
Abstract
Purpose:
We analyzed the technical feasibility, physiological influence, and safety of transvaginal (TV) and transrectal (TR) natural orifice translumenal endoscopic surgery (NOTES) nephrectomy compared with conventional laparoscopic surgery in a porcine survival model.
Methods:
Fifteen female pigs (32.8–37.2 kg) were randomly assigned to undergo TV NOTES (n=5), TR NOTES (n=5), or conventional laparoscopic nephrectomy (n=5). Postoperatively, all animals were observed for global health status during the recovery from anesthesia. Variable laboratory parameters and inflammatory cytokines were compared among the groups during the entire experimental period. Postmortem examination was performed 1 week after operation for assessment of abdominal complications and cultures for microorganisms.
Results:
All experiments were completed successfully without insertion of an extra port or conversion to laparoscopic or open surgery. Although mean operative times were longer in TV and TR NOTES groups than in the conventional laparoscopy group (61 vs 84 vs 24 min, P<0.001), there were no signs of visceral injury or peritonitis on postmortem examination. None of the laboratory parameters, including white blood cell count, tumor necrosis factor-α, interleukin (IL)-1, and IL-6 differed among the groups during the entire experimental period.
Conclusions:
TV and TR NOTES nephrectomy could be completed successfully with similar physiologic influence to those of conventional laparoscopic nephrectomy in a porcine survival model.
Introduction
B
Natural orifice translumenal endoscopic surgery (NOTES) is a technological breakthrough of minimally invasive surgery that may have advantages over conventional laparoscopic surgery because it eliminates the abdominal incisions. 5 Although NOTES may have enormous potential, there are many problems that need to be clarified before this approach is introduced into clinical practice. The most significant concern is the physiologic influence of NOTES, which could be considered an important measure for the invasiveness of a new surgical approach. Another concern regarding NOTES is intraperitoneal complications, because the laparoscopy comes in through the gastrointestinal tract or vagina, which is more contaminated than the skin.
To our knowledge, however, few in vivo data evaluating the physiologic influence or safety of urologic NOTES are currently available. 6,7 To clarify this, we analyzed the technical feasibility, physiological influence, and safety of transvaginal (TV) and transrectal (TR) NOTES nephrectomy compared with conventional laparoscopic surgery in a porcine survival model.
Methods
Preoperative preparation of animals
This experiment was approved by the Institutional Animal Care and Use Committee at Seoul National University Hospital Biomedical Research Institute (IACUC No. 11-0284). A total of 15 female pigs (30–35 kg) were randomly assigned to undergo TV NOTES (n=5), TR NOTES (n=5), or conventional laparoscopic nephrectomy (n=5). All animals were fasted for 24 hours, and water was withheld for 8 hours before surgery. After sedation with intramuscular Zoletil and xylazine at a dose of 5 mg/kg, the animals were given general anesthesia and the level of anesthesia and cardiopulmonary status was blind monitored by veterinary technicians unaware of the research question. All animals were given intramuscular cefazolin (TV NOTES or conventional laparoscopy group) or cefazolin+metronidazole (TR NOTES group) antibiotics at the beginning of the operation after irrigation of the vagina (TV NOTES group) and rectum (TR NOTES group) by water enemas until the drainage was clear.
Operative procedures
(1) Conventional laparoscopic nephrectomy
Conventional laparoscopic nephrectomy was performed with the animals in the flank position. After CO2 insufflation up to 14 mm Hg, two 12-mm (Ethicon Endosurgery, Cincinnati, OH) and one 5-mm trocars were placed. Peritoneum was dissected over the kidney. The renal artery, vein, and ureter were dissected, clamped with titanium clips (Covidien, Norwalk, CT), and then divided. Finally, the kidney was placed inside a laparoscopic bag and removed through the camera port. Skin incisions were closed with 3-0 polyglactin sutures.
(2) TV NOTES nephrectomy
The animal was placed in the flank position, and then the Trendelenburg position with an inclination of 30 degrees. The lower limbs remained in a parallel, opened position for easier TV access. A 2-cm incision of the anterior vaginal wall, 1 cm proximal to the opening of the urethra, was made using a resectoscope (Karl Storz, Tuttlingen, Germany, Fig. 1). By using this approach, the bladder and rectum are spared from injuries, allowing safe port placement.
