
Abstract
Purpose:
This study was to evaluate the effect of intraoperative continuous infusion of dexmedetomidine on intraocular pressure (IOP) in patients undergoing robot-assisted laparoscopic radical prostatectomy (RALRP) in the steep Trendelenburg (ST).
Materials and Methods:
Sixty-eight patients were randomly divided into two groups. The dexmedetomidine group (Group D, n=34) received a continuous infusion of dexmedetomidine at a rate of 0.4 μg kg−1 hour−1 from the induction of anesthesia until the end of the ST position, while the control group (Group C, n=34) received an equal volume of physiologic saline at the same rate under conventional general anesthesia with sevoflurane and remifentanil. IOP was measured at 11 predefined time points for all patients.
Results:
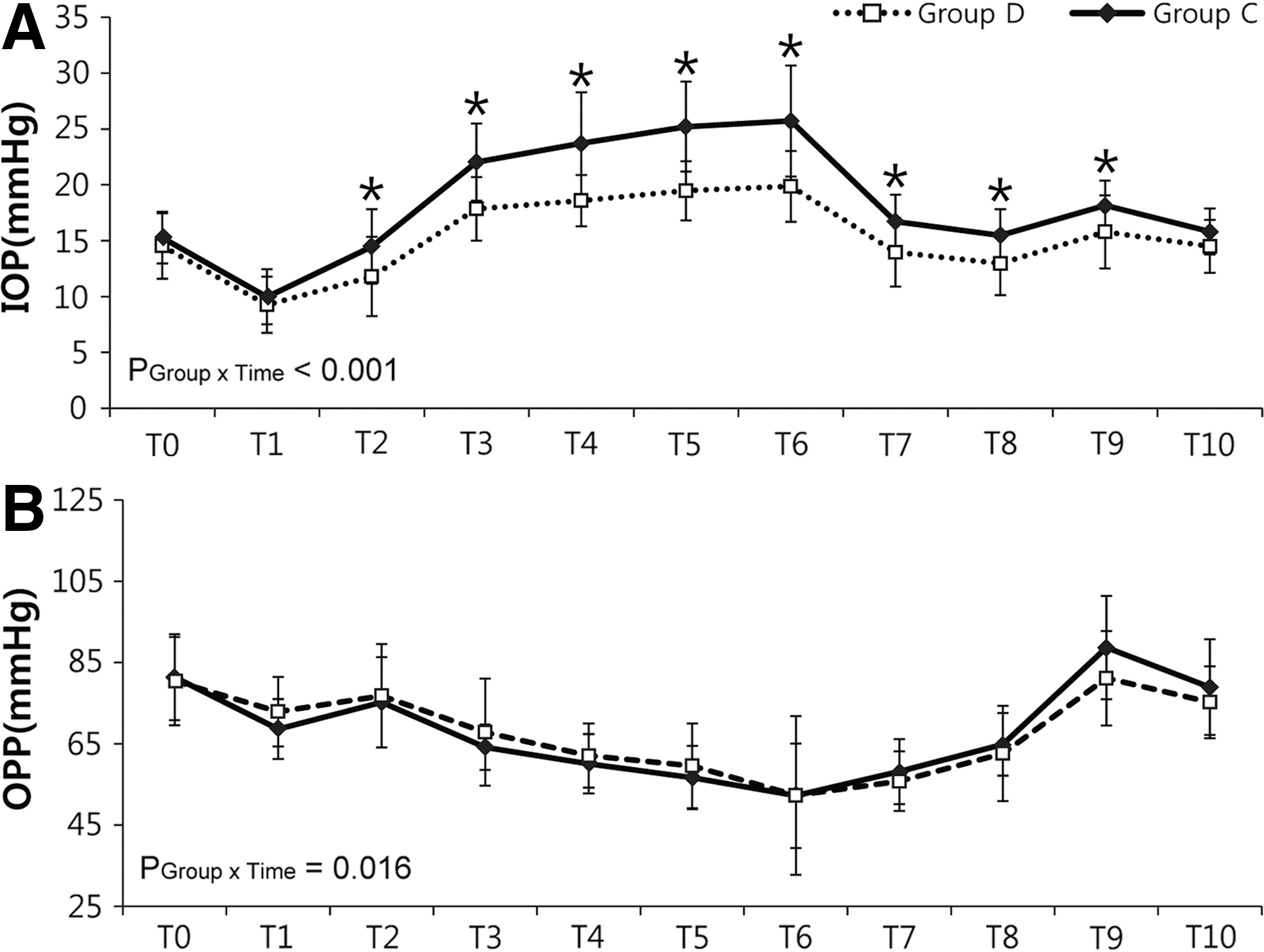
Significant differences in IOP were detected between the two groups by a linear mixed model analysis (p<0.001). The highest mean IOP was 19.9±5.0 mm Hg in Group D and 25.7±5.0 mm Hg in Group C; both were measured 60 minutes after the patients had been placed in the ST position. No significant between-group differences in ocular perfusion pressure, mean blood pressure, or heart rate were observed between the two groups. No ocular or other complications were noted.
Conclusion:
Intraoperative continuous infusion of dexmedetomidine may help alleviate IOP increase in patients undergoing RALRP in the ST position.
Introduction
P
The use of robot-assisted laparoscopic radical prostatectomy (RALRP) has increased since it was first introduced. 5,6 Despite its high cost, owing to advantages such as fewer respiratory complications, lesser transfusion, faster recovery time, and smaller incisions with less postoperative analgesics, this minimally invasive technique has been preferred over conventional open prostatectomy. 5,7
