
Abstract
Background:
Monitoring of urinary pH is an important part of the assessment of patients with urinary tract stones. It provides valuable information about the future stone risk of certain patients and further allows the effective tailoring of medical intervention. Accurate measurement is therefore essential in these patients.
Objective:
The purpose of this study was to determine the most accurate method of measuring urinary pH in an outpatient setting.
Materials, Methods, and Participants:
Urine samples were collected from 200 patients attending stone clinics at The University Hospital of South Manchester. pH was measured by three commonly used methods: Siemens Clinitek Status pH meter, a hand-held pH meter, and litmus paper read visually. Results were compared with readings simultaneously obtained from a bench-top laboratory pH machine, which is the reference method for pH measurement.
Statistical Analysis:
The pH readings obtained were analyzed using the Bland-Altman plot.
Results and Limitations:
When compared with the reference method, the hand-held pH meter differed the least with a mean bias of 0.0073 and a maximum under-read of −0.2 pH units and maximum over-read of +0.2 pH units. The Siemens Clinitek pH meter differed most with a mean bias of −0.108, with a maximum over-read of +0.99 pH units and a maximum under-read of 0.78 pH units. The pH values obtained with the litmus paper gave similar results to that of the Clinitek pH meter with a mean bias of −0.069, with a maximum over-read of 0.96 and maximum under-read of 0.82 pH units.
Conclusion:
The hand-held pH device gave urinary pH readings that most closely and consistently matched those of the reference bench-top laboratory machine. This method of pH measurement should be considered in stone clinics in patients with pH-dependent stone risk.
Introduction
K
Materials and Methods
Sampling strategy
Urine samples for pH analysis were collected over a period of 6 months from a total of 200 patients attending stone clinics at University Hospital South Manchester. Samples were taken from both male and female patients and also from individuals who had a metabolic diagnosis, such as cystinuria or diabetes, giving as wide a variety of patients as possible within the study group.
Urinary sample collection
Urine samples were collected immediately after voiding and analyzed via the three urinary pH testing methods under investigation: Clinitek pH meter (Siemens), litmus paper (Simply Health), and hand-held pH meter (Hanna Instruments). All readings obtained were compared with readings with the reference laboratory pH meter (Corning Lifesciences), which was calibrated using freshly prepared standard pH solutions. Readings were taken by an HPC-registered health care professional in a CPA-accredited pathology laboratory.
Urinary pH testing
Clinitek pH meter (Siemens)
Urine dipsticks (supplied by manufacturer) were dipped into the urine specimen provided, immediately after voiding in accordance with the manufacturer's instructions. It was then read on the manufacturer-calibrated machine and the result was printed.
Hand-held pH meter (Hanna Instruments)
The pH meter was calibrated with pH solutions of pH 3, 7, and 10; after which, the probe was placed into the urine sample. The pH reading was digitally read and recorded.
Litmus paper
A strip of litmus paper was placed into the urine pot and the color change was recorded, by comparison with the manufacturer's color chart corresponding to relevant pH values. The reader was tested beforehand for color blindness with an appropriate group of charts. The color change on the pH strip was compared with the color chart corresponding to relevant pH values.
Laboratory pH meter
The pH meter was calibrated prior to use with pH solutions of pH 3, 7, and 10. The pH probe was placed in the urine sample and a pH reading was recorded for all samples tested with the previous methods.
Statistical analysis
The pH measurements recorded were documented on a spread sheet in Excel before being analyzed statistically on SPSS. The Bland-Altman plot was used to establish the differences in accuracy the methods used for the testing of urinary pH. The results of the comparison between the three methods when compared with the reference method are summarized in Tables 1 and 2.
Results
Siemens Clinitek pH meter
The Siemens Clinitek pH meter showed a mean bias of 0.108 pH units. The Clinitek pH meter gave a maximum over-read of 0.99 and maximum under-read of 0.78 pH units when compared with the reference pH meter. One hundred twenty (60%) patients showed an under-read and 66 (33%) patients showed an over-read in pH readings (Fig. 1).
