
Abstract
Objective:
Flexible cystoscopy is a common practice in urology. We wanted to determine whether a retention time of 5 minutes between the administration of a local anesthetic lubricant and flexible cystoscope insertion decreased the degree of discomfort or pain in the patient.
Materials and Methods:
Males who underwent flexible cystoscopy during 5 months were randomized in a prospective study. They were divided into two groups. In the first one, the Cathejell lubricant with lidocaine 12.5 g was administered and cystoscopy was performed immediately. In the second one, the same lubricant was maintained in the urethra for 5 minutes before the performance of cystoscopy. After scanning, all the patients were requested to indicate the degree of perceived pain on a visual pain scale from 0 to 10, with 0 being no discomfort and 10 being the maximum degree of pain bearable. As a secondary objective, the relationship of pain to age and to the type of cystoscopist (urologist/resident doctor) was studied. For statistical analysis, a Student's t-test for independent samples and correlation analysis were used.
Results:
A total of 242 patients were studied, 110 in the immediate group and 132 in the 5-minute delay group, with samples being homogeneous for the age and type of cystoscopist. The mean in the pain scale in the immediate group was 2.41, and in the 5-minute delay group was 2.04, with no significant differences between them (p=0.175). There was no relationship with age (r=−0.061, p=0.348) or with the type of cystoscopist (2.06 of average pain in the associate group, 2.35 in the resident, p=0.28).
Conclusions:
There is no benefit in waiting a short time after the administration of intraurethral lubrication with a local anesthetic in flexible cystoscopy in men. There is also no relationship between the patient age or the type of cystoscopist (urologist/resident doctor) and perceived pain.
Introduction
F
A study published in 2004, agrees with the benefit of using a topical anesthetic lubricant versus lubricant without anesthesia, both in urethral catheterization and in performing flexible cystoscopy. 2 On the contrary, another study concludes that there are no differences in the perception of discomfort and pain by patients when an anesthetic lubricant or simple lubrication is used, if the waiting time before the exploration is 5 minutes. 3 In addition, a meta-analysis of 2008 denied this improvement in pain when using lubricants with anesthesia. 4
Regarding the issue of the retention time of an anesthetic intraurethral lubricant, it is clear that a prolonged time between 15 and 20 minutes favors a decrease in the sensation of discomfort in flexible cystoscopy. 5 Moreover, time under 3 minutes appears not to be useful for this purpose. 6
Reviewing the information displayed in the monograph of the lubricant with a local anesthetic Cathejell 12.5 g (used in this study); anesthesia is achieved within 5 minutes, following topical application. 7
This study aims to determine whether a short, clinically manageable 5-minute time delay, between lubrication and insertion of the cystoscope versus immediate insertion, reduces discomfort in male patients undergoing flexible cystoscopy.
Materials and Methods
During a 5-month period, all males who underwent flexible cystoscopy in our center were included and a randomized prospective study was performed.
Patients were divided into two groups based on the last number present in their hospital internal identification number (medical record number). The ones ending in an even number were placed in the immediate group. Those with an odd number were placed in the 5-minute delay group.
The general procedure was performed as follows by a resident or a consultant doctor and took an average of 1.5–2 minutes. A 15.5F flexible cystoscope was used. First, the penis was cleaned with iodine solution. Then, 12.5 g of Cathejell lubricant with lidocaine at room temperature was slowly administered along the urethra by the cystoscopist. In the immediate group, Cathejell was administered and the cystoscopy was performed without delay. In the 5-minute delay group, the same type of lubricant was maintained with a penile clamp in the urethra for 5 minutes before cystoscopy. After the procedure, all patients were requested to mark the degree of perceived pain on a visual pain scale from 0 to 10, with 0 being no discomfort and 10 being the maximum degree of pain bearable (VAS scale). 8 The assessment was made by the nurse a few minutes after the procedure, without the presence of the cystoscopist.
Subjects with anatomical or neurological abnormalities, which could alter the degree of pain in a normal cystoscopy (e.g., urethral stricture, foreskin sclerosis, and dementia), were excluded.
As a secondary objective, the relationship of pain with age and the type of cystoscopist (urologist/resident doctor) was studied. For this, the year of birth of all patients and the status of each cystoscopist (distinguishing between resident doctor and urologist) were recorded.
For statistical analysis, a Student's t-test for independent samples and a Pearson correlation analysis were used.
Results
A total of 242 patients, 110 in the immediate group and 132 in the 5-minute delay group, were studied.
The mean on the pain scale in the immediate group was 2.41 and in the 5-minute delay group was 2.04, with no significant differences between them (p=0.175). The mean difference was 0.371 (95% CI: −0.166 to +0.909) (Fig. 1).