However, during RALRP, patients are placed in the steep Trendelenburg (ST) position under pneumoperitoneum for a prolonged period to achieve better surgical access. 8 This position may cause severe ophthalmic complications owing to increased IOP and decreased OPP. 9 –11 Recently, serious optic damage has been reported after robot- or laparoscopic-assisted radical prostatectomy. 12 In addition, our recent study demonstrated that IOP rises consistently during RALRP. 10 Moreover, most patients undergoing RALRP are elderly patients who are more vulnerable to ocular complications. 13 Therefore, a strategy for reducing the IOP increase during surgery is important for preventing postoperative ophthalmic complications.
Dexmedetomidine, a potent highly preferential α2-adrenergic agonist, has hypnotic, sedative, analgesic properties, and sympatholytic effects without severe respiratory depression. 14 –16 Previous studies have shown that a bolus injection of dexmedetomidine as a premedication can mitigate the IOP increase that occurs following endotracheal intubation. 17,18 However, no study has determined the effect of dexmedetomidine in a state of sustainably increased IOP such as that in the ST position.
The present randomized controlled trial was thus performed to determine the effect of a continuous infusion of dexmedetomidine on the IOP increase in patients undergoing RALRP.
Materials and Methods
Study design
The study was approved by the Institutional Review Board and Hospital Research Ethics Committee of Severance Hospital, Yonsei University Health System, Seoul, Korea, on May 20, 2013, and registered at
Patients who had previously undergone ophthalmic surgery, had received medications for glaucoma, had concomitant ophthalmic disease (glaucoma, diabetic retinopathy, cataract, and retinal detachment), and those who had a baseline IOP >30 mm Hg after screening were excluded from the study. Patients with uncontrolled hypertension, bradycardia <60 beats minute−1, ventricular conduction abnormalities, congestive heart failure, hepatic failure, renal failure, hypersensitivity to anesthetic drugs, and neurological or psychiatric illnesses were also excluded.