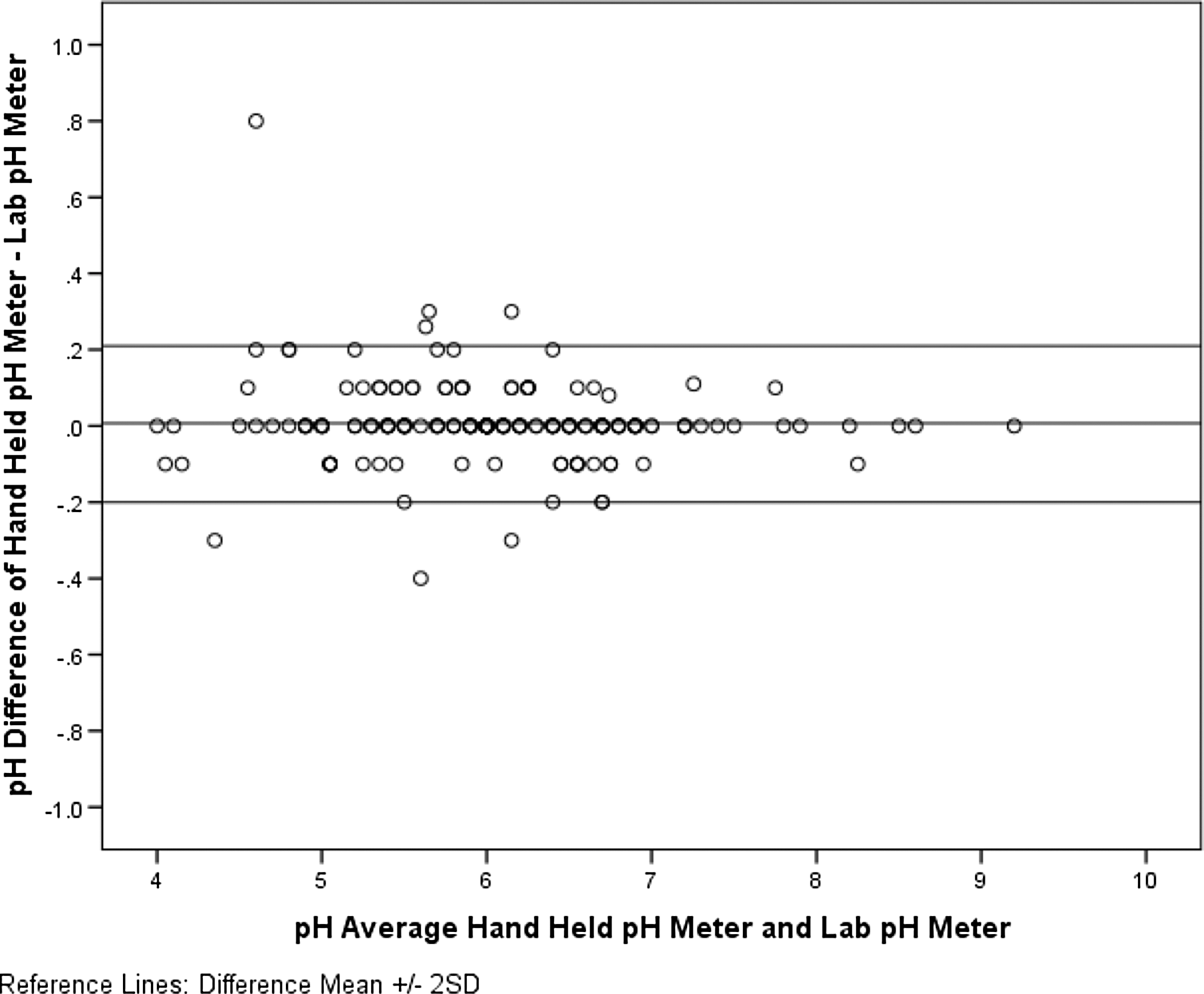
Bland-Altman plot showing agreement between hand-held pH meter and the bench-top reference pH meter (laboratory).
Litmus paper
pH readings obtained with litmus paper showed a mean bias of 0.069. There was a maximum under-read of 0.82 and maximum over-read of 0.96 pH units, compared with the reference (Fig. 2). One hundred three (51%) patients showed an under-read in urinary pH and 73 (36%) showed an over-read.
