
Abstract
Background and Purpose:
Indications for laparoscopic renal surgery are increasing; however, benefits in adult polycystic kidney disease (APKD) remain uncertain. Our objective was to systematically synthesize the reported literature on safety, feasibility, complications, and early outcomes of laparoscopic nephrectomy in APKD to determine clinical benefits for surgical practice.
Methods:
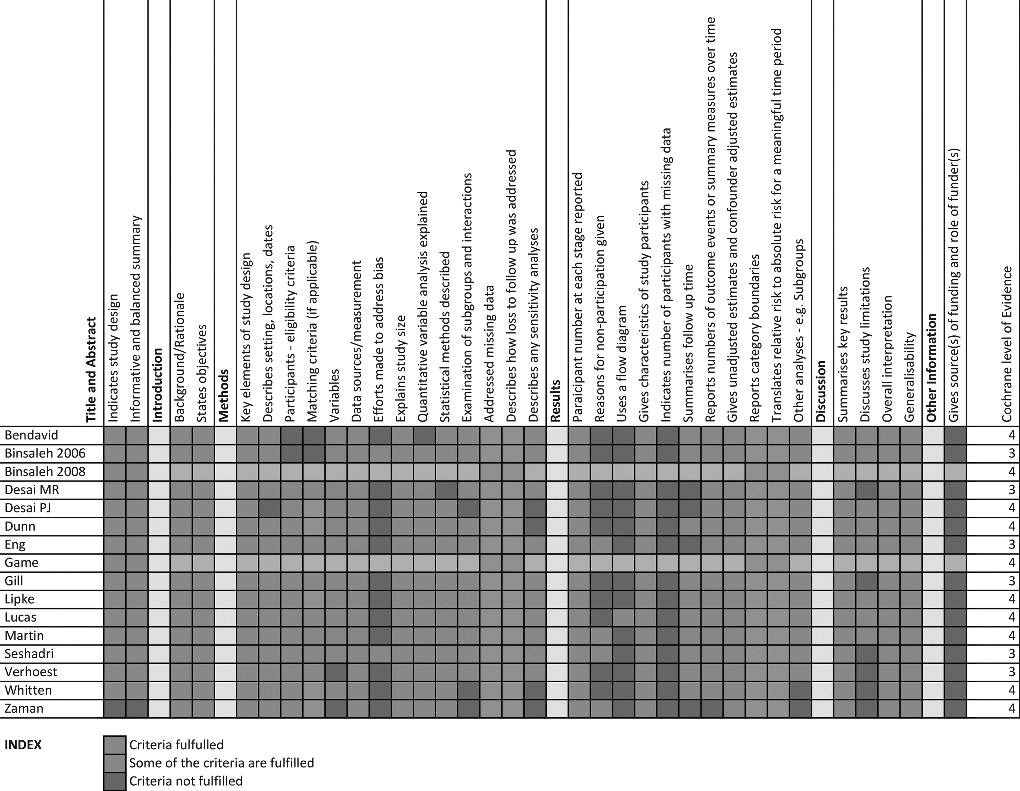
We conducted a meta-analysis of the published literature reporting on laparoscopic nephrectomy in APKD between 1991 and 2013. The criteria from the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) study were used to assess the quality of reported literature.
Results:
One prospective and 15 retrospective studies of low to modest quality (according to the STROBE checklist) were identified, reporting on 293 patients who underwent laparoscopic nephrectomy for APKD. None of the studies was a randomized clinical trial (RCT). The transperitoneal approach was the most commonly used technique. Body mass index ranged from 16 to 57 (mean 26.2 kg/m2; 53% of patients were dialysis dependent, and 31% had a previous or simultaneous transplant. Kidney length ranged from 8 to 50 cm (mean 34.5cm), and the mean mass of affected kidneys was 1647 g (range 132 g–7200 g). Duration of hospital stay ranged from 2.6 to 11 days (mean 4.9 days). Operative time ranged from 90 to 568 minutes, with 16.2% of patients needing blood transfusion. There were 24 intraoperative complications and 68 postoperative complications, a rate of 8% and 24%, respectively. A total of 16 (5%) cases were converted to an open technique. No mortality was reported in any of the included studies.
