
Abstract
Purpose:
To determine the appropriate template of regional lymph node dissection (LND) at the time of laparoscopic nephroureterectomy (LNU) for patients with clinically node- negative urothelial carcinoma of the upper urinary tract.
Patients and Methods:
This prospective study included 45 patients undergoing LND with LNU in accordance with our prospective rules regarding the area of LND. Perioperative, pathologic, and follow-up data were collected. Micrometastasis in lymph nodes (LNs) was later evaluated by immunohistochemistry (IHC). Recurrence-free survival (RFS) was calculated with the Kaplan-Meier method.
Results:
The median number of LNs removed was 14 (range 1–33). One patient with pT3 disease had node metastasis based on routine pathologic examination, and IHC revealed micrometastases in two additional patients (pT2 in one and pT3 in one). Therefore, 15% (3/20) of patients with ≥pT2 disease had node disease. After surgery, six patients experienced minor complications (Grade 1 or 2), and Grade 5 gastrointestinal bleeding after aspiration pneumonia developed in one elderly male patient on the 45th postoperative day, which was not considered to be associated with LND. At the last follow-up, lung metastasis developed in four patients (pT1 in one, pT2 in one, and pT3 in two), and presacral lymph node metastasis developed in one patient with a lower ureteral tumor (pT2), which was not included in our prospective template for a lower ureteral tumor. LN recurrence within/ near the LND area was not observed in patients with pelvic/upper ureteral carcinoma. The 2-year nonurothelial RFS rate was 84%.
Conclusions:
We consider that the present template represents regional LNs for patients with clinically node-negative pelvic/upper ureteral carcinoma, while presacral LNs may be incorporated into the regional LND template for patients with clinically node-negative lower ureteral carcinoma.
Introduction
A
Regarding the role of lymph node dissection (LND), it remains undetermined and, especially, there are limited data regarding regional LND at the time of LNU. 2 –4 Several recent studies supported the survival benefit of LND. For example, Brausi and associates 5 and Roscigno and colleagues 6 demonstrated that cancer-specific survival rates were significantly higher in patients undergoing lymphadenectomy at the time of nephroureterectomy than in patients without LND. We also found that patients with pN0 showed significantly more favorable cancer-specific as well as recurrence-free survival (RFS) than those with pNx, suggesting that the removal of micro-disease by lymphadenectomy promotes survival in the pN0 group, and the feasibility as well as safety of LND at the time of LNU. 7 –9 These studies, however, had several limitations, including their retrospective nature and the lack of strict prospective criteria regarding the extent of LND.
In 2009, we started a prospective multi-institutional study at Hokkaido University Hospital and Hokkaido Cancer Center in which LND was performed according to the prospective rules to determine the appropriate area of LND at the time of nephroureterectomy for patients with clinically node-negative UC of the UUT. In the present article, we report the midterm outcomes.
Patients and Methods
This prospective clinical trial was approved by each participating Institutional Review Board. All patients gave written informed consent. Eligibility criteria included the presence of UC of the UUT without metastatic disease, which was an indication of open nephroureterectomy or LNU. Exclusion criteria were apparent lymphadenopathy (more than 1-cm diameter on CT) and pretreatment with neoadjuvant chemotherapy. Up to the present, 45 patients have been enrolled in this study, with all being treated with LNU at Hokkaido University Hospital or Hokkaido Cancer Center, because we actively perform LNU for patients without lymph node swelling. This study was registered in the UMIN Clinical Trials Registry (UMIN000003279).
LNU was performed using a four-port retroperitoneal approach (n=34), or a four-port transperitoneal approach (n=11) in combination with a lower abdominal incision (Gibson, Pfannenstiel, or midline incision) for specimen removal and bladder cuff resection. We previously reported the surgical technique of LND.
8
Briefly, after LNU, lymphadenectomy was laparoscopically performed in patients with a renal pelvic/upper ureteral tumor, or endopelvic LND was conducted under direct vision through a lower abdominal opening in those with a lower ureteral tumor. The template of lymphadenectomy was as follows: • For tumors of the renal pelvic or upper ureteral tumor (higher than the crossing of the common iliac artery), renal hilar, paracaval, retrocaval, and interaortocaval LNs (right side), or renal hilar and para-aortic LNs (left side) are resected laparoscopically. Regarding the vertical limits, the LNs between the area 1 to 2 cm higher than the renal hilum and the height of aortic bifurcation are dissected (Fig. 1a). • For tumors of the lower ureter, the ipsilateral obturator, common iliac, external iliac, and internal iliac LNs are resected by open surgery through a lower abdominal opening (Fig. 1b).
