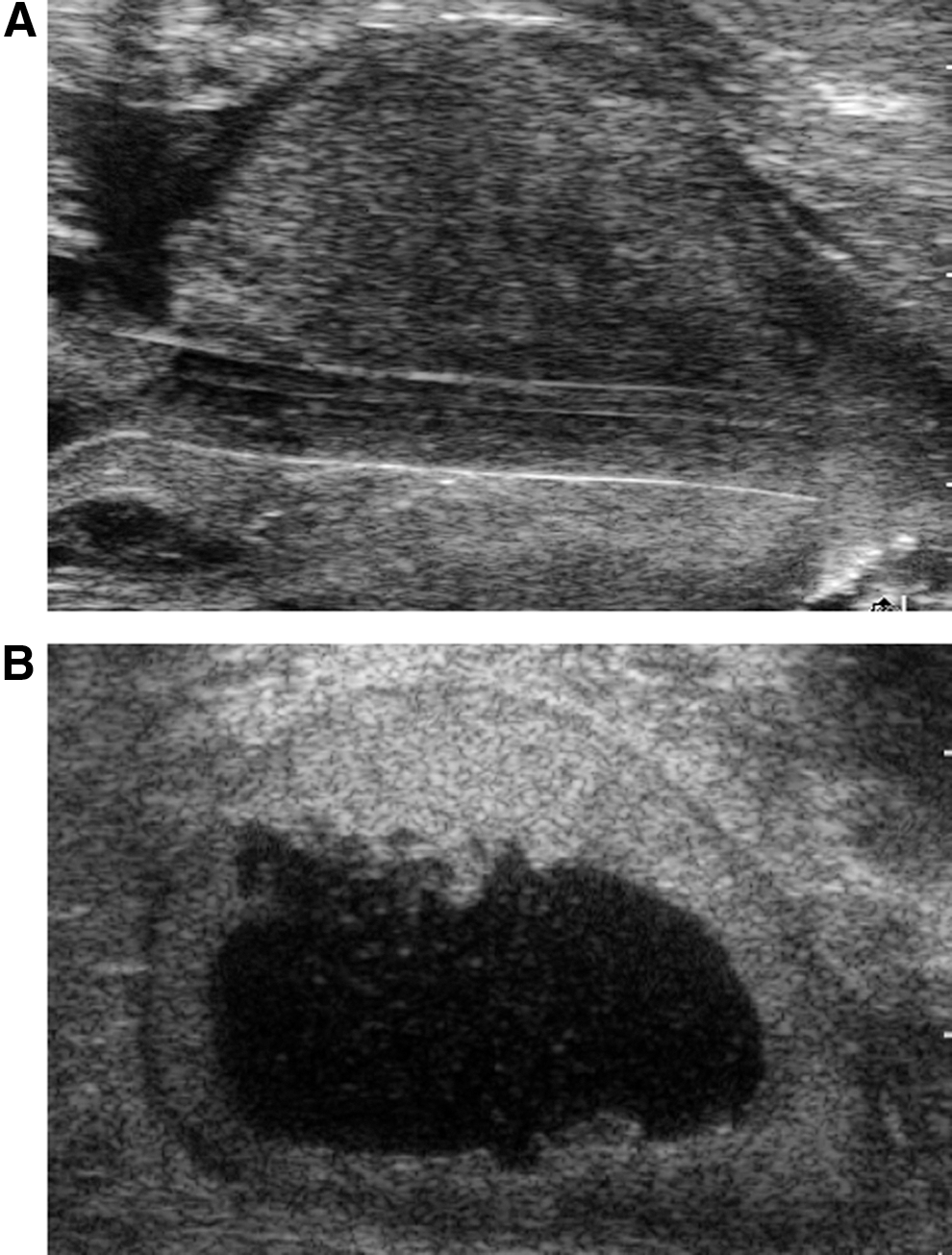
Transrectal ultrasonography of the prostate (
All dogs were given one preoperative dose of antibiotics in the form of oral cephalexin, followed by two more doses to complete a 24-hour course. No catheter was placed in dogs 3 and 4, the first dogs to undergo the survival study; however, both experienced a urinary tract infection, and the decision was made for the remaining dogs to all have a Foley catheter postoperatively; catheters were removed after 1 week.
The dogs survived for 6 weeks after aquablation and were monitored for complications. The study veterinarians euthanized the dogs per standard protocol.