Conclusion:
The quality of the included studies is poor, and it is difficult to argue for or against change in clinical practice because the evidence included is of level 3 and 4 only. Higher quality studies are needed to demonstrate that the technique is generalizable across all populations.
Introduction
L
Adult polycystic kidney disease (APKD) or autosomal dominant polycystic kidney disease is estimated to affect between 1 in 400 and 1 in 1000 in all populations. 9 It frequently leads to end-stage kidney failure necessitating dialysis, and nephrectomy may be indicated for a variety of reasons including the requirement for space for transplant, intractable pain, recurrent urinary tract infections, and other reasons, which arise because of the grossly enlarged kidneys that may develop in APKD.
The challenges of laparoscopic surgical resection in polycystic kidney disease are real, particularly for grossly enlarged kidneys, and not many centers offer this technique as a procedure of choice. Higher risk of conversion to open procedure; risk of damage to neighboring organs; risk of bleeding because of coagulopathy; uncertain anatomic landmarks to rely on; and doubtfulness about its real benefits to patients are some of the factors that have caused delay in the adoption of laparoscopic resection of polycystic kidneys since it was first described in 1996. 10 There are, however, many observational studies reported in the literature demonstrating the feasibility and safety of this procedure in selected patients, when performed by experienced surgeons. 6,11
Because of significantly better perioperative outcomes reported for laparoscopic renal resection for kidney diseases, 12 it has been hypothesized that the laparoscopic approach for polycystic kidney resection may offer similar benefits to patients in their recovery to normal activities. The impact of this approach on the outcomes, however, is uncertain. Initial studies 10,13 investigating the safety, feasibility, and early results are small and inconclusive, but the evidence has not previously been appraised systematically.
The objective of the present meta-analysis was to synthesize results from observational studies reporting on laparoscopic polycystic kidney resections and to assess: 1. Technique, safety, and feasibility of the procedure, taking into account blood loss, operative time, length of stay, and rate of complications. 2. Perioperative and early outcomes of the various clinical end points.
Methods
Search strategy and study selection
We searched PubMed, Scopus, and Embase for observational studies investigating the results of the laparoscopic approach for polycystic kidney disease resection. We used free text and the Medical Subject Headings terms “laparoscopy,” “kidney,” “polycystic kidney disease,” “nephrectomy,” “laparoscopic nephrectomy,” “minimally invasive surgery,” “laparoscopic kidney resection,” “renal failure,” and “mortality due to nephrectomy.” The search period was January 1991 through September week 4, 2013; no language restrictions were added. We also searched the Cochrane Central Register of Controlled Trials and reviewed the reference lists of relevant original articless and review articles. The search was limited to studies after the first successful report of laparoscopic nephrectomy in 1991. 14
We aimed to identify all observational studies that evaluated the outcomes of laparoscopic polycystic kidney resection (Table 1). Our exclusion criteria were the following: (1) Not original research (reviews, editorials, nonresearch letters); (2) studies not conducted in humans; (3) case reports and studies considering fewer than six cases in total. Studies considering laparoscopic nephrectomy performed in a combined operation with renal transplant were included.
HAL=hand–assisted laparoscopy.
Three investigators (SP/GN/AW) independently reviewed search results and selected articles to determine eligibility and extract study data. They resolved discrepancies by consensus. For observational studies, the checklist from the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) article was used to assess each cohort's study quality. 15 The checklist includes the basic domains of appropriate selection of participants, appropriate measurement of outcome variables, and appropriate control of confounding. This is a scientific method of assessing design-specific biases.
Surgical techniques used within Tayside
Transperitoneal approach
The patient is placed in the lateral decubitus position, with the kidney bolster up and the table flexed. The operating surgeon stands opposite the nephrectomy. Video monitors are located at the head of the operating table on both sides. All patients received preoperative antibiotics.
Pneumoperitoneum is established, with a 12-mm laparoscopic cannula placed just lateral to the rectus muscle using an open technique. Two or three additional ports of varying size (5 to 12 mm) are placed under direct vision in the subcostal, iliac fossa, and flank, as needed. A 0-degree–viewing 10-mm laparoscope is inserted through the 12-mm port and held by an assistant. After colonic mobilization, cysts are punctured using a standard suction device to reduce volume and improve working space. This facilitates the hilar dissection and identification of structures such as the inferior vena cava and duodenum. The hilar vessels are clipped and the kidney mobilized. If there is any difficulty encountered during mobilization, cysts are punctured to ease the dissection and reduce the size of the specimen. The kidneys are either morcellated or removed as an intact specimen through a small cut in the right iliac fossa.