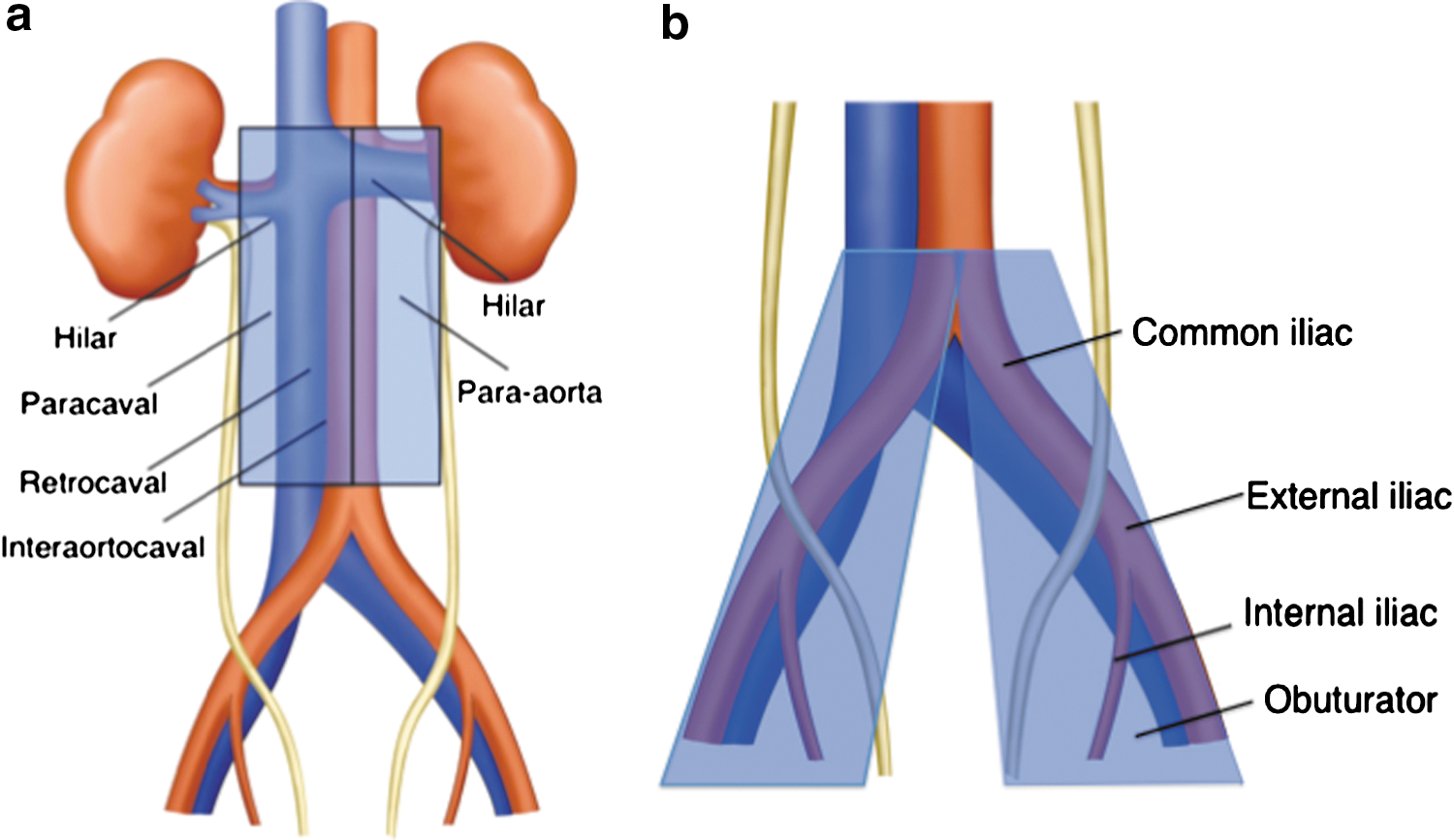
Template of lymph node dissection according to the location of the primary tumors: (
LN specimens were labeled according to their anatomic location and sent separately for pathologic evaluation.
