
Abstract
Introduction:
Transurethral resection of bladder tumor (TURBT) and pathological staging are both standard surgical therapies for nonmuscle-invasive bladder cancer and integral parts of the diagnostic evaluation and progression monitoring of all bladder tumors. We developed and tested a dexterous robot that can fit through a standard resectoscope for evaluation for possible en bloc resection of bladder tumors, especially tumors along the dome and anterior wall of the bladder.
Materials and Methods:
Our dexterous robot uses a continuum (snake-like) mechanical architecture with three working channels through which a fiberscope, biopsy graspers, and a holmium laser were placed. The continuum robot has two segments. Using indigo carmine, injections were performed through the detrusor muscle into the mucosa of the ex vivo bovine bladders at a total of 11 positions throughout all quadrants of the bladder. The snake robot was used in conjunction with the holmium laser to ablate nine of the lesions; two additional lesions were resected en bloc using the grasper and the laser down through the muscle layer.
Results:
Both experiments showed that the robotic system was able to directly visualize all 11 targets. In both the bladders, we were able to resect en bloc two tumors using the grasper and 200 μm holmium laser fiber down to the muscle layer indicating a good resection. All of the other targets were completely ablated using the holmium laser.
Conclusion:
The dexterous robot allowed for visualization as well as provided adequate ablation and en bloc resection of bladder lesions throughout the entire bladder.
Introduction
I
Another potential drawback of the current practice of TURBT is that tumor resection is carried out in a piecemeal manner using the loop cautery rather than en bloc, resulting in potential suboptimal orientation and staging of pathology and the release of tumor cells into the irrigant fluid environment. Tumor disruption, results in viable cell release, potentially contributing to tumor recurrence due to the seeding of raw surfaces and other areas. 2 Although resection in one piece (en bloc during TURBT was recently demonstrated clinically in specific cases, 3 transurethral en bloc resection remains challenging or impossible depending on the location of the lesion. Use of various laser technologies has been explored as an alternative to standard loop resection and was found to potentially reduce the cellular seeding potential. 4 More recently, holmium laser energy has been utilized to treat NIMBC with en bloc resection, but superiority has not been demonstrated in large, randomized prospective studies. 5
In this study, we present a pilot evaluation of a novel platform robotic system for robot-assisted bladder visualization and TURBT. This system includes a dexterous two-stage continuum robot with multiple access channels that are used for visualization, instrument deployment of biopsy or retraction forceps, and energy delivery with a holmium laser fiber. The master–slave architecture allows for telemanipulation of the slave robot using a Sensable Phantom Omni haptic interface and a pedal switch for initiating manipulation. Preliminary evaluations on two ex vivo bovine bladders demonstrated the ability of the system to target all quadrants, deliver laser energy, and perform biopsies.
Materials and Methods
The proposed telesurgical system for TURBT is shown in Figure 1. The figure shows the platform robot's actuation unit, the master manipulator (Sensable Phantom Omni), a monitor showing the view from the on-board fiberscope, an inflated ex vivo bovine bladder, and an additional laparoscope for improved visualization and procedural monitoring. The robot platform uses a steerable 5 mm flexible snake-like robot with three working channels. The fundamental design of these robots was first presented 6,7 in the context of distal dexterity for endoscopic and minimally invasive surgery. The scope of this pilot study was to demonstrate the basic surgical tasks, such as endoscopic complete surface visualization and coverage, energy delivery, and resection, during TURBT.

Overview of the experimental setup.
The robotic platform was deployed inside the bovine bladder through a standard resectoscope sheath. The ex vivo bovine bladder was inflated with air (due to the lack of a water impermeable system at present) and kept at constant inflation pressure for the entire procedure. Visualization feedback was obtained from both the on-board 1.2 mm flexible fiberscope prototype, with 10,000 fibers and integrated light, and the external laparoscope inserted through the side of the bladder. The external laparoscope was a 10 mm 30° laparoscope placed in the upper left lateral wall of the ex vivo bovine bladder. The use of the secondary access port for this article was used mainly to be able to visualize the robot from the side so as to provide images showing the robot operation. Another reason for this second port was the need to keep insufflation of the bladder without having to redesign our low-cost prototype, while taking into account sealing it against liquid. The internal 1.2 mm fiberscope in this prototype was inadequate for guidance due to its low resolution. The external laparoscope met the need for adequate visualization to guide, evaluate, and record the experiment.