The extraction incision is closed, and the pneumoperitoneum re-created to inspect for hemostasis. The abdomen is deflated, and all trocar incisions are closed with absorbable sutures.
Retroperitoneal approach
In large cystic kidneys filling almost half of the abdomen (Figs. 1A, 1B), the transperitoneal approach was thought not to be feasible; hence, a retroperitoneal access was planned in these cases. In a lateral kidney position with a break in the table, ports placement is performed as shown in Figure 2. Before port placement, transabdominal ultrasonography-guided cyst aspiration is performed to make space for balloon dissection and ports entry. With three ports in place (two 12 mm and one 5 mm), hilar structures are approached with the psoas muscle as an anatomic landmark (Fig. 3A). Hilar structures are dissected and clipped (Fig. 3B). It is important to make sure that vessels are entering into the kidney before the application of any clip because superior mesenteric vessels could be close and may be mistaken in a very large kidney crossing the midline for the renal artery. Satisfactory control of the hilum should lead to mobilization of the kidney, and during mobilization, large cysts could be punctured and aspirated as the dissection proceeds (Fig. 3C).


Patient positioned in the lateral decubitus position for the surgical procedure, with port holes highlighted.

Mobilized kidneys could be morcellated or removed as an intact specimen through the enlarged middle port. The extraction incision and other port sites are closed after ensuring hemostasis. In cases in which bilateral nephrectomy is to be performed, patients were placed with the opposite side on the top and the procedure repeated using the same steps.
Results
Meta-analysis
Characteristics of included studies
From 72 abstracts scanned, 15 retrospective case series and one prospective case control study were included (Fig. 4; Table 1). The included studies reported on 293 patients, with a total of 454 renal units extracted. There were 148 unilateral procedures and 153 bilateral procedures included. The studies were published between 2000 and 2013. All but one study 16 was performed in the United States, Canada, or France. The number of case subjects varied between 617–19 and 58. 20

Flow chart demonstrating study selection process.
The surgical procedures were accomplished via the transperitoneal approach in most cases, except for three studies that described the retroperitoneal route, 16,18,21 although Dunn and associates 21 and Desai and colleagues 16 only described using this in one and two cases, respectively. Where the mean age of patients was given, the mean value across studies was 50.8 years, and the range was 29 to 73 years. The body mass index of patients (where given) ranged from 16 to 57, and the mean value was 26.2 kg/m2 (Table 2).
BMI=body mass index.
Across 14 studies where data were included, 156 (53%) patients were receiving dialysis treatment at the time of the surgical procedure and 90 (31%) patients had a previous or simultaneous transplant.
The size of the kidney (preoperative, before any cyst decortication) was reported in the results of 10 studies, and where given ranged from 8 to 50 cm with a mean size of 34.5 cm (across the studies where a mean value was given).
The mean duration of hospital stay ranged from 2.6 to 11 days, with a mean across the studies including the mean duration for their cohort of 4.9 days.
All studies found the laparoscopic approach to be safe and feasible.
Laparoscopic approaches
The majority of kidney extirpations were performed using the transperitoneal approach—either complete laparoscopy or hand-assisted. Some of the reports mentioned retroperitoneoscopy. 11,16,18,21 Most of the studies confirm the safety and feasibility of total transperitoneal and transperitoneal hand-assisted laparoscopy approach.
Intraoperative and postoperative complications
Based on the included studies, operative time ranged from 90 to 568 minutes, including both unilateral and bilateral procedures. The shortest unilateral procedure lasted 90 minutes, and the longest unilateral procedure, 528 minutes. The shortest bilateral procedure lasted 99 minutes and the longest, 568 minutes (Table 3).
Mean blood loss across all studies was 198 mL, with a range from 75 mL to 5000 mL. The mean percentage of patients needing blood transfusion was 16.2%. Procedure-related complications ranged from 0% to 67
Five studies reported conversion of procedures to an open approach because of complications occurring during the surgery such as aspiration of adjacent cysts; dense adhesions between the transverse mesocolon, kidney and spleen; inferior vena cava tear; and large kidney size.