Sample size calculation
Sample size calculations were based on a previous study, 10 in which we found that the mean±SD difference in IOP at 30 minutes after CO2 pneumoperitoneum in the ST position with propofol-based total intravenous (IV) anesthesia was 19.97±3.76 mm Hg, whereas that for sevoflurane anesthesia was 23.5±4.32 mm Hg. To detect a 3.5 mm Hg difference in IOP between the two groups (two-sided α 0.05, power 90%), 29 patients were needed in each group. Considering a possible 20% dropout rate, 35 patients were enrolled in each group.
Randomization and allocation
Patients were randomly allocated to either the dexmedetomidine infusion group (Group D, n=34) or the saline infusion group (Group C, n=34) after enrollment. This randomization was performed according to a table of random sequence, which was generated in a website (
Procedure
Dexmedetomidine was mixed with 48 mL physiologic saline in a 50-mL syringe to achieve a final concentration of 4 μg mL−1. An equal volume of physiologic saline was prepared in the same manner. Two anesthesiologists participated in the procedure; one, who is the chief investigator, was aware of the patient allocation and prepared the drugs in accordance with those allocations, and the other was an investigator who was blinded to the group assignment and only collected the data without involving the anesthetic management. Each patient was provided standardized anesthetic management by blinded anesthetists who were not related in this study. The ophthalmologist, surgeons, recovery nurses, and patients were also blinded to the group allocation. All patients underwent preoperative eye examinations by an ophthalmologist who was not involved in the study to measure the preoperative IOP and to inspect the fundus and cornea for ophthalmic disorders such as glaucoma, diabetic retinopathy, cataract, and retinal detachment.
Premedication was given with intramuscular midazolam 0.05 mg kg−1 1 hour before surgery, and glycopyrrolate 0.2 mg was injected just before anesthesia. After standard monitoring of mean blood pressure (MBP), electrocardiogram, and oxygen saturation (SpO2), radial artery catheterization was performed under local anesthesia to enable continuous blood pressure monitoring and gas analysis. Anesthesia was induced with propofol (2 mg kg−1), rocuronium (0.6 mg kg−1), and remifentanil infusion (0.05–0.1 μg kg−1 minute−1). Controlled ventilation was achieved in 40% oxygen with air at a respiratory rate of 10 to 20 breaths minute−1 by applying a tidal volume of 8 mL kg−1 of the ideal body weight, a positive end-expiratory pressure of 5 cm H2O, and an 1:2 inspiratory to expiratory ration (I:E) ratio to maintain the end-tidal CO2 (ETCO2) at 35 to 42 mm Hg. After induction, a central venous catheter was placed through the right internal jugular vein to monitor central venous pressure (CVP). Dexmedetomidine or saline (0.4 μg kg−1 hour−1) was infused continuously from the induction of anesthesia until the end of the ST position.
All patients were treated in the same way and underwent conventional inhalation anesthesia with sevoflurane (0.6–2.3 age-adjusted minimal alveolar concentration) and remifentanil (0.03–0.1 μg kg−1 minute−1) to maintain either a bispectral index (BIS) monitor (Aspect A-2000®; Aspect Medical System, Inc., Newton, MA) target range of 40 to 60 or hemodynamic stability. Topical local anesthetic eye drops containing 0.5% proparacaine HCl (Alcon, Seoul, Korea) were instilled in the eyes of patients in both groups. All IOP measurements were performed by the same ophthalmologist who was blinded to group allocation using a Tono-Pen AVIA® applanation tonometer (Reichert, Inc., Depew, NY) at 11 separate time points (Table 1). 19 The IOP measurements were repeated thrice for each eye at each time point, and the median value was used in the analysis. A 20-mm Hg intra-abdominal pressure pneumoperitoneum was generated by a CO2 insufflator in the supine position. Then, when the patient was in the 29° Trendelenburg position, as displayed on the remote controller of the surgical bed, the intra-abdominal pressure was reduced to 15 mm Hg and this pressure was maintained throughout the surgery. Hypotension (MBP <65 mm Hg) and bradycardia (heart rate [HR] <40 beats minute−1) were treated with IV ephedrine 4 mg and atropine 0.5 mg, respectively.
