
Abstract
Purpose:
Permanent and prolonged incontinence following robot assisted radical prostatectomy (RARP) is known to result from injury to the external sphincter. We hypothesize that pre-existing detrusor overactivity may also contribute to delayed return of continence (>3 months). This pilot study examines the safety profile and efficacy of muscarinic receptor antagonist, solifenacin, in incontinent men after prostatectomy.
Materials and Methods:
Men using three or more pads 7 days post catheter removal were invited to enroll into the study (5 mg daily of solifenacin for 3 months). All subjects received RARP under hypothermic conditions by one surgeon. Continence was defined as 0 pads.
Results:
Forty men were enrolled, one excluded due to missing follow-up. Two men reported nonserious adverse events: one a vaso-vagal reaction when taking solifenacin with sildenafil, and the other was dehydration and dizziness after strenuous exercise. Additionally, four withdrew due to side effects. The efficacy outcomes show improved intermittency after prostatectomy, though unclear if due to the medication. At 3 months, 21 patients (53.8%) reached the primary continence outcome of zero pads. The median time to continence in this group was 95 days.
Conclusions:
Solifenacin is well tolerated in post radical prostatectomy patients with a 15% withdrawal rate due to side effects. These results formed the basis of a large, prospectively randomized clinical trial comparing the effects of solifenacin versus placebo in a population of men incontinent after RARP.
Introduction
P
The pathophysiology of postoperative incontinence is largely due to intrinsic sphincter deficiency and may be exacerbated by detrusor instability and poor bladder compliance. 6 –8 Sphincter incompetence may allow urine to leak into the urethra causing irritation and subsequent detrusor instability. 9 –11 Our group was the first to report that irritative symptoms consistent with detrusor instability were statistically correlated with men who achieved pad-free status but with occasional dripping versus pad-free status and “never leaking.” 12 We also noted that these men with pad-free continence and occasional dripping achieved continence significantly slower than men who never leaked. We proposed that detrusor instability may play a role in prolonged incontinence and that an anticholinergic might shorten time to continence. Although urologists occasionally prescribe anticholinergic medications after RP, we could not find any publication(s) that examines the use of anticholinergics to improve time to continence. Further, there are no approved treatments to improve continence or symptoms from incontinence after radical prostatectomy prior to 1 year of prolonged incontinence.
Herein, we perform the first exploratory investigator-initiated trial to evaluate safety and efficacy of postoperative solifenacin in men at high risk for prolonged urinary incontinence in order to assess the feasibility of a large-scale, prospectively randomized clinical trial. Men were considered at “high risk” of prolonged incontinence based on pad use 1 week after removal of the catheter. 13 Several groups have shown that delayed recovery of continence is best predicted on postoperative pad use or pad weights rather than preoperative parameters. 13 –15
Methods
Study design
We performed a prospective, open-label, and nonblinded phase-1 clinical trial sequentially enrolling men after robotic prostatectomy for the treatment of prostate cancer by a single surgeon (T.A.). All subjects underwent preoperative urine analysis, sexual health inventory for men, American Urological Association (AUA) symptom score questionnaire, and urodynamics evaluation. All subjects had hypothermic cooling performed during surgery. 16 Patients had their catheter removed 1 week after surgery. On day seven after the catheter removal, the subject was queried about his pad status to determine enrollment qualification. Patients using three or more pads were offered enrollment into the study and medication was dispensed to the patient after the internal review board (IRB)–approved consent process (UCI HS No. 2011-8421).