The tumor grade was assessed according to the World Health Organization grading for urothelial carcinoma, and staging was performed according to the Tumor Node Metastasis system by different pathologists. 10,11 We subsequently evaluated the presence of micrometastases by cytokeratin immunohistochemistry (IHC) in our laboratory, as previously reported. 7 During follow-up, patients underwent chest and abdominal CT every 6 months for the first 2 years, with cystoscopy every 3 months. So far, we have not performed intravesical instillation of chemotherapeutic agents after nephroureterectomy, although two randomized studies recently showed that a single intravesical instillation of mitomycin C or pirarubicin reduced bladder recurrence after nephroureterectomy. 12,13 When UC relapse did not occur within 2 years after surgery, we extended the follow-up interval.
In the present analysis, we evaluated the perioperative as well as pathologic outcomes. Postoperative complications were categorized with modified Clavien grading. 14 The disease status at the last follow-up was also extracted and the survival curve was calculated with the Kaplan-Meier method. Statistical analysis was performed with JMP® 6.03 (SAS Institute, Japan).
Results
Table 1 shows patient characteristics. Between November 2009 and July 2013, 45 patients were enrolled in this study. The median age was 71 years (range 41–93). Twenty-one patients had disease in the renal pelvis, 22 in the ureter, and 2 in both. The median (range) operative time was 278 (150–480) min, and the median (range) blood loss was 120 (0–1317) mL. Three patients needed blood transfusion intraoperatively. The pathologic stage was pTa-is in 12, pT1 in 13, pT2 in 11, and pT3 in 9.
Table 2 summarizes LND and the pathologic node status. The median number of LNs resected was 14 (range 1–33). In the 26 patients with renal pelvic or upper ureteral tumors, a median of 13.5 nodes were resected laparoscopically. In the 17 patients with lower ureteral tumors, a median of 12 nodes were resected under direct vision. In addition, presacral LNs were removed based on