ST=steep Trendelenburg.
Statistical analysis
IBM SPSS Statistics 19.0 (SPSS, Inc., Chicago, IL) and SAS version 9.2 (SAS Institute, Inc., Cary, NC) were used for statistical analysis of the data. The mean±SD was used for continuous variables and the number of patients (percentage) for categorical variables. IOP was measured repeatedly thrice for each eye at 11 different time points; the median value was used as a representative value in the analysis with a linear mixed model. 10 The OPP, MBP, HR, ETCO2, CVP, peak inspiratory pressure (PIP), BIS, and end-tidal sevoflurane concentration were analyzed in the same way as IOP. Differences over time were compared between the groups using a group-by-time interaction. When significant differences in the repeatedly measured variables were detected, a post hoc analysis was performed with the Bonferroni correction to facilitate multiple comparisons. Considering that the variables were measured repeatedly in each patient, a correlation coefficient was obtained between IOP and MBP, CVP, ETCO2, and PIP over each time period using a linear mixed model, and Fisher's z transformation was used to calculate the p-value. All other data were analyzed using Student's t-test, the chi-square test, or Fisher`s exact test. Statistical significance for a two-tailed test was defined as a p-value<0.05. For significance after post hoc analysis with Bonferroni correction, an adjusted p-value was required with a new threshold of p<0.05/the number of time points.
Results
A total of 70 patients were evaluated for eligibility, and two patients with senile cataracts diagnosed during the preoperative ophthalmologic examination were excluded. The remaining 68 patients were randomly divided into two groups. One patient in Group C was dropped from the study because of severe subcutaneous emphysema that occurred during surgery; the patient was transferred to the intensive care unit without postoperative extubation. As a result, 67 patients completed the study (Fig. 1).
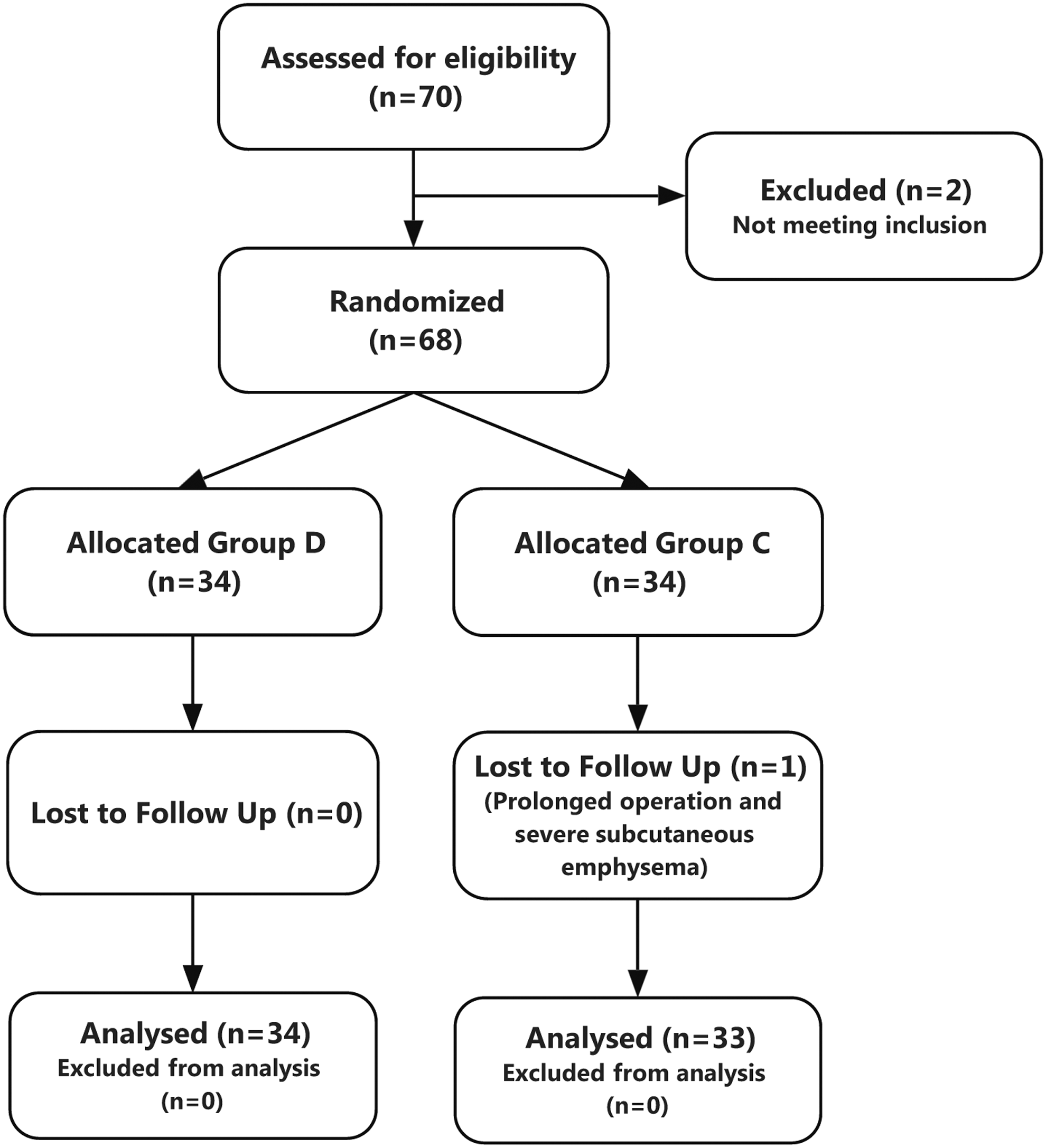
CONSORT flow diagram. Group C, control group; Group D, dexmedetomidine group.