Medication and adverse events
Solifenacin (Vesicare) is an M3 acetylecholine receptor selective anticholinergic medication used as a bladder antispasmotic. Patients were prescribed daily doses of 5 mg solifenacin as per package insert description for 3 months. Men could elect to discontinue medication if they have achieved pad-free continence. All men were off study medication for months 4 through 12 for observation. Subjects were asked to score their side effects on a self-report weekly log throughout the 3-month medication period, derived from the manufacturer's data safety information sheet. The following possible side effects were queried: (1) dry mouth, (2) constipation, (3) dry eyes, (4) blurred vision, (5) urinary retention, (6) upset stomach, (7) nausea, (8) dizziness, (9) fatigue, and (10) other. Each symptom was scored on the following scale: (0) not noticed, (1) sometimes, (2) minor—not a problem, (3) irritating but tolerable, (4) very irritating, and (5) severe, and whether the symptoms were (C) constant or (I) intermittent.
Effectiveness
Effectiveness was measured by comparing AUA and urinary quality-of-life symptom scores performed preoperatively and at 3 months. Additionally, we used a post card mailing system so that the patient would mail back to the department when continence was reached. Continence was defined as zero-pad usage. 3 If we did not receive a postcard, then regular email or telephone contact was obtained to determine when the patient reached zero-pad continence.
Statistical analysis
Our primary outcome was tolerability of the medication and to document adverse events in preparation for a clinical trial. Our secondary outcome was efficacy of solifenacin after prostatectomy in men with significant urinary incontinence after radical prostatectomy. Efficacy was defined as two outcomes that are as follows: improvement in symptom control by AUA symptom score and quality-of-life time to continence. The study used standard statistical methods, such as paired t-tests, to determine individual improvements. Kaplan–Meier curves are utilized to determine the mean and median time to continence in an intent-to-treat analysis.
Results
Adverse events
The current study enrolled 40 men undergoing robotic radical prostatectomy, of which one was excluded due to loss of contact without follow-up (total=39). Demographics of solifenacin-treated group are displayed in Table 1. Patients all maintained inclusion criteria of three or more pads per day for urinary incontinence at 7 days after catheter removal. Overall, 15% (6/39) of men stopped the study due to medication side effect or adverse event (Table 2). Two men reported adverse events and terminated solifenacin due to severe flushing and significant dehydration after strenuous exercise. Additionally, four other men stopped treatment due to study medication side effects of dizziness, dyspepsia, dry mouth, or blurred vision. Eighteen patients finished the full course of 90 days; all but two were incontinent at 3 months. The remaining 16 men stopped medication due either to achieving pad-free continence before the 90 days (15), and one stopped due to self-assessed lack of improvement. At the first month, three men reported either very irritating or severe side effects (constipation, dry mouth, and in the third subject multiple symptoms of dry mouth, constipation, and fatigue). At month 2, one additional man experienced very irritating symptoms (dry eyes), and one more at 3 months (constipation), for a total of 5 (12.5%) men over the 3-month medication period. Seven more men reported irritating but tolerable side effects. Twenty-six men (65%) reported minor to not noticed side effects (Table 3).
AUA=American Urological Association symptom score; SHIM=sexual health inventory for men (AKA IIEF-5).
GERD=gastroesophageal reflux disease.
Efficacy
At 3 months, comparison of individual paired results (Table 4) displayed as the mean difference from baseline to 3 months demonstrates improvements, weak stream (−0.8; p=0.001) and intermittency (−0.45; p=0.02). The AUA symptom score has a trend to reduced symptoms (mean reduction of 1.7; p=0.073); however, the quality-of-life question trends to be slightly worse (+0.68; p=0.09). At 3 months, 21 patients (53.8%) reached the primary continence outcome of zero pads. The median time to continence in this group was 95 days and mean of 143 days, shown in Figure 1.