The mass of affected kidneys ranged between 132 g and 7200 g with a mean of 1647 g. There were two renal unit removal techniques described in the studies; some of the authors utilized cyst puncture and extraction of the resected kidney through a midline or Pfannenstiel incision; others suggested placing the kidney in a bag and morcellating the specimen before extraction. It was acknowledged that morcellation hampers the ability to investigate the extracted renal unit within histopathology and could potentially pose a risk of renal tumor seeding.
Postoperative complications of laparoscopic nephrectomy most commonly included arteriovenous fistula thrombosis, 18,20,21 –23 incisional hernia, 20,24 prolonged bowel ileus, 11,25 and retroperitoneal hematoma. 11 In addition, it was noted by Eng and coworkers 20 that there was an increase in hand-port site hernia development where the hand-assisted approach was used.
Ten of 16 studies included a statistical test.
Quality assessment of the included studies
Table 5 summarizes the quality of the studies. Methodologic quality was broadly acceptable, with a high risk of bias in reporting, performance, and selection of participants. Most of the studies were conducted in major high-volume laparoscopic centers and hence generalizability of findings remains a major challenge. Precision of estimates of events such as complications is variable because of a large variation in the sample sizes of the included studies. Any expansion in the indications of a complex procedure such as laparoscopy should be based on clear and consistent standards of reporting, which was lacking in the present study. Participants varied in their baseline characteristics within and across all the studies included in the review, and hence a large selection bias exists.
Discussion
In the present meta-analysis, we identified that the laparoscopic approach in the resection of kidneys affected by APKD is a procedure that involves many risks. A complication rate as high as 67% 6 and higher conversion rate compared with laparoscopic radical nephrectomy offered in routine practice should be kept in mind while counseling patients. The validity of these findings, however, is uncertain, because observational retrospective studies have been unreliable in determining the outcomes and are associated with various biases. There were no RCTs or well-conducted prospective studies assessing the outcomes of laparoscopic resection of polycystic kidney disease. Overall, the evidence does not at present demonstrate an overall benefit of the laparoscopic approach compared with open in polycystic kidney disease resection.
Safety and outcomes of the procedure
Laparoscopic surgical excision of the polycystic kidney is associated with unique challenges. The size of kidneys, distortion of anatomy, and risk of bleeding from coagulopathy are some of the factors responsible for the delayed adoption of the laparoscopic approach for this condition. A higher conversion rate and the challenging range of intraoperative injuries reported in this meta-analysis reflect the complexity of the surgical procedure. Decreased postoperative pain with lower analgesia requirement, and shorter hospital stay (in the meta-analysis, the median length of stay after laparoscopic kidney resection was 4.9 days) observed during the reported observational studies are the driving factors for offering this procedure to patients.
Several intraoperative complications occurred, including inferior vena cava tear, a splenic tear, serosal duodenal tear, caval injury during the aspiration of the cysts, intraoperative arteriovenous dialysis, fistula thrombosis, adhesions of cysts to surrounding tissue and organs, and perforation of the gallbladder. Conversion to open surgery occurred mostly because of intraoperative complications, but in four patients, conversion occurred because the size of the kidney was too large to extract laparoscopically. 25 One procedure was converted to an open approach because of hemorrhage from ruptured cysts. 24 The most common reason for conversion was adhesions. 20,24,25 This did not subsequently affect outcomes but led to longer hospital stay.
Blood loss did not seem to be affected by patient age, body mass index, or kidney size. Many patients within this cohort had end-stage renal failure and were receiving dialysis at the time of surgery, increasing the likelihood of bleeding and tissue damage. Patients may also be awaiting or have undergone previous renal transplant. Consequently, blood transfusion is to be avoided if at all possible, with the risk it carries of immune sensitization and increased possibility of subsequent transplant rejection.
The included studies offered different opinions on the debulking of polycystic kidneys intraoperatively—from our observation of results, there did not appear to be any correlation between cyst rupture and a negative postoperative outcome. In addition, there was no correlation between kidney morcellation or removal of intact specimen and negative clinical outcome.
The spectrum of injuries is a reminder that the laparoscopic approach in this condition should not be taken for granted in centers with limited or no experience. A careful and prudent decision by the surgical team to elect for open conversion should be part of the surgical plan.