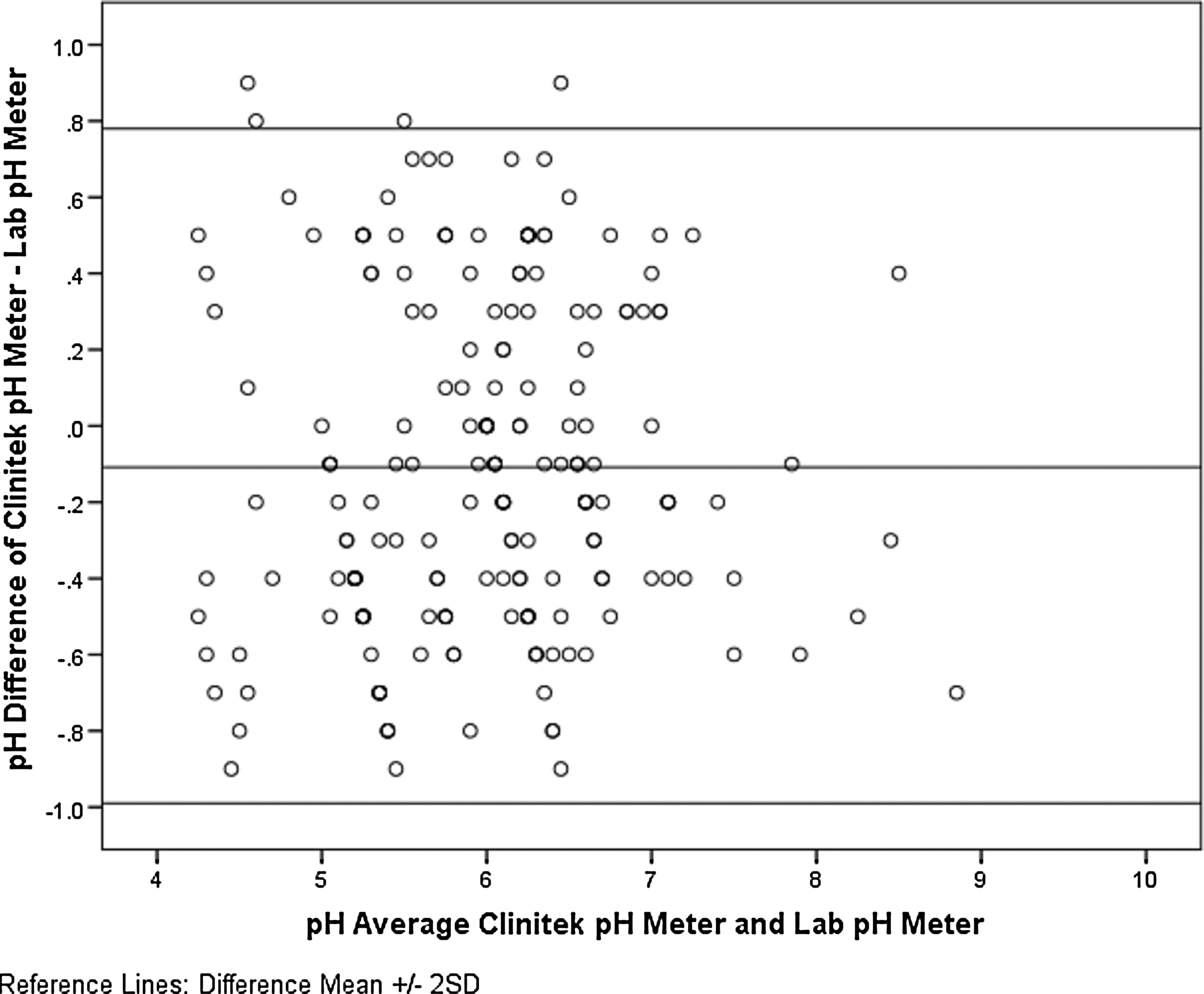
Bland-Altman plot showing agreement between Clinitek pH meter and the bench-top reference pH meter (laboratory).
Hand-held pH meter (Hanna Instruments)
The hand-held pH meter showed a mean bias of 0.0073. There was a maximum under-read of 0.2 and maximum over-read of 0.2 pH units, compared with the reference. The hand-held pH meter showed no consistent over- or underestimation of pH compared with the reference method. One hundred thirty-four (67%) patients showed no difference in pH reading (Fig. 3).