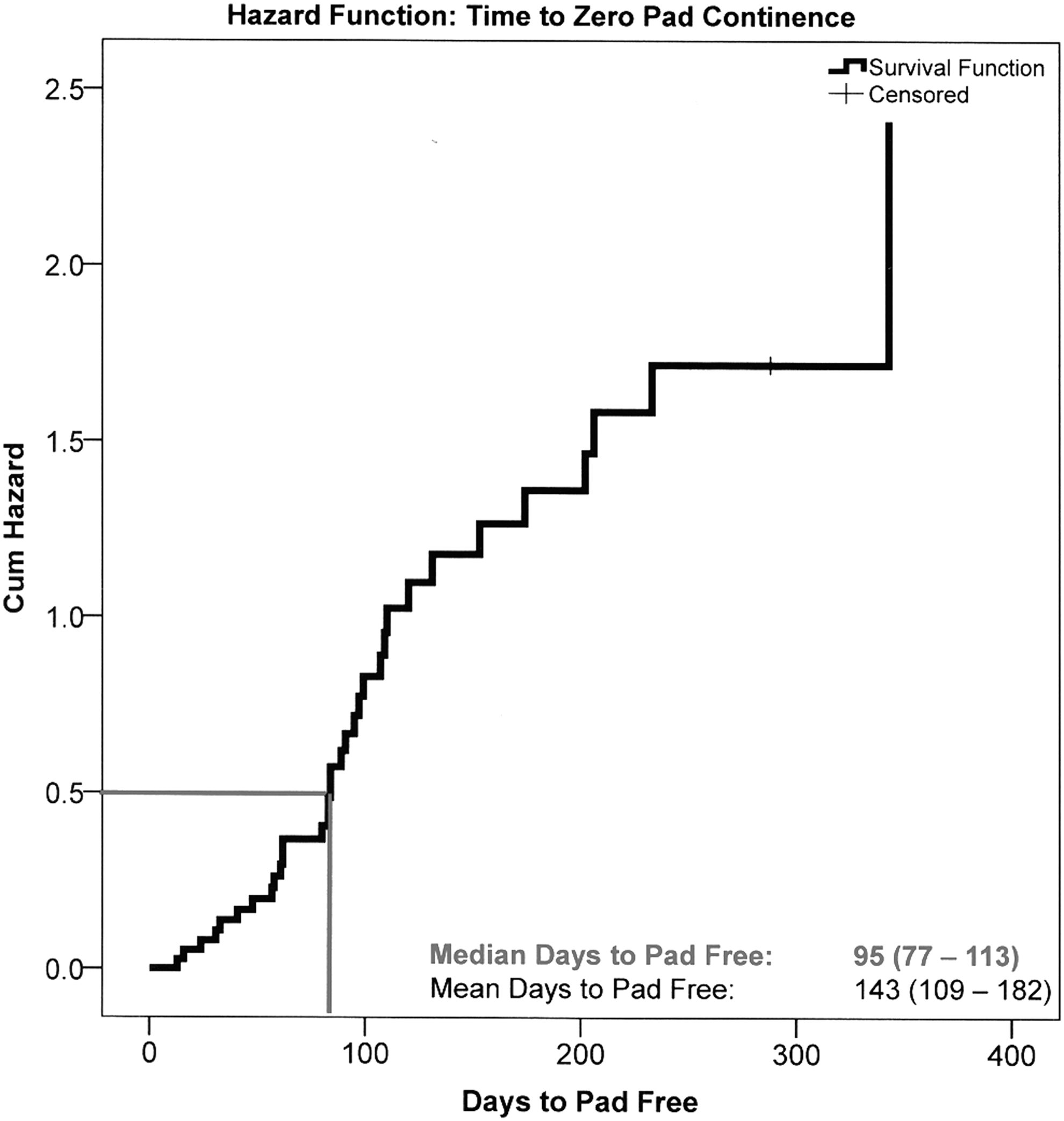
Kaplan–Meier graph of time to pad-free continence after RARP for men using three or more pads daily 1 week post catheter removal and placed on solifenacin.
Discussion
This is the first evaluation of an anticholinergic in the postoperative RP setting. Solifenacin had a discontinuation rate of 15% among men who started the medication after radical prostatectomy that had more than three-pad urinary incontinence and no deaths were reported. The discontinuation rate should be considered in the sample size calculation for an expanded clinical trial. Post card follow-up was a useful tool and reminder for patients to follow up with their urinary outcomes. Additionally, solifenacin may improve some symptom components of the AUA symptoms; only the improvement of intermittency may be related to solifenacin, though it also can be improved with a decrease in outlet resistance from radical prostatectomy.