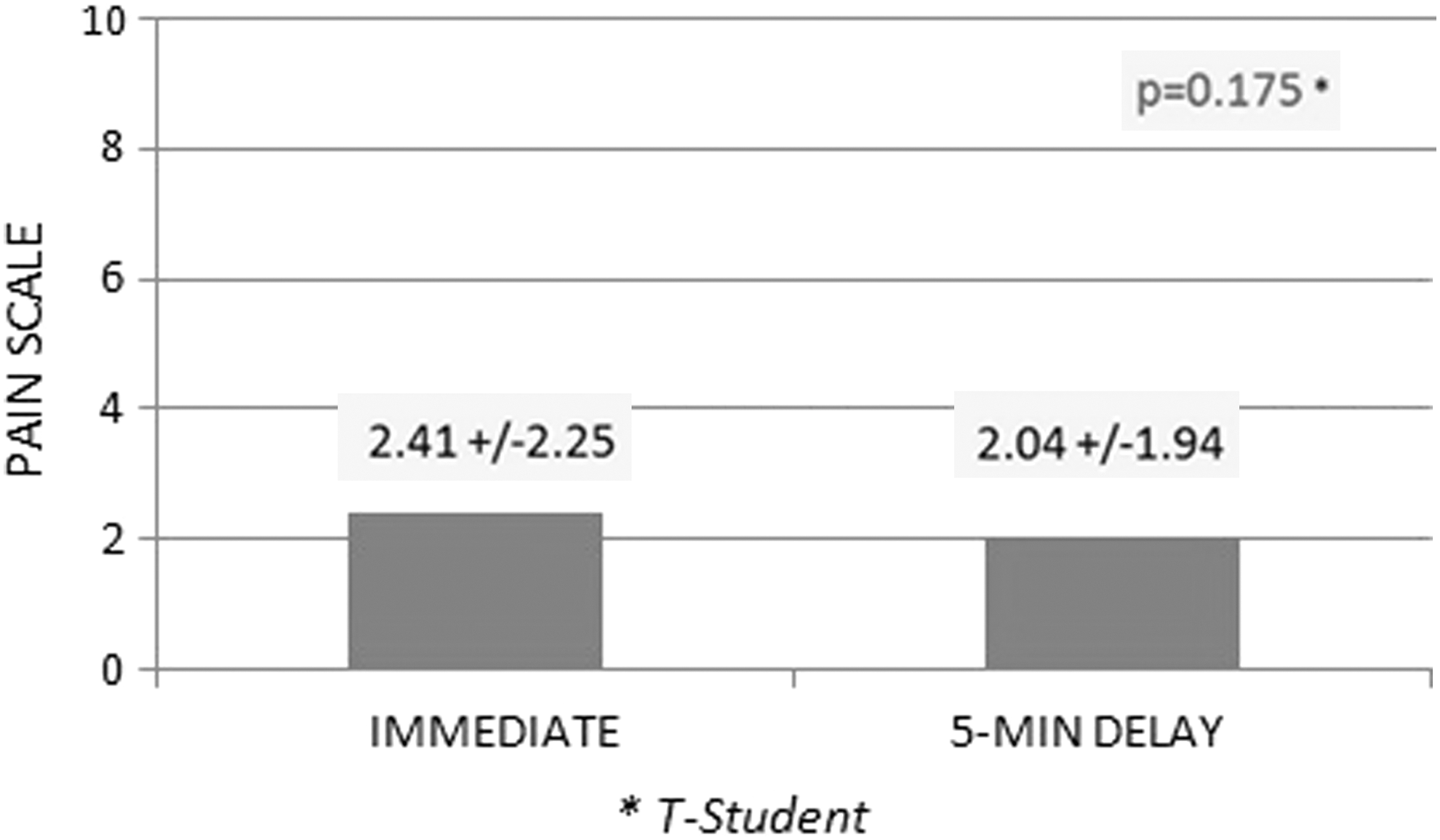
Average pain after performing flexible cystoscopy in both groups of patients studied.
The type of cystoscopist was also considered, distinguishing between urologist and resident doctor, with 119 cystoscopies being performed by urologists and 123 by resident doctors. Objectively, the mean of pain is lower in the urologist group (2.09±1.98) when compared with the resident group (2.35±2.19), with no statistically significant difference (p=0.28).
Regarding the influence of age on the patient's pain perception, no relationship between age and pain intensity (r=−0.061, p=0.348) was observed (Fig. 2).