Demographic data were comparable between the two groups (Table 2). Except for the total amounts of remifentanil and ephedrine administered, there were no significant differences between the two groups. Total fluids, blood loss, and urine output were also not significantly different (Table 3). Patients in Group D received significantly less remifentanil and more ephedrine than those in Group C (p=0.029 and p=0.021, respectively). During surgery, there was no noticeable between-group difference in arterial blood gas at T1, T4, and T8. Neither were HR and BIS significantly different between the two groups. Moreover, no patients experienced bradycardia (defined as HR <40 beats minute−1). The end-tidal sevoflurane concentration was significantly lower in Group D than Group C between T6 and T8 after post hoc analysis with the Bonferroni correction (p=0.0040, p<0.0001, and p=0.0004 at T6, T7, and T8, respectively) (Table 4). For significance, an adjusted p-value was required of less than 0.00625 (p<0.05/8).
Values are mean±SD, numbers (%).
ASA=American Society of Anesthesiologists; BMI=body–mass index; Group C=control group; Group D=dexmedetomidine group.
Values are mean±SD.
p<0.05.
drug=dexmedetomidine or saline.
Time points are defined in Table 1.
Values are mean±SD.
p<0.05.
The degree of conformity of IOP value measured six times at each time point is represented in Appendix Table A1. The result indicates a high consistency because every measured intraclass correlation coefficient (ICC) value is greater than 0.75. 20 Baseline IOP, which was measured before induction, was similar in both groups. No patient in either group had a baseline IOP >20 mm Hg. Significant differences in IOP over time were found between the two groups through the linear mixed model analysis (p<0.001) (Fig. 2A). After post hoc analysis with the Bonferroni correction, the mean IOP of Group D was significantly lower compared with Group C from T2 to T9 (with a threshold of p<0.00455).The linear mixed model analysis also indicated that there was a significant between-group difference in OPP (Fig. 2B). However, after the post hoc analysis and the application of the Bonferroni correction, this was no longer significant at any specific time point (with a threshold of p<0.00455). A similar finding was obtained for MBP (Fig. 3A). There were no significant between-group differences in CVP, ETCO2, or PIP (Fig. 3B–D).