Pathology
Immediately after euthanasia, prostates were removed, weighed, bisected, measured, and photographed (Fig. 5). After being fixed in 4% formalin, prostate tissue was serially sectioned at 3 to 5 mm, microsectioned (5–7 ìm), and stained with hematoxylin and eosin (H&E, Sigma Chemical Co., St. Louis, MO) and Masson trichrome. The depths of ablation as well as coagulation zones were measured after H&E and Masson trichrome staining by light microscopy with the use of a calibrated caliper.
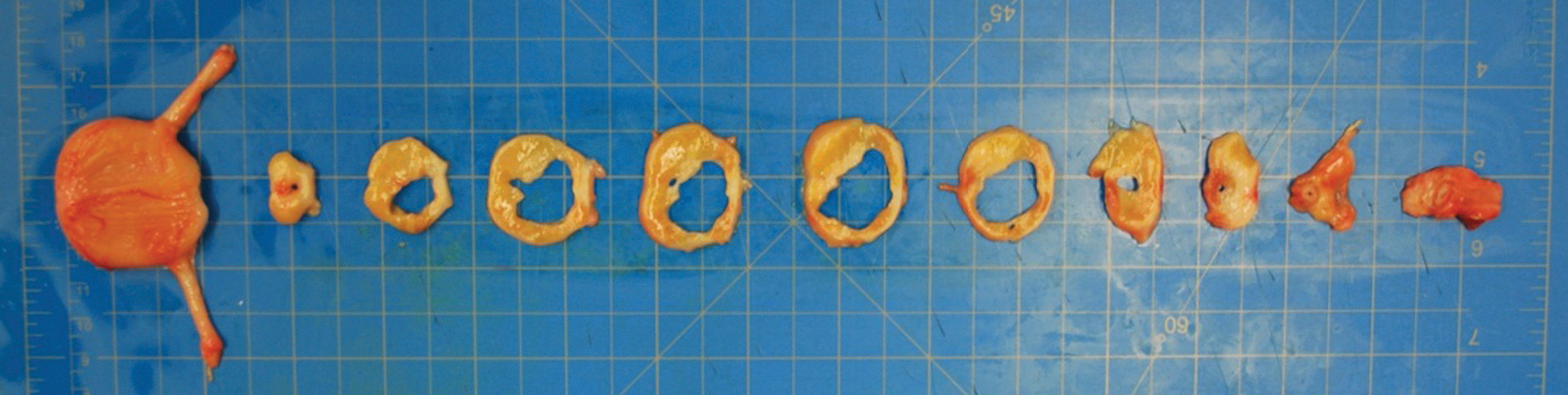
Serial sectioning of the prostate after harvesting showing the open prostatic fossa.
Results
Table 1 details the baseline demographics and TRUS findings. The ages ranged from 5 to 10 years (average 7.75 years), and prostate volume ranged from 16 to 34 cm3 (average 25.5 cm3). Table 1 summarizes technical details for the Aquablation procedure. The duration of Aquablation ranged from 40 to 84 seconds (average 60.5 sec). There was no active bleeding in any of the dogs during or after Aquablation. Laser coagulation of the ablative surface was nevertheless performed for purposes of monitoring safety and efficacy. Laser cauterization time ranged from 180 to 500 seconds (average 372 sec).
TRUS=transrectal ultrasonography.
Complications and sequelae are detailed in Table 2. Five of the six dogs that underwent survival study survived up to the 6-week mark. One dog was euthanized before the target 6 weeks survival because of abdominal distention and sepsis secondary to intraperitoneal bladder rupture. An additional dog had an intraperitoneal rupture that was successfully repaired, and the dog survived uneventfully until 6 weeks. In both cases, the rupture was at the bladder neck, and the ablated prostatic fossa was intact. Two dogs had urinary tract infection, and both were treated successfully with antibiotics. One dog had a false passage created during cystoscope placement at the start of the procedure, but the procedure was completed successfully and a catheter was left for 2 weeks to allow for healing. Another dog was found to have the sheath of the Aquablator placed into the ureter, and hence the procedure was aborted. No injury was noted and the dog recovered well and the procedure was completed a few weeks later; the dog survived to planned euthanesia.
UTI=urinary tract infection; OR=operating room.
The two complications related to perineal urethrostomy were both infections of the urethrostomy. One was successfully managed with antibiotics and removal of a suture in the area of infection. The other necessitated take-back to the operating room for opening of the perineal incision, which was irrigated and reapproximated with suture and healed with antibiotics.