surgeons' decisions in the six patients with lower ureteral tumors. On routine pathologic examination, a 68-year-old female patient with pT3 renal pelvic disease had node metastasis. Although we recommended adjuvant systemic chemotherapy, she refused it, and she was disease-free 5 months after surgery. Subsequent IHC analysis revealed micrometastases in two additional patients (pT2 in one and pT3 in one, Fig. 2) who had a diagnosis of pN0 on routine pathologic examination. They were disease-free without further therapy 15 and 17 months after surgery. Overall, 15% (3/20) of patients with ≥pT2 disease had node disease.
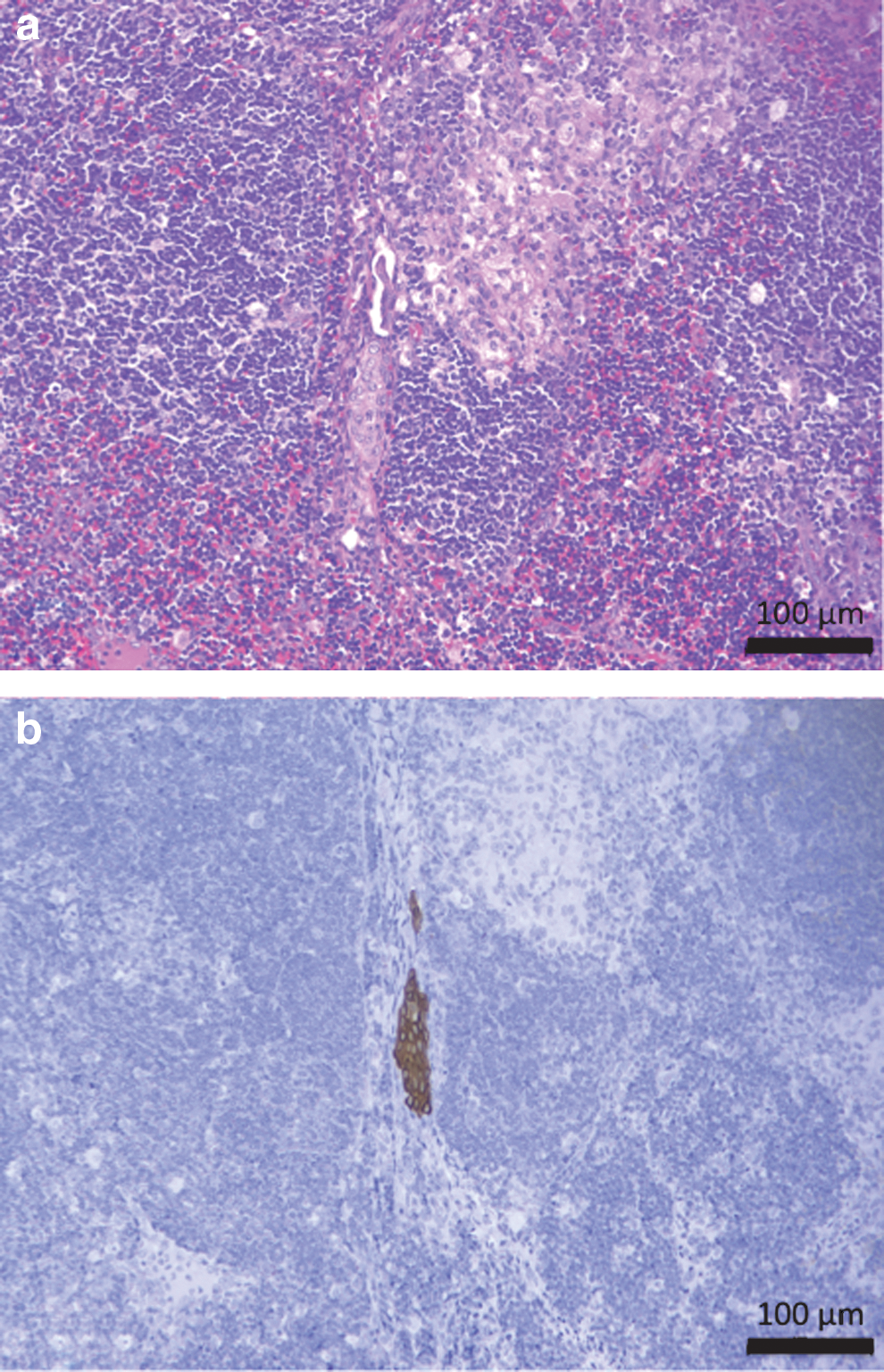
Micrometastasis in lymph node detected by immunohistochemistry: (
LN=lymph node.
Table 3 shows a summary of perioperative complications. Intraoperatively, iliac vascular injury occurred during specimen removal in one patient, and this was repaired under direct vision. The pancreas was slightly injured in another patient, but this did not necessitate an additional procedure. After the surgical procedure, nine events occurred in seven patients. Six patients experienced minor complications (Grade I or II), including chylous leakage in two patients after dietary intake, which resolved spontaneously without active intervention. Regarding major complications, Grade V gastrointestinal bleeding after aspiration pneumonia developed in a 93-year-old male patient on the 45th postoperative day.
Follow-up data were available for all patients. Intravesical recurrence developed in 18 patients at a median of 3 months (range 1–10) after LNU, and contralateral pelvic recurrence developed in 1 of the 18 patients at 17 months after LNU. Regarding nonurothelial disease recurrence, lung recurrence developed in four patients (pT1 in one, pT2 in one, and pT3 in two) at a median of 3 months (range 1–10). Regarding locoregional disease relapse, LN recurrence was detected in the right presacral area in one patient who was treated for a right lower ureteral tumor (pT2 disease) 11 months after LNU. Figure 3 shows the nonurothelial RFS curve. The 2-year RFS rate was 84%.