Anterior vaginal incision using the resectoscope.
After the placement of Quadriport (Olympus, Orangeburg, NY) through that incision (Fig. 2), a 5-mm flexible laparoscope (EndoEye™; Olympus) was inserted through the most dependent channel. After thorough abdominal inspection, nephrectomy was performed in the same manner with conventional laparoscopic surgery using roticulating laparoscopic instruments (Covidien) to create the required angle. After the surgery, the kidney was removed using a vaginal incision, and the incision was not closed.
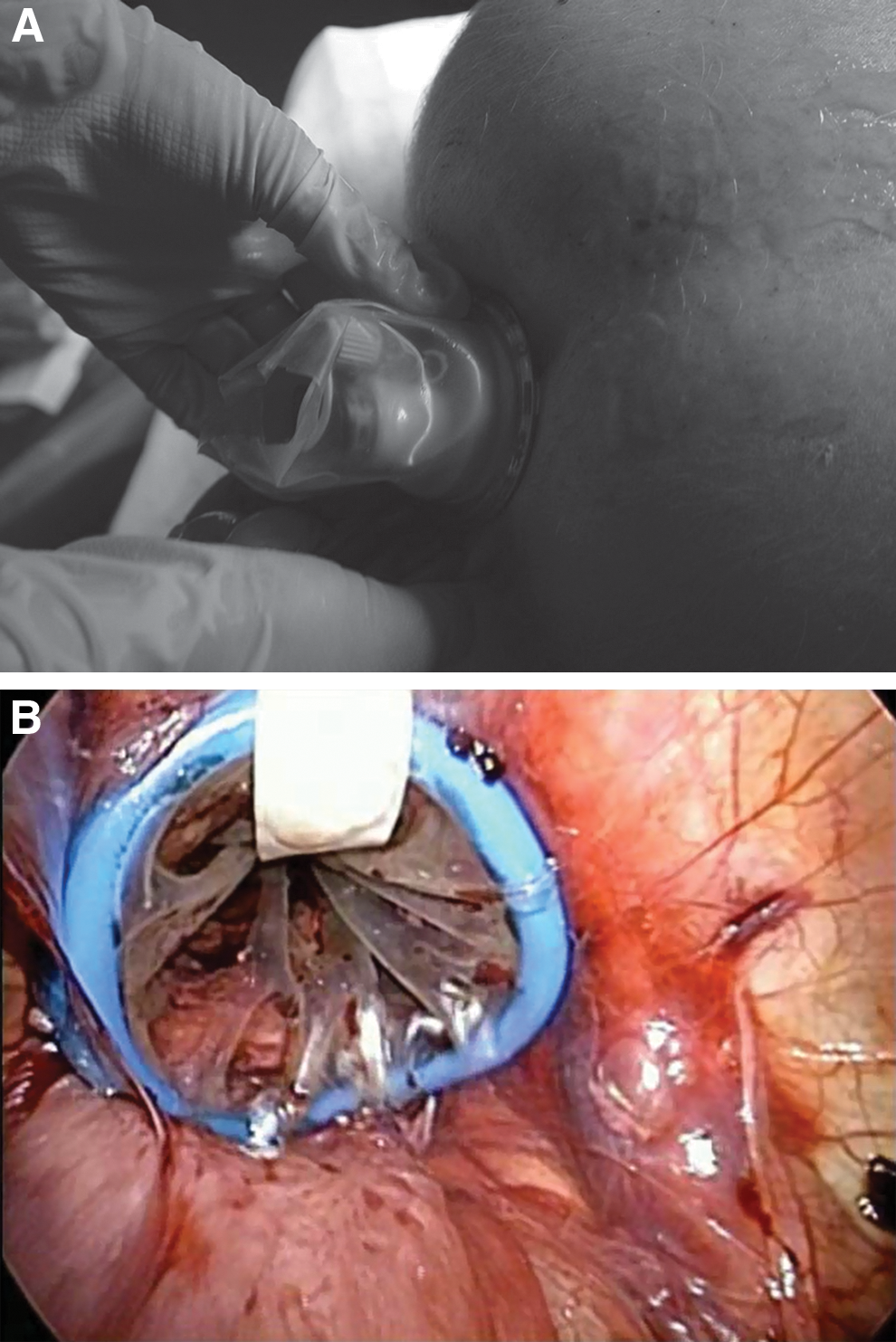
Placement of Quadriport through the vaginal incision: (
(3) TR NOTES nephrectomy
Regarding TR NOTES nephrectomy, the animal was placed in the same position as that for the TV NOTES nephrectomy. After a vigorous water enema, a purse string suture was applied approximately 10 cm upward from the anal verge to prevent bowel insufflations and fecal contamination. A 2-cm mucosal incision through the anterior aspect of the rectal wall was made below 2 cm from the purse string suture using a cold knife. After dissecting the submucosal layer more proximally and making an incision in the seromuscular layer at the distal end of the submucosal tunnel, a Quadriport was inserted into the peritoneal cavity. After the nephrectomy using the roticulating laparoscopic instrument (Fig. 3), the kidney was delivered transanally, and the incision was closed with 3-0 polyglactin absorbable sutures and the purse string suture was removed.