Gross anatomic examination revealed intact capsular architecture with a widely patent lumen between the peripheral sphincter and bladder neck (Fig. 5). In the acute cases, histologic examination revealed a newly created lumen devoid of epithelium surrounded with normal cellular architecture beyond a 0.4 to 0.5 mm zone of swollen cells. In the chronic cases, the prostatic urethra maintained a widely patent lumen, and the urethral channels were lined by several layers of epithelium supported by a 0.4 to 0.5 mm thick layer of regenerative fibromuscular and elastic stroma underneath. Cellular structures beyond this zone were essentially normal and unaffected by the treatment application (Fig. 6).
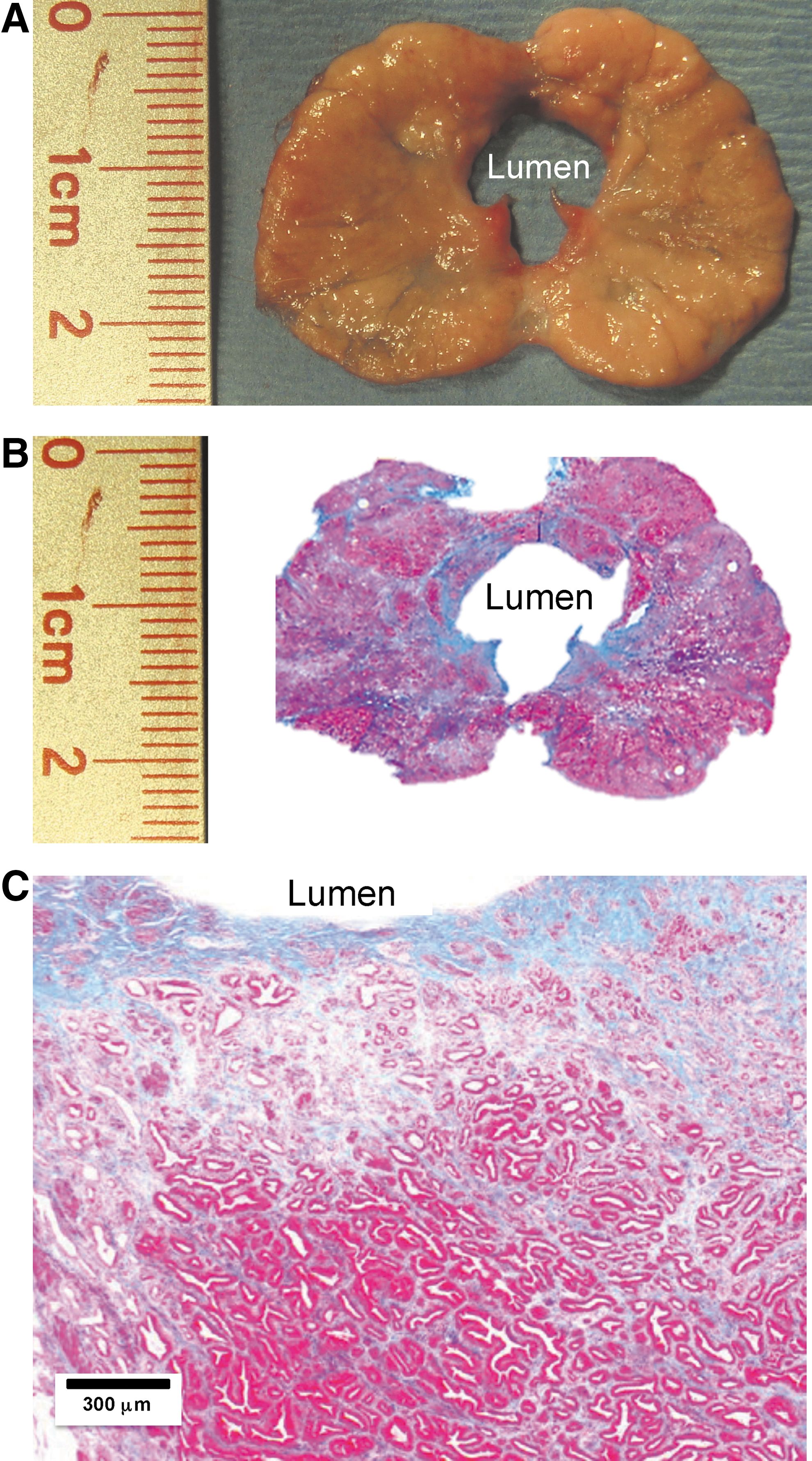
Histologic comparison with the gross view of the prostate harvested at 6 weeks after aquablation. (
Discussion
BPH is the most common cause of bladder outlet obstruction in men. Despite the advent of several novel surgical techniques for treatment of BPH, TURP still remains the gold standard. Although the technique of TURP has been widely practiced over the last several decades, complications are seen in up to 20% of patients following a successful intervention. 2,3 Several new transurethral procedures for management of BPH have emerged with an attempt to further reduce the morbidity of TURP. These techniques include resection, ablation, or enucleation of the prostatic adenoma using either bipolar current or a variety of lasers. Ablative techniques in general are easier to perform than enucleative techniques but are limited by the size of the prostate that can be efficiently ablated. Experience with photoselective vaporization has demonstrated shorter duration of catheterization and reduced bleeding but longer operative times when compared with TURP. 4,5
High-pressure water jet technology has been adapted to dissect parenchymal tissues in animal models and in humans. Medical application of water jet technology was first described for liver resection for selective dissection of liver parenchyma, leaving bile ducts and blood vessels intact. 6 –8 Subsequently, this was extended to a wide range of parenchymal organs such as the brain, kidney, and lungs. 9 –12 When appropriately calibrated, water jet can achieve precise parenchymal ablation preserving collagenous structures such as blood vessels, bile ducts, etc. More recently, similar hydrodissection and water jet technology have been used transurethrally for resection of bladder tumors. 13 This study found that all tumors could be resected en bloc, and the lamina propria was intact, allowing the pathologist to distinguish between superficial and invasive tumors.
The development of the aquablation technology for BPH is based on the hypothesis that the high-pressure water jet will preferentially ablate the adenomatous tissue, preserving collagenous structures such as surgical capsule, bladder neck, and blood vessels. The low-power laser is trapped in a low-pressure jet to provide superficial hemostasis of the prostatic fossa. In the present study, ablation was successfully planned and monitored real-time using TRUS guidance to achieve rapid and precise ablation of the transitional zone. In the present study, we could visualize important transurethral landmarks such as the bladder neck, verumontanum, and the extent of prostatic adenoma with TRUS. The ablation was rapid as evidenced by the Aquablation time.