Mean intraocular pressure (IOP)
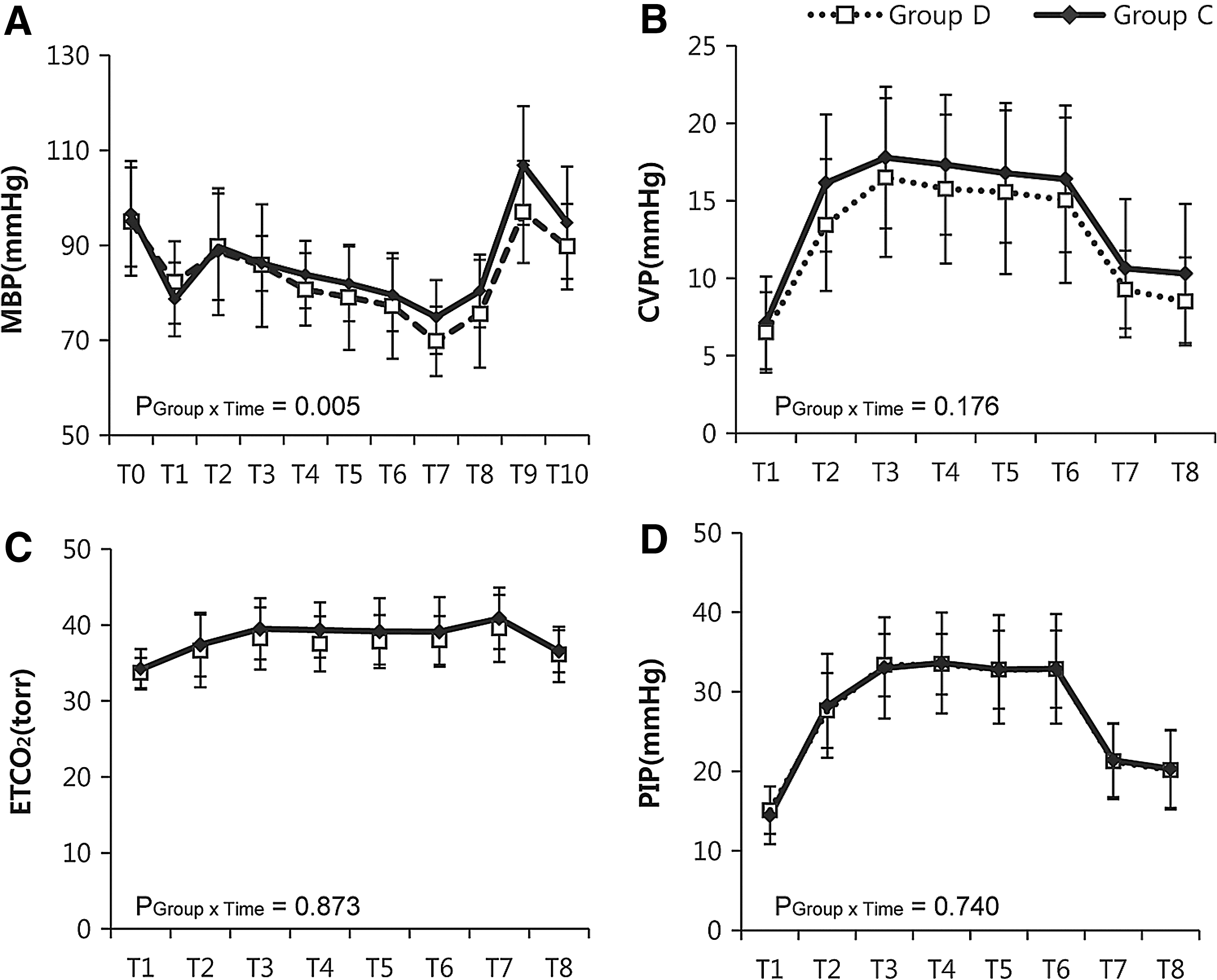
Mean blood pressure (MBP)
A further analysis was carried out to detect any correlations between IOP and MBP (T0–T10), CVP (T1–T9), PIP (T1–T8), and ETCO2 (T1–T8). IOP was found to be correlated with CVP (r=0.49, 95% confidence interval [CI]: 0.28–0.65, p<0.001) and ETCO2 (r=0.60, 95% CI: 0.42–0.73, p<0.001). No patient suffered ocular or any other complications.