To model lesions involving the bladder wall, Indigo blue dye was manually injected submucosally with a 20-gauge needle and syringe to create defined target resection areas in all the quadrants at initiation of the experiment. Eleven targets were created throughout the bladder incorporating all of the quadrants, including bladder neck and trigone, left lateral wall and right lateral wall, posterior and anterior bladder wall, and the dome of the bladder. The robotic platform was then telemanipulated to fire the laser on the target area, as shown in Figure 2. A 0.55 mm holmium laser fiber was deployed through one of the access channels, and a standard holmium laser at 1 Joule and 10 Hertz energy was delivered for resections and ablations.
Laser delivery experiments. (Top) Indigo blue dye was used to delineate the resection area. (Bottom) Laser energy was delivered over the entire target area.
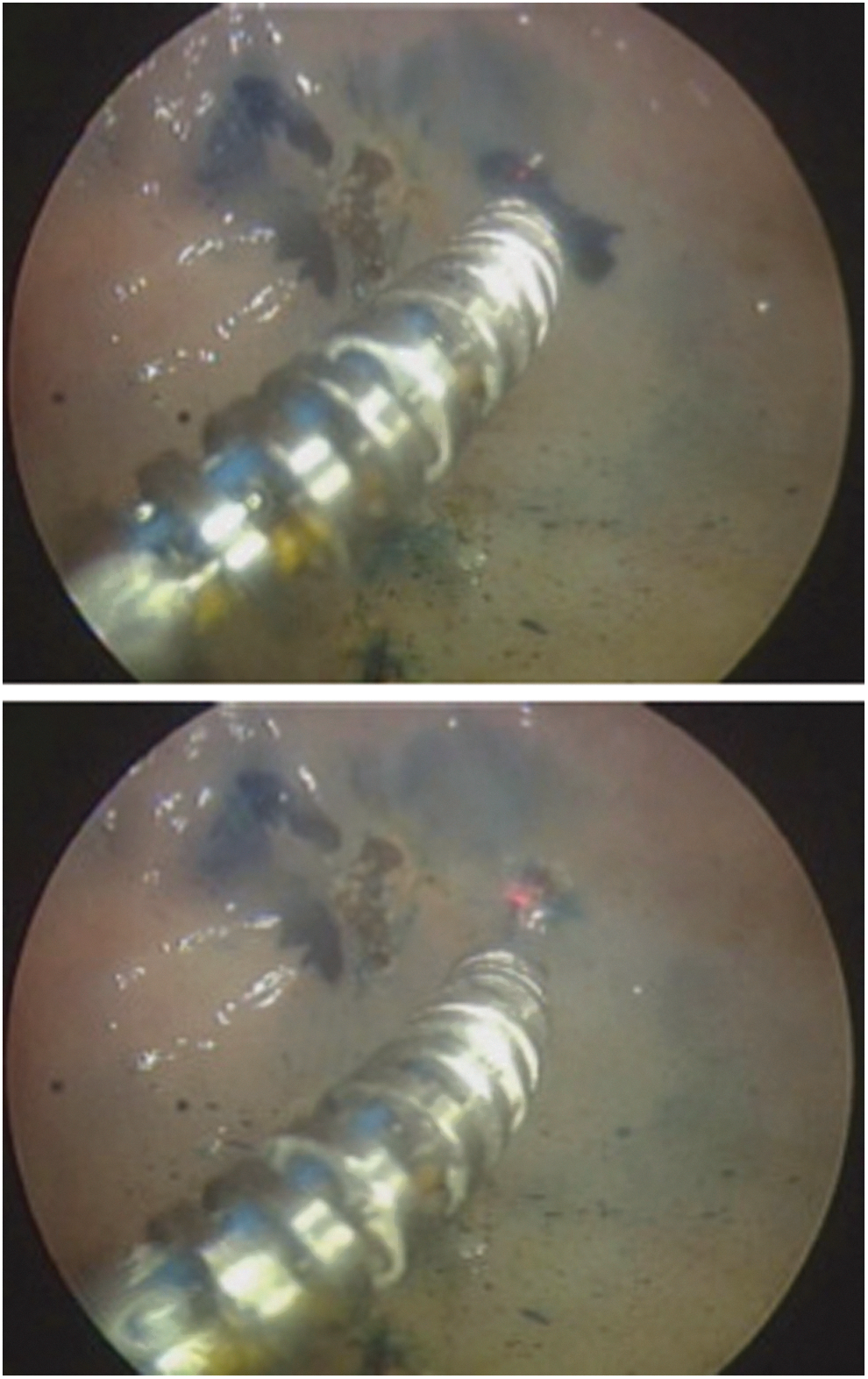
Additional experiments were performed to demonstrate the feasibility of tissue retraction potentially combined with cancer resection and biopsy. A 1.8-mm disposable biopsy forceps was delivered through the third access channel. The tissue was grasped and retracted with the grasper and laser energy was delivered to resect the sample, as shown in Figure 3. The potential of this demonstration shows that the dexterity of the slave robot end-effector allows for pivoting about the contact tissue retraction point and effectively completing en bloc resection.