Most complications were secondary to the anatomic and technical limitations specific to the animal model. The steep urethral angulation and penile bone necessitates creating a perineal urethrostomy for rigid endoscopic access in male beagles resulting in a few complications. The urethral diameter in the beagles is small, which necessitates dilation before introduction of the sheath. Moreover, the canine prostate is quite separate from the bladder with the intervening unsupported and flimsy bladder neck predisposing to tears and extravasation from this site. Last, the beagle has a small bladder capacity with a relatively weak wall. Two intraperitoneal bladder perforations occurred at the bladder dome, likely related to the small size of the beagle bladder.
Urinary extravasation at the bladder neck occurred during dilation in two animals, and this was detected clinically even before the ablation was started. In no case was there perforation of the prostate capsule from the high-pressure water jet. Also, there was no significant bleeding from the prostate fossa. The minor surface oozing was successfully controlled with the low-power superficial laser coagulation.
Aquablation may have several potential advantages in the surgical management of BPH. It may provide a significantly faster rate of ablation compared with other thermal ablative technologies, thereby reducing operative time and enabling treatment of larger glands. In addition, there is no thermal energy applied for aquablation, and the minimal laser energy for final hemostasis may not be needed in most cases. A further advantage is the ability of this ablation to be applied in an automated, controlled fashion, without the pitfalls of manual use. The axial and longitudinal rotation of the probe coupled with the ability to anchor the unit in position allows the procedure to be performed only with original placement of the handpiece and monitoring of progress with the cystoscope. These advantages, however, must be proven by clinical trials in patients with BPH and are currently under way.
The limitations to this study include a limited supply of beagles available for use. Unfortunately, these eight beagles were the only available that met the appropriate criteria for our study as well as the IACUC at our institution during the time frame of our study. Because the equipment was developed and designed for human use, performing the procedure on beagles is a limitation itself. The differences in anatomy between humans and beagles provided some technical challenges and likely inflated the complications.
Conclusions
High-pressure water jet appears to be safe and effective in achieving precise and rapid ablation of prostatic tissue in the animal model. Our survival animal study confirms the safety of the robotic image-guided ablation technology. Clinical evaluation of this novel technology is currently under way in patients with symptomatic BPH.
Footnotes
Disclosure Statement
Nikolai Aljuri and Surag Mantri are owner and employer of Procept BioRobotics, which is the company that has developed the technology. Mihir Desai is a consultant for Procept. For the remaining authors, no competing financial interests exist.