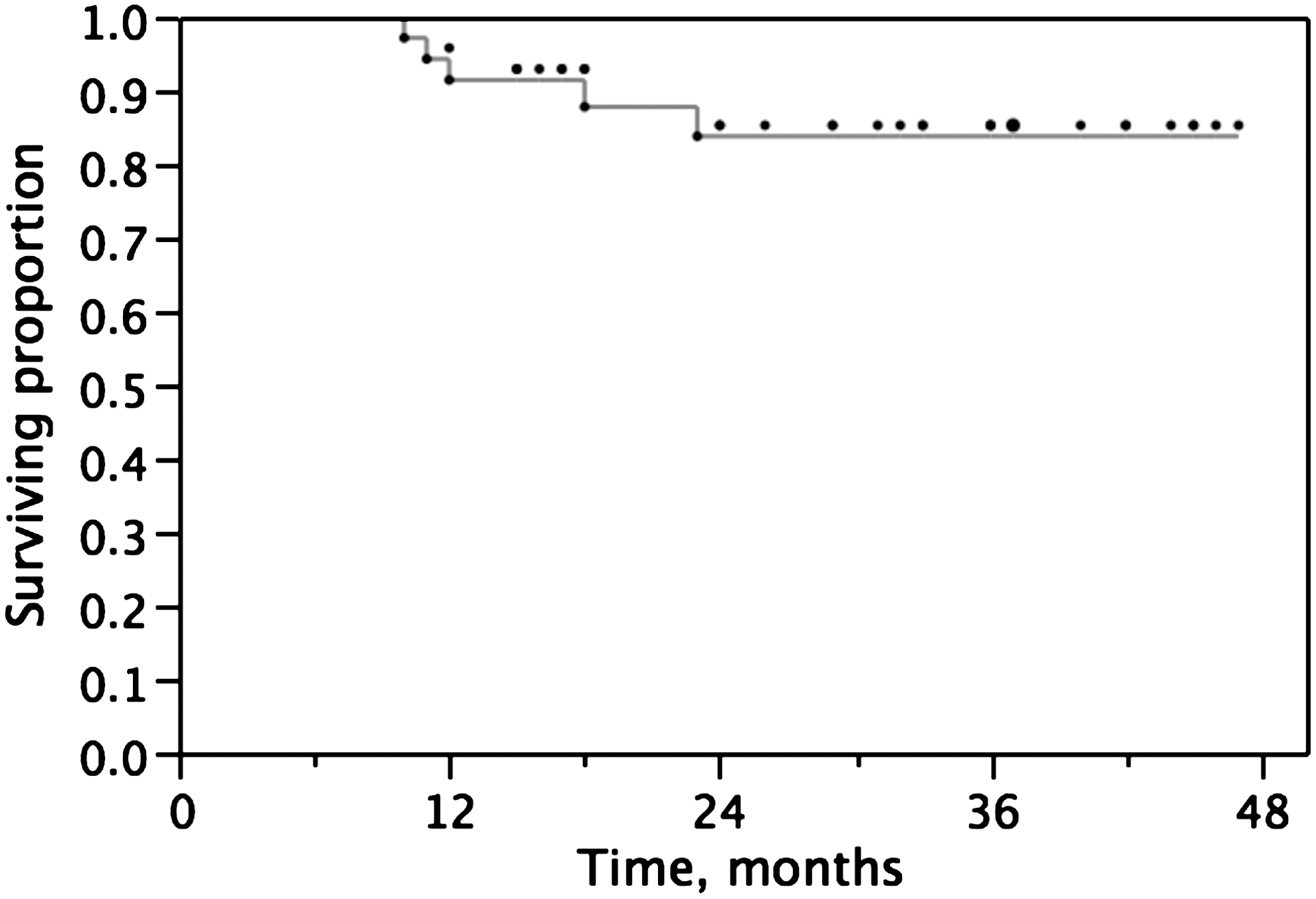
Kaplan-Meier analysis of nonurothelial recurrence-free survival.
Discussion
Based on our previous findings as well as other retrospective studies, 5 –9,15 we started this prospective study to determine the appropriate template of LND in accordance with the primary tumor location at nephroureterectomy. Because our group actively performed LNU in patients without LN swelling, the present analysis represents the feasibility and midterm survival outcome after LND in conjunction with LNU for UC of the UUT. In patients with apparent node swelling disease, we usually initially perform systemic chemotherapy and, thereafter, nephroureterectomy plus lymphadenectomy via an open or a laparoscopic approach if systemic chemotherapy is considered effective.
With regard to the number of LNs, a median of 14 was removed in this cohort, which was more than in our previous observation (median, 10; range 2–59). 8 Regarding other retrospective reports, Klingler and coworkers 2 stated that lymphadenectomy was performed in nearly three quarters (14/19) of a LNU group and the mean node count was 8.7 (range 5–11). Busby and colleagues 3 reported a median of six nodes dissected in a LNU group, 3 while Hattori and associates 4 reported a mean of 11.6 nodes for a LNU group. Rao and coworkers, 16 in their prospective study, reported that the mean node count was seven (range 2–17) in patients undergoing regional lymphadenectomy in conjunction with open nephroureterectomy (n=10), LNU (n=4), or robot-assisted nephroureterectomy (n=6).
Our observation of a median of 14 nodes is the highest node count among the reported studies, which means that the prospective rule of the LND template and so-called Hawthorne effect, a phenomenon whereby persons will improve or modify their behavior simply because they are being observed, would increase the node count. Very recently, Kondo and Tanabe, 17 based on their open nephroureterectomy cohort, in which regional lymphadenectomy was prospectively performed under very similar rules as ours, reported that a mean of 13 nodes were removed in patients with a renal pelvic or upper urinary tract tumor. In the present cohort, a median of 13.5 nodes were retrieved by laparoscopic procedures in patients with a renal pelvic or upper ureteral carcinoma, which supported the feasibility of laparoscopic LND in conjunction with LNU. Regarding the duration of LND, it usually added 0.5 to 1 hour, although it was not recorded separately from the total operative time.