Retroperitoneoscopic approach
Some surgeons may use the retroperitoneoscopic technique with preport placement ultrasonography-guided cyst aspiration when dealing with very enlarged polycystic kidneys that fill almost half of the abdomen. The use of transabdominal ultrasonography-guided cyst aspiration before port placement makes space in the retroperitoneal area for port entry and balloon dissection. With psoas as a landmark, the hilar structures are dissected and the kidney is mobilized. Extraction occurs either after morcellation or through an enlarged middle port. The technique did not take significantly more time than many of the studies included in our meta-analysis, including the hand-assisted transperitoneal laparoscopic technique. No retroperitoneal case needed conversion to an open procedure or blood transfusion; there were no major complications. We therefore propose that while performing laparoscopic nephrectomy for very enlarged polycystic kidneys, a retroperitoneal approach should be used, in the hands of experienced surgeons.
Limitations of this meta-analysis
The meta-analysis of current research studies is limited because of the small number of patients included in the studies, meaning that many do not achieve significant results or have been able to conduct a statistical test. Our meta-analysis is also limited by the fact that the majority of included data are retrospective, and only one of the included studies was based on prospective data collection.
The ability to draw significant conclusions is hampered by the lack of any RCTs comparing different approaches to polycystic kidneys, and the lack of experience of the operative technique demonstrated in several of the included studies (particularly as many are single surgeon studies) in which the operative time decreased with more experience of using the technique. Single surgeon studies may also imply that the technique could be difficult to reproduce.
The included studies were generally retrospective with high selection bias. The reporting was generally of modest quality with several articless not specifying follow-up, as can be seen in Table 5. All but one study presented internal comparisons between study participants, and data were collected in a similar manner for all studies, generally including relevant patient demographics, operative time, and complications. Study quality was generally poor, but the lack of statistical tests is important to note when considering the evidence for different operative techniques in this setting.
Future research and clinical implications
Laparoscopic surgery has established itself as a surgical approach-of-choice in many conditions mainly because of significantly better perioperative outcomes and minimal access-related trauma compared with open surgery, confirmed by the larger cohort studies in our meta-analysis. 11,20,26,27 The expanding indications of this approach now include areas in which even open surgery would have been difficult, if not impossible. Laparoscopic resection of polycystic kidneys is an example. The often forgotten question in the introduction of expanding new surgical approaches remains: “Are new approaches better than the established ones?” The data from our systematic synthesis of the literature described above are aimed at answering the same question. Innovative surgical techniques may offer the promise of improved patient care and appear to be attractive, intuitive, and magnetic to healthcare professionals. A widely held perception that scientific routes of assessing new surgical procedures such as RCTs are unethical needs to be challenged. The most common design used by surgeons in reporting new procedures is retrospective case series (single reporter; single center) as confirmed by us in the case of laparoscopic nephrectomy in APKD. This design lacks hypotheses, planned collection of data, independent assessment, and is prone to biases. All of these factors contribute to the poor quality of the reported literature.
Furthermore, we adopted the STROBE checklist as a tool for assessing the quality of published observational research in laparoscopic resection of polycystic kidneys.
28
This approach may not be seen as prescriptive as this sounds to be; it addresses issues such as confounding, bias, and external validity of findings in a transparent way and may improve the methodology of studies in the long term. Improved reporting may help to have better informed decisions and better adoption (or otherwise) of new technology in the future. Any future reporting in the area of expanding indications in laparoscopic surgery should include: 1. Scientific background, specific objectives, and prespecified hypotheses. 2. Study design, methods of participant selection and data collection, and a follow-up protocol—including ways of ensuring all complications are included using validated methodology. 3. Methods of data analyses, sample size calculation, reporting of confounding factors and biases. 4. Discussion of key findings including the implications, limitations, and generalizability of the procedure/technology.
Conclusion
Based on systematic synthesis of the reported literature in the present study, poor quality (level 3 or 4) evidence hampers the ability to draw useful conclusions for or against change in clinical practice. Further research is needed, preferably a RCT or at least in the form of a well-conducted case control series or in center(s) experienced in the laparoscopic approach, before the technique can be shown to be generalizable across all populations.
Footnotes
Acknowledgment
This work was sponsored by Urology Research Funds at the University of Dundee.
Disclosure Statement
No competing financial interests exist.