Urinary incontinence has a major impact on patient satisfaction, quality of life, and anxiety after radical prostatectomy. 17 Unfortunately, current treatments for post radical prostatectomy incontinence are limited. Surgical treatments, such as a urethral sling, bulking agent, or artificial urinary sphincter, are usually recommended only after a year of failed behavioral therapies, such as Kegel exercises and biofeedback. 18 –20 The use of hypothermia has been suggested to reduce surgical trauma and inflammation to improve time to continence; however, results from a prospective randomized clinical trial are still in progress. 21
Conservative therapies such as early use of medication have not been thoroughly evaluated. Leach and associates studied 215 men urodynamically with postprostatectomy incontinence and found that 57% had detrusor instability as a major component of incontinence and 15% as the sole cause. 11 Other studies have indicated that patients may also develop de novo detrusor overactivity (2%–77%) and impaired bladder compliance (8%–39%). 7 –9,11 Therefore, if anticholinergics can reduce detrusor overactivity, then incontinence may be reduced. To our knowledge, the only medication previously studied involves duloxetine intended to treat stress urinary incontinence that showed increased quality of life and significant decrease in the number of incontinence episodes. 22,23 Specifically, duloxetine blocks the reuptake of noradrenalin and serotonin in the Onuf's nucleus within the sacral spinal cord causing an increase in the striated urethral sphincter tone and may relax the detrusor via the pudendal nerve. 24 These studies have small numbers and mixed population of radical prostatectomy and cystectomy patients. In addition, duloxetine may increase quality of life as it is an antidepressant possibly leading to less distress about incontinence.
We investigated solifenacin due to its selectivity at blocking the M3 receptor to inhibit contractions by detrusor smooth muscle. 25 A potential unique benefit of solifenacin among anticholinergics is that it is more selective than other antimuscarinics and has up to 15% of the medication secreted as an active metabolite into the urine and available for binding to receptors on the urothelium. 26,27 If incontinence does occur, then the active metabolite may potentially bind the urethral urothelium causing less irritation and decreasing the signals sent to the bladder causing instability. In addition, solifenacin did perform better than tolterodine ER in the European STAR trial, decreasing number of incontinence pads used, in which 14.7% were men. 28 The additional locations of M3 receptors in the intestine and salivary gland lead to the most common side effect of constipation and dry mouth (xerostomia). 25,29 Overall, the drug was well tolerated in this 3-month trial.
Weaknesses of phase-1 trial include the small sample size and lack of a control group for effectiveness comparisons. However, in phase-1 trials, the main outcome is to determine safety and identify appropriate outcomes and other calculations needed for a randomized clinical trial. Another potential limitation is the dropout rate of 15%. Further weaknesses include not performing perioperative urodynamics; however, catheters are not recommended in the postoperative period after prostatectomy. Moreover, urodynamics does not reliably identify patients with overactive bladder symptoms. 30,31 Another weakness includes only using the 5-mg dose of solifenacin. The lower dose was used in order to minimize side effects, though this medication has a flexible dosing regimen that can extend to 10 mg that was not investigated. A large randomized, placebo-controlled, validation study to formally evaluate the potential of antimuscarinics to improve time to pad-free status is required, and the current study provides data to support further investigation.
Conclusions
Solifenacin is tolerated in post radical prostatectomy patients. Of the 40 men, 6 (15%) withdrew from study medication due to side effects. Although solifenacin did not demonstrate an obvious continence benefit, there may be some symptomatic relief at 3 months. The findings have been used to develop a large prospective, randomized clinical trial.
Footnotes
Acknowledgment
This study was supported by a grant from Astellas Pharmaceuticals.
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.