Schematic cross-sectional image of the pelvis. TV=transvaginal; TR=transrectal.
Postoperative care and data collection
All experimental animals survived for 1 week, during which time behavior, oral intake, and body temperature were monitored every day. Blood samples for cytokines including tumor necrosis factor (TNF)-α, interleukin (IL)-1β and IL-6, and white blood cell (WBC) counts were performed as follows; immediately before the surgery and 0, 1, 3, 5, and 7 days after surgery. Concentration of TNF-α, IL-1β, and IL-6 were determined using the multiplex bead immunoassay system, Procarta® Cytokine Assay Kit (Affymetrix, Inc., Santa Clara, CA) according to the manufacturer's guidance. Data acquisition was completed using a Luminex-compatible Bio-Plex workstation and its software version 6.0 (Bio-Rad, Tokyo, Japan) according to the manufacturer's guidance.
Postmortem examination was performed 1 week after the surgical procedure for assessment of abdominal complications and cultures for microorganisms. The peritoneal cavity was examined for any signs of visceral injury or peritonitis and intraperitoneal fluid cultures for microorganisms were performed.
Statistical analysis
Statistical analysis was completed using IBM Statistical Package for the Social Sciences (SPSS) software, version 19.0 (SPSS Inc., an IBM Company, Chicago, IL). We compared perioperative parameters, including operative time and complications, as well as all laboratory and immunologic parameters among these groups. Differences in outcomes were analyzed by Mann–Whitney U test for continuous variables and chi-square test for categorical variables. Data were considered statistically significant at P<0.05.
Results
The mean weight of the animals was 35.2 kg (range 32.8∼37.2 kg) with no differences among the groups. All experiments were completed successfully without insertion of an extra port or conversion to laparoscopic or open operation as planned initially. Mean operative time was significantly longer for TV and TR NOTES nephrectomy than for conventional laparoscopic nephrectomy (61.2±32.3 vs 84.7±37.1 vs 24.0±5.4 min, P<0.001). There was one intraoperative complication during the procedure. In one case in the TV NOTES group, bleeding occurred because of incomplete vein ligation. It was possible to control the bleeding, however, by grasping the bleeding point with a roticulating grasper and reclamping it with titanium clips.
All animals had unremarkable recoveries and thrived without adverse consequences until they were euthanized 7 days after surgery. None of the animals demonstrated clinical signs of infection (fever, tachypnea, lethargy, changes in bowel habit, etc.) during the observational period. There were no differences among the groups for any of the hematologic parameters measured at days 0, 1, 3, 5, and 7 (Table 1). Also, baseline and postoperative serum TNF-α, IL-1β, and IL-6 levels demonstrated no significant variations among the groups (Fig. 4). All the hematologic parameters and inflammatory cytokines at day 7 had returned to levels similar to those measured preoperatively in all groups.