(Top and Bottom) En bloc resection and extraction of a mock-up tumor.
Results and Discussions
The preliminary results demonstrated the ability of the proposed robot to complete critical surgical tasks required during TURBT. These tasks include surveillance, energy delivery, biopsy, and resection of cancerous areas.
The main limitation of the robot prototype is the on-board fiberscope. The limited cross section of the fiberscope requires a trade-off between fibers used for visualization and fibers used for illumination. Although the fiberscope was useful to examine tissue and maneuver the end-effector locally on the tissue, its short focal distance does not allow use for gross motion. We note that our current robot prototype has a diameter of 5.0 mm. We therefore do not agree that our system is more invasive, since we are able to preserve transurethral access within a 9-mm tube, while having enough space for a 3-mm Hopkins rod and two irrigation channels. The design of this specialty robot-compatible resectoscope is currently being carried out under our current NIH grant. While we are not yet to release experimental data with our new system, we believe that if the reviewer draws a 9 mm circle encompassing a 5 mm circle for the robot access channel and a 3 mm circle for a 3-mm Hopkins rod, it will be easy for the reviewer to envision our plan for this resectoscope.
Energy delivery to the all the targets in all the quadrants was effectively performed. Figure 4 shows some of the targeted area. The ex vivo bovine bladder was opened after experimental completion, and the targeted areas were examined. The energy delivery was localized to the predetermined areas only (as seen in Fig. 4).

(Top and Bottom) Close-up of the target areas after the experiments.
Tissue manipulation with biopsy and resection was also effectively demonstrated, as shown in Figure 3. The slave manipulator with multiple channels allows for the delivery of a standard 1.8-mm biopsy forceps. The biopsy forceps allows for grasping and elevating the desired tissue. By pivoting about the contact point, it is possible to resect larger areas than using the forceps for biopsy only. Figure 4 shows the slave manipulator grasping the resected tissue outside the bovine bladder. The tissue sample was pulled out along with the slave manipulator at the end of the procedure. The size of the resected tissue is larger than conventional samples that can be obtained with biopsy forceps alone. The size of the tissue is compared next to a dime of 18 mm in width, as shown in Figure 5.

(Top and Bottom) Close-up of the mock-up tumor extracted from the bovine bladder.
This robot will provide a platform that could help overcome some of the anatomical obstacles that can be seen with TURBT, such as body habitus or location of the target. New diagnostic intraoperative imaging technologies are in development that may add ability to depth of invasion staging accuracy and detect early pathological changes in tissues and organs in a field known as optical endomicroscopy, which includes optical spectrometry and optical coherence tomography. 8 These technologies can often require a stable application to a designated tissue area for extended periods of time and a robotic platform would be optimal.
Current limitations with this robotic platform are many, as this is a first-generation prototype of the platform. The system will need to be able to be sterilized for human trials. The platform will also need to incorporate waterproofing and an irrigation channel to work in fluid-filled environments, such as the bladder. Further development of an articulating channel better equipped for grasping tissue will be needed to enhance biopsy and en bloc resection capabilities. While the cost of such a system would be high, there is potential for increased safety, visualization, new optical diagnostic technology deployment, enhancement of resection of tissue, and teleoperation allowing for expert telesurgery. Additional limitations stem from the lack of independent control of the laser ablation tip to provide independent control from the grasper.
Conclusion
This pilot study of an ex vivo evaluation of a telerobotic system for transurethral intervention and surveillance was effective for both laser ablation in all quadrants of the bladder and en bloc resection of modeled bladder lesions.
Future designs will improve dexterity in the inferior quadrant by adding independent control of the robot tip, the biopsy tool, and the laser ablation probe. Additional research will focus on depth-controlled resection, enforcement of safety telemanipulation zones (virtual fixtures/active constraints), and detailed clinical evaluation of the benefits of robotic assistance for transurethral resection and surveillance. An IRB protocol has been approved for animal testing and will be carried out in the near future once we have improvements in visualization and the necessary steps for obtaining a clinically deployable system for in-vivo animal studies.
Footnotes
Disclosure Statement
No competing financial interests exist.