The results of international multi-institutional studies have supported the positive role of lymphadenectomy in UC of the UUT, 15 as has been proposed in radical cystectomy in terms of accurate staging and improving the oncologic outcomes by eliminating micrometastases. In the present study, a 68-year-old female patient with pT3 renal pelvic disease had node metastasis. Using an immunohistochemical technique, we detected micrometastases in two additional patients with a diagnosis of pN0 disease on routine pathologic examination (pT2 in one and pT3 in one, Fig. 2), and, therefore, in the present cohort, 15% (3/20) of patients with ≥pT2 disease had node disease.
Because the LN status is one of the powerful prognostic factors and preoperative node staging has limited accuracy to detect LN metastasis, we consider that, at present, LND is necessary for accurate node staging in the treatment of UC of the UUT. In addition, the two patients with micrometastases were disease free without adjuvant treatment at 15 and 17 months after surgery. As described above, at the last follow-up, lung metastasis had developed in four patients, and locoregional LN relapse had developed in only one patient with a lower ureteral tumor. Previously, in a retrospective multi-institutional study (total n=293, pN0/pNx/pN+=130/141/22), we observed that regional LN recurrence (n=34) was more common than that at distant sites (n=28) and pNx (omitting LND) was a risk factor for both types of recurrence. 7 Although the observations in this study suggest improved local disease control by LND, we could not reach a definitive conclusion because we did not have a control cohort.
In the present study, postoperative complications developed in seven patients. Although six patients experienced minor complications (Grade I or II), Grade 5 gastrointestinal bleeding after aspiration pneumonia developed in a 93-year-old male patient on the 45th postoperative day. Although it was an unfortunate complication, we consider that this event was incidental, not directly associated with LND, and that his advanced age compromised his recovery after aspiration pneumonia. Chylous drain discharge was observed in two patients after starting a meal, and it resolved spontaneously without significant problems. In our previous study, we observed eight patients with chylous leakage of 39 patients, and it also resolved spontaneously. 8 Therefore, in our experience, the amount of chylous leakage after dietary intake was usually small and it did not cause a significant problem. Therefore, we removed the drain on postoperative day 2 or 3 as long as the amount of chylous leakage was limited.
Our final goal was to determine the appropriate template of LND in accordance with the primary location of UC of the UUT. If LN recurrence occurs near the LND area after the patient has a diagnosis of pN0 disease, the area with LN recurrence should be considered as one of the primary landing sites, and it should be incorporated into the regional LND template. In the present study, although the follow-up duration was too short to draw a definitive conclusion, after nephroureterectomy, LN recurrence in the right presacral area developed in one patient with a right lower ureteral tumor. Based on our observation as well as the previous findings from bladder cancer studies showing that primary lymphatic drainage of bladder cancer extends into the obturator, internal iliac, external iliac, and presacral LNs, 18 –20 we have made minor modifications to our protocol, whereby the presacral area is included in the LND template in patients with a lower ureteral tumor, although presacral LNs had already been removed based on surgeons' decisions in six patients with lower ureteral tumors. Because we did not observe LN recurrence within/near the LND area in patients with pelvic/upper ureteral carcinoma, we consider that the present template is appropriate for patients with clinically node-negative pelvic/upper ureteral carcinoma, and that LND can be effectively performed laparoscopically.
A limitation of our study was its small sample size. The follow-up duration was also too short to observe whether LN recurrence occurred within/nearby the LND area. In addition, the surgeons and pathologists differed between the two institutions. Our study could not determine in which patients we can safely omit LND. Future studies to improve preoperative staging are needed for patient stratification. We consider, however, that our study revealed that LND during LNU was performed effectively and safely. In addition, IHC and survival analyses suggested improved local disease control because of LND.
Conclusion
LND during LNU was performed effectively and safely. We consider that the present template represents regional LNs for patients with clinically node-negative pelvic/upper ureteral carcinoma, while presacral LNs may be incorporated into the regional LND template for patients with clinically node-negative lower ureteral carcinoma.
Footnotes
Disclosure Statement
No competing financial interests exist.