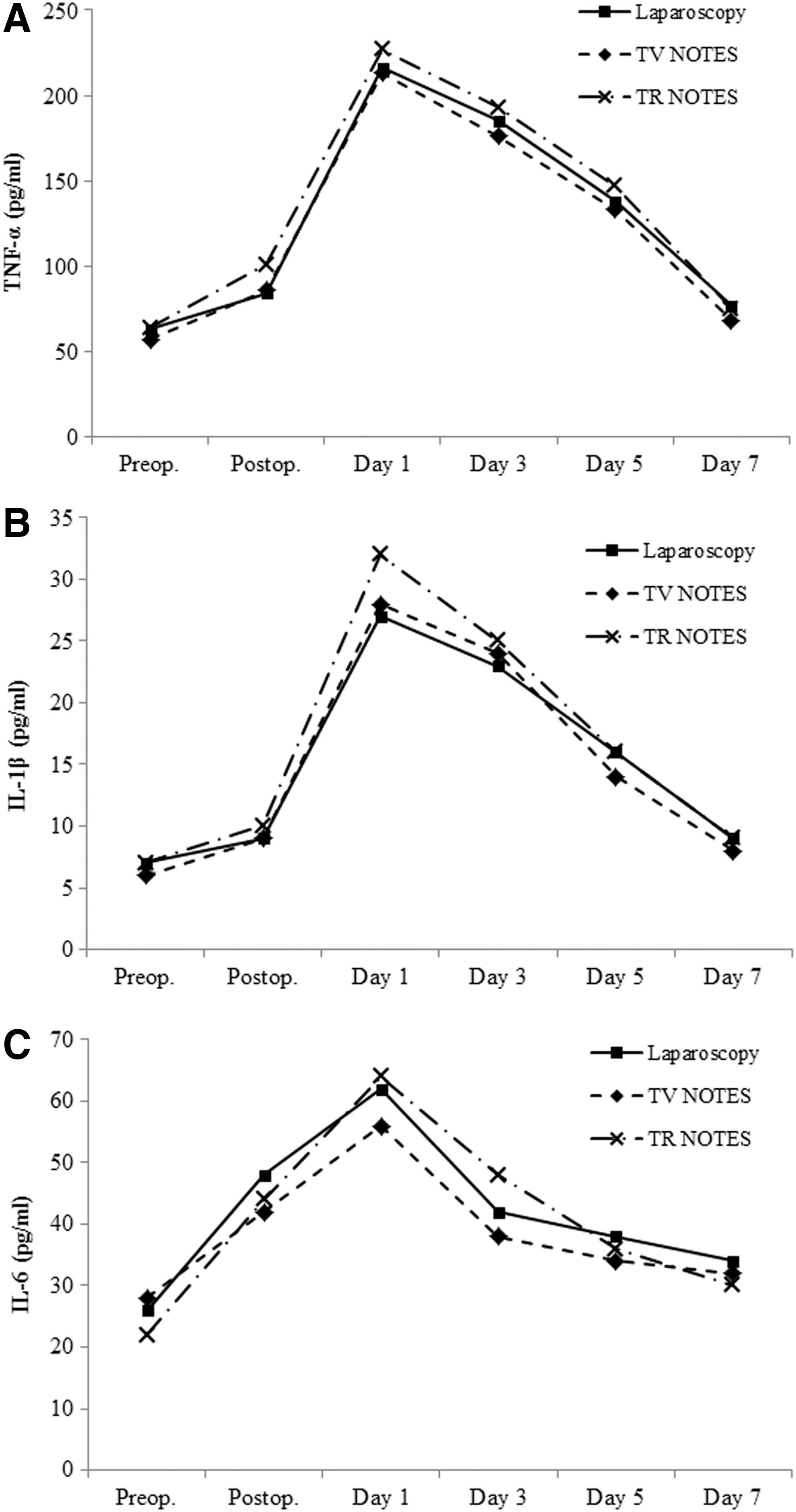
Changes in inflammatory cytokines among the experimental groups: (
All P values are statistically insignificant (p>0.05).
Hs-CRP=high sensitivity–C-reactive protein; TV=transvaginal; NOTES=natural orifice translumenal endoscopic surgery; TR=transrectal.
Autopsy confirmed complete healing of TV and TR NOTES incision sites in all animals. There were no signs of visceral injury, bleeding, or peritonitis. None of the animals in the conventional laparoscopy and TV NOTES group showed bacterial growth in the abdominal cavity, whereas one of the animals from the TR NOTES group had positive cultures. The microbes found in the peritoneal fluid were mainly Escherichia coli and Staphylococcus aureus.