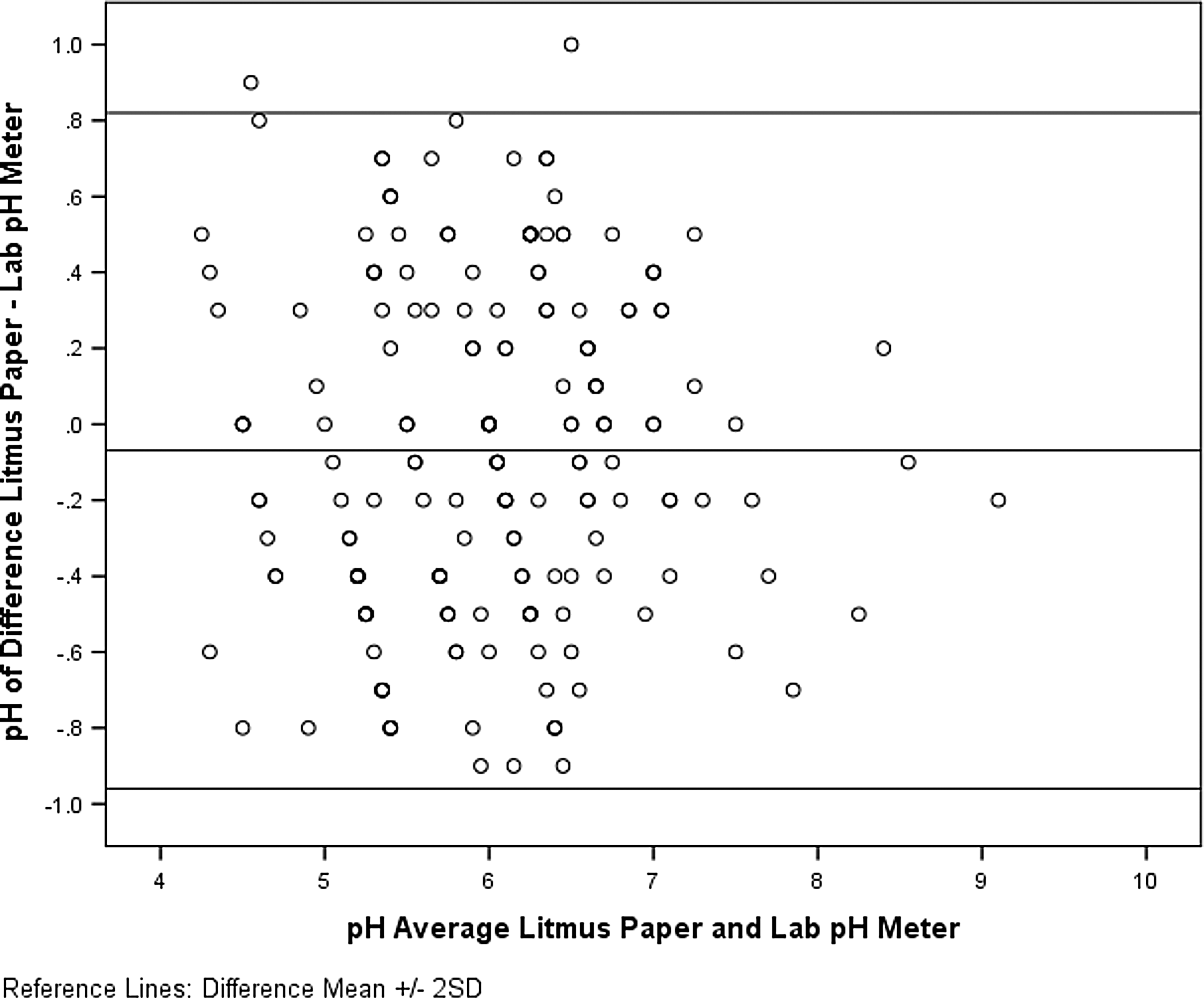
Bland-Altman plot showing agreement between litmus paper and the bench-top reference pH meter (laboratory).
Discussion
Analysis of urinary pH in the management of renal calculi is an important clinical parameter in recurrent stone formers. This study was carried out in order to establish the most accurate method for urinary pH analysis in an outpatient setting. Previously, we have relied on machine-read Siemens Clinitek as the main method of pH measurement, with litmus papers also utilized for patients to take home to record a pH diary if diurnal variation in pH was thought to be likely or significant. The use of a small, portable hand-held pH meter was suggested by the University Hospital South Manchester (UHSM) Department of Clinical Biochemistry since these meters have become more widely available and lower in price. The hand-held pH meter had not been previously tested for its clinical reliability when measuring urinary pH.