Discussion
The present study demonstrated that intraoperative continuous infusion of dexmedetomidine (0.4 μg kg−1 hour−1) until the end of ST position significantly helped alleviate IOP increase in patients undergoing RALRP. Furthermore, this can be achieved without hemodynamic instability. As in previous studies, a gradual increase in IOP was observed with a pneumoperitoneum in the ST position. 6,10 The majority of the patients were elderly and even more vulnerable to an eye injury from the increase in IOP. 13,21,22 There have been a number of reports regarding the impact of a sudden increase in IOP during surgery on optic nerve damage. 23,24 Although these studies have not clearly shown that the temporary increase in IOP and decreased OPP have any clear effect and safe thresholds on optic nerve damage, the risk still exists for vulnerable patients with coexisting glaucoma or those who are of an advanced age.
Dexmedetomidine is the most potent and highly selective a2 agonist, and it also exhibits attenuating sympathetic activities. 25,26 a2 agonists have previously been shown to be effective at controlling IOP during surgery. 27,28 A bolus injection of dexmedetomidine as premedication was reported to mitigate the IOP increase that occurs following endotracheal intubation. 17,18 However, to the best of our knowledge, no study to date has evaluated the effects of a continuous infusion of dexmedetomidine on the state of sustainably increased IOP that occurs during procedures such as RALRP.
In the present study, dexmedetomidine attenuated the increase in IOP not only at T4, which was the primary endpoint of the study, but also throughout surgery (p<0.001). A previous study reported an IOP value of 23.5±4.3 mm Hg in the sevoflurane group and 19.9±3.8 mm Hg in the propofol group (difference=3.5 mm Hg; 95% CI: 1.5–5.5; p=0.0019) after 30 minutes in the ST position. 10 In the present study, the IOP at T4 was 23.7±4.6 mm Hg in Group C, which is similar to the previous study, 10 but it was 18.6±2.3 mm Hg in Group D, a greater decreased value compared with the propofol group in the previous study (difference=5.1 mm Hg; 95% CI: 3.4–7.0; p<0.001). In the present study, IOP was compared between the two groups every 15 minutes until 60 minutes after ST position. The highest IOP value was observed at T6 (60 minutes after ST position); the highest IOP was 25.7±5.0 mm Hg in Group C and 19.9±5.0 mm Hg in Group D (difference=5.9 mm Hg; 95% CI: 3.7–8.0; p<0.001). The differences in the IOP values between the two groups increased gradually at each time point up to T6.