Discussion
Since it was first reported in 2004, 5 NOTES continues to be developed and reported, offering the promise of a truly scarless surgical procedure. There are potential obstacles to clinical practice of NOTES, however, including the need for adequate access to the peritoneal cavity, the need for safe closure of the incision site, infection prevention, the need to keep spatial orientation, the need for a stable platform and appropriate instruments, and prevention of physiologic untoward events. 8 Despite the existing body of research for laparoscopic surgical procedures, which has led to the understanding and reduction of physiologic untoward events associated with pneumoperitoneum, the extent to which these findings can be extrapolated into NOTES remains unclear.
Our experimental study clearly demonstrated that TV and TR NOTES nephrectomy can be performed safely without significant inflammatory response in a porcine survival model. Inflammatory cytokines, WBC count, and serum high sensitivity–C-reactive protein levels did not differ among the TV NOTES, TR NOTES, and conventional laparoscopy groups. There is still some debate, however, concerning previous results. Trunzo and associates 9 measured TNF-α, IL-1β, and IL-6 concentrations locally in the peritoneal fluid after transgastric NOTES and conventional laparoscopy and reported significantly higher levels of TNF-α and IL-6 in the NOTES group than in the conventional laparoscopy group when using CO2 to create the pneumoperitoneum.
In addition, Guo and colleagues 10 reported that transgastric NOTES in rats was associated with a worse physiologic outcome in terms of peritoneal inflammation assessed by peritoneal IL-1β, IL-6, and IL-10. In a more recent study, however, by Guarner-Argente and coworkers, 11 baseline and postoperative serum TNF-α levels demonstrated no significant variation among the NOTES and conventional laparoscopy group. These results are consistent with those of several previous studies. 12 –14
These contradictory results from previous studies may be because of the differences in peritoneal access, peritoneal insufflation, and types of surgery. To our knowledge, most of the previous studies have been submitted to journals within general surgical fields focused on peritoneoscopy, cholecystectomy, and so on. 15 We think that the current study has benefit over previous studies because this is the first report evaluating the safety and physiologic influence of the urologic NOTES procedure.
In the current study, TV and TR NOTES nephrectomy did not increase the risk of intraperitoneal infections. In microbial cultures performed from the peritoneal fluid, one animal of the TR NOTES group had bacterial growth of E. coli and S. aureus without clinically relevant infections, which might be considered contamination from the rectal and skin flora of the experimental animal. These findings are consistent with those of previous studies. 16,17 Azadani and colleagues 17 evaluated the risk of intraperitoneal bacterial contamination after open, laparoscopic, and transgastric NOTES procedures. At the start of the surgical procedure, four animals in the transgastric NOTES group showed positive cultures, but at the end of the procedure, only one animal showed positive cultures without clinical signs of peritonitis. They concluded that clinically significant infections are uncommon after transgastric NOTES procedures in spite of the evidence of bacterial contamination.
Although care was taken to minimize biases, the potential limitations of our study should be mentioned. First, we did not calculate sample size based on precise statistical analysis. The number of experimental animals in our study was limited, and the results could be statistically underrepresented. We believe, however, that it is also important to balance the number of animals between the minimum number of animals to limit potential suffering and enough number of animals to avoid repetitions of experiments. Second, questions might be raised concerning the use of a porcine model to study bacterial contamination in TV and TR NOTES groups. Despite possible differences in the normal flora between humans and pigs, 18 we believe that clinically relevant conclusions can be drawn by this comparative study.
Finally, total operative times differed among the groups, which might influence the inflammatory response. Modified inflammatory response was clearly observed in laparoscopic procedures with long operative times with CO2 pneumoperitoneum and extensive traumatic tissue manipulations. 19 Differences in operative times in each procedure, however, are beyond our control. 20,21 Further studies in humans should therefore be performed to confirm these results.
Conclusion
Although technically demanding and necessitating longer operative time, TV and TR NOTES nephrectomy could be completed safely with comparable physiologic influence to conventional laparoscopic nephrectomy in a porcine survival model.
Footnotes
Acknowledgments
This research was supported by the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education, Science and Technology (2010-0008492).
This research was selected as the recipient of the WCE 2012 Best Laparoscopy/Robotic Paper.
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.