The accuracy of our current methods used to measure urinary pH was therefore tested and compared with the hand-held meter and a bench-top machine. The Siemens Clinitek showed considerable inaccuracy when measuring urinary pH, generally giving an over-read of up to 0.99 pH units. This may constitute a significant difference when managing urinary pH, for example, in deciding to change dosing of oral potassium citrate. The Clinitek machine under-read the urinary pH by up to 0.99 pH units. Perhaps more concerning was the inconsistency seen in the spread of values demonstrated on the Bland-Altman plot in Figure 1.
It is unclear why these inaccuracies may arise. The Clinitek reading machine is calibrated in accordance with the manufacturer's instructions, although this is only once per year. Attempting to measure several parameters (leucocytes, red blood cells, etc.) at once may interfere with the values of the colorimeter as only one light-detector channel is used to measure all parameters (Manufacturers insert; Siemens). Litmus paper gave an underestimate of up to 0.82 pH units, but more commonly also over-read the urinary pH by up to 0.96 pH units, similarly to the Siemens Clinitek method. Litmus paper is also effectively a colorimetric assay, which moreover relies on a subjective visual comparison of the color change compared with a standard chart. Nevertheless its accuracy and spread of values was very similar to the Clinitek. Similar results regarding the inaccuracy of dipstick measurement of pH have been noted in both animal (veterinary) and human studies; Johnson et al. 3 performed a study on dog urine noting significant inaccuracy of dipsticks and superiority of a hand-held meter. Measurements were then made with four different portable hand-held pH meters and compared with a bench-top pH meter as a reference method. This study universally showed superiority of hand-held meters over the colorimetric assays more commonly used clinically.
Kwong et al. 4 similarly demonstrated inaccuracy and the general under-reading of urinary pH, which they speculated may lead to overtreatment in those patients where controlling urinary alkalinization is imperative.
Limitations of this study include the testing of only one brand of urine dipstick (Siemens Clinitek). There is evidence that different brands of dipstick may have varying performance and optimum pH ranges for accuracy. 5
Cost is also clearly an increasingly important factor in healthcare. Material costs are fairly consistent between countries and regions but staffing/time costs are likely to be more variable. We have found that with adequate training, nursing staff are able to perform any of these methods of testing. We made an estimate of costs for 1000 tests, which we considered the minimum likely number of patient episodes annually in a stone clinic. In our setting, litmus papers proved the cheapest, costing approximately £49 for 1000 strips. Urine multistix cost around £350 for 1000. To this it must also be added the capital cost of the machine over its lifetime (approximately £770). The hand-held pH meter is relatively cheaper to run, costing approximately £36 for the pH meter itself and £45 for buffer sachets that should be sufficient for daily calibration for 1 year. Therefore, as well as giving more accurate better results, the hand-held pH meter appears to be a cost-effective method to implement.
In terms of the clinical applicability of the study, it must also be borne in mind that urinary pH can vary during the day, depending on dietary intake among other factors. Some studies have suggested variance between spot and 24-hour home readings, 6 while others have found insignificant variation. 7 Therefore, clinical decisions regarding urinary alkalinization may require either repeat spot testing or patient-recorded 24-hour pH diaries, which realistically can only be recorded with litmus paper.
The results of this study have led to a change of clinical practice at UHSM. A hand-held pH meter is now used by a trained technician in clinic to analyze urine from “pH-critical” patients with metabolic conditions predisposing to stone formation. For example, individuals with an underlying medical condition such as type 2 diabetes mellitus accompanied by poor glycemic control 8 with recurrent uric acid stones. Similarly, urinary alkalinization is commonly used to try to achieve an increase in solubility of cystine. We have a number of cystinuric patients who manage their disease with high fluid intake and alkalinization, either preferring to avoid the toxicity of thiols used to bind cystine, such as tiopronin and penicillamine, or having experienced adverse effects from these medications. These patients aim for a pH over 7.5, but below 8, to avoid phosphate stone formation. Clearly, the closer they can get to a pH of 8, the greater the solubility of cystine in their urine and the lower their risk of stone formation (urinary cystine is solubilized by 50% at pH 7.5 and a further 1000 mL/L at pH 8). 9 There is therefore a fairly narrow therapeutic window that requires reliable and accurate pH measurement. 10,11 For these reasons we would now recommend the use of a hand-held pH meter in such patients.
Footnotes
Acknowledgment
The authors wish to thank the statistics department at the University Hospital of South Manchester.
Disclosure Statement
No competing financial interests exist.