Dexmedetomidine may be associated with hemodynamic changes such as hypotension or bradycardia. 29 Furthermore, RALRP is usually performed in elderly patients with various cardiovascular comorbidities. Consequently, maintenance of hemodynamic stability is as essential as the reduction in IOP in elderly patients. In this study, therefore, a continuous infusion of 0.4 μg kg−1 hour−1 dexmedetomidine was thus administered without a loading dose from induction until the end of the Trendelenburg position. 30 No severe hemodynamic instability was noted in either group. MBP in Group D was slightly lower (3%–6%) than that in Group C from the T4 time point, which was 30 minutes after ST position. However, there was no statistical significance except at the T9 time point (5 minutes after extubation), where MBP in Group C was 11% higher than that in Group D. The lowest MBP in Group D was 60 mm Hg, and the lowest HR was once 43 beats minute−1 in Group D. As seen in Table 3, total amounts of administered ephedrine were higher in Group D than in Group C. HR showed a similar trend as MBP and was slightly lower in Group D than in Group C from T4 to T9, with no significant difference. Although the lowest HR was observed in Group D, there was no bradycardia (HR <40 beats minute−1) that had to be treated with atropine in both groups. A possible explanation may be that the preinduction administration of glycopyrrolate for premedication may have mitigated the potential for bradycardia. In addition, the concentrations of anesthetic agents other than dexmedetomidine were significantly lower in Group D than in Group C, as inferred by the end-tidal sevoflurane concentrations and the amounts of infused remifentanil. Despite a higher amount of ephedrine in Group D, these study findings may have clinical significance, given that only this low-dose infusion of dexmedetomidine significantly prevented a sustained increase in IOP in elderly patients without hemodynamic instability under a prolonged ST position with pneumoperitoneum.
In addition, the correlations between IOP and CVP and IOP and ETCO2 observed in the present study are in accordance with previous reports. 6 However, there was no difference in ETCO2 and CVP between the two groups. Therefore, dexmedetomidine may reduce IOP through a mechanism that does not affect CVP or ETCO2. Previous reports on the influence of dexmedetomidine on the regulation of IOP have noted that direct vasoconstriction in afferent blood vessels of the ciliary body results in decreased aqueous humor production, which may affect the decrease in IOP. 31 It is also possible that it is affected by a decrease in the vasomotor tone of the ocular drainage system and an acceleration of aqueous humor outflow. 32
However, we did not evaluate the exact mechanisms by which dexmedetomidine attenuated the IOP increase in this study, which is a limitation. Further studies are thus required for more precise results. Also, the variability of IOP throughout the day could be considered as a confounder. However, diurnal variation is acceptable in normal eyes, whereas IOP in glaucomatous eyes is variable throughout the day. 33 Since IOP measurements in the present study were performed between 8 am and 3 pm in both groups, we believe that the time when surgery was performed would not be a confounder. Another limitation of the present study is that there was no significant difference in OPP between the two groups. This is because we calculated OPP as MBP–IOP. Although MBP was comparable between the two groups, it was still lower in Group D. However, taking into account the harmful effects of the increase in IOP, as shown in previous studies, 12,34,35 we believe that our protocol is a practical method for reducing the increase in IOP without any accompanying hemodynamic instability.
Conclusions
Intraoperative continuous infusion of dexmedetomidine (0.4 μg kg−1 hour−1) may help alleviate IOP increase in patients undergoing RALRP in the ST position without leading to any hemodynamic instability.
Footnotes
Acknowledgments
The authors are grateful to Dong Wook Kim and Jung Hwa Hong (Biostatistics Collaboration Unit, Yonsei University College of Medicine, Seoul, Korea) for their help with the statistical support.
Disclosure Statement
The authors have no conflicts of interest to report.
Abbreviations Used
Appendix
| Time | ICC (95% CI) |
|---|---|
| T0 | 0.866 (0.810–0.910) |
| T1 | 0.922 (0.890–0.948) |
| T2 | 0.959 (0.942–0.973) |
| T3 | 0.969 (0.956–0.979) |
| T4 | 0.977 (0.968–0.985) |
| T5 | 0.973 (0.962–0.982) |
| T6 | 0.973 (0.961–0.982) |
| T7 | 0.945 (0.921–0.963) |
| T8 | 0.925 (0.893–0.950) |
| T9 | 0.940 (0.915–0.960) |
| T10 | 0.842 (0.775–0.894) |
Time points are defined in Table 1.
≥0.75 good reliability, 0.5 to <0.75 moderate reliability, <0.5 represented poor reliability.
CI=confidence interval; ICC=intraclass correlation coefficient.