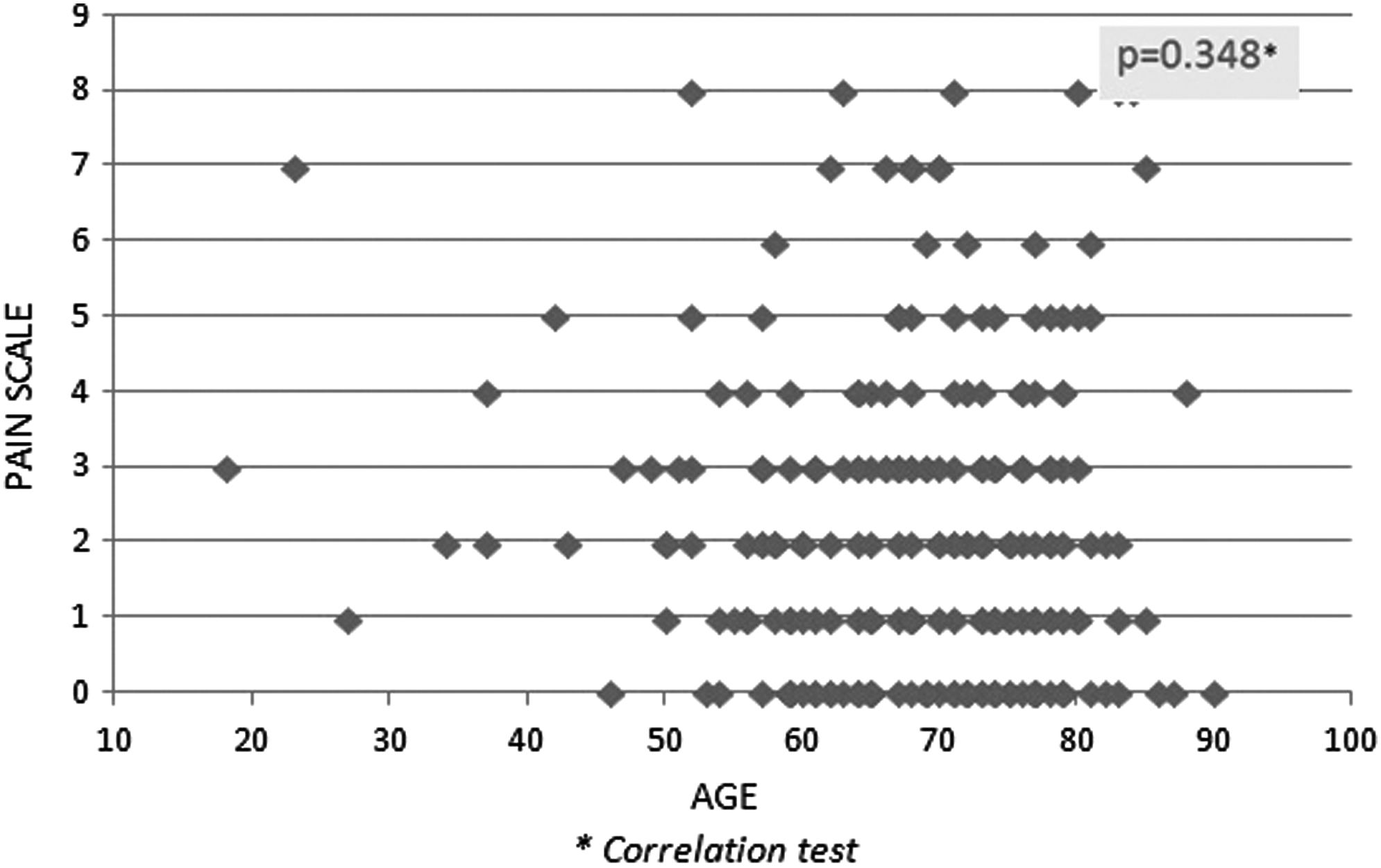
Diagram of points showing the relationship between perceived pain and patient age.
Discussion
After analyzing the results, it is immediately striking that the mean pain score in both the 5-minute delay groups as well as in the immediate insertion one is quite low. This shows that flexible cystoscopy in men is generally a well-tolerated procedure. This is unlikely to occur when a rigid instrument is used in cystoscopy, a situation where the recommendation is to wait 15 minutes to optimize the effect of the lubricant with a topical anesthetic. 9
On the contrary, and in reference to flexible cystoscopy, some studies have demonstrated no reduction in pain relief when using topical anesthetics for short periods of time. 6 Nevertheless, others conclude that there is an improvement with long periods of intraurethral anesthetic lubricant retention. 5 In relation to long retention times, the study of Choong et al. concluded that a period of 15 minutes produced a significant decrease in pain. In the present study, we have attempted to confer a degree of the reality of daily practice to intraurethral lubricant times, 5 minutes for one of the groups of patients (sufficient time, in theory, to achieve the full effect of the anesthetic). The differences, as noted, are minimal between the two groups. This conclusion is the same as that for prior reports. In the present case, a larger sample was used. 10
A meta-analysis by Aaronson et al. included four studies on the pain perceived by males undergoing flexible cystoscopy. In three of them, there was no pain improvement in patients receiving the anesthetic lubricant. The conclusion of this meta-analysis stated that there is less chance of developing moderate to severe pain in cases where the lubricant is used with lidocaine. 11
The results of our study cause us to consider the real benefit of waiting after administering the lubricant before performing a cystoscopy. This delay may affect the anxiety level of the patient and delay medical assistance without an apparent benefit, in accordance with the conclusions of this work. Another issue to take into account is if there is a benefit in using lubricant with or without a topical anesthetic. We have not studied this issue in our investigation, although our conclusions with those of another study make us think that the role of the topical anesthetic in these procedures is of little relevance. 3
A secondary objective was to observe if there was any difference in the perceived pain when doctors with more or with less experience performed the test: urologists or resident doctors. According to the results, although the pain was slightly lower in the group with urologists, there does not appear to be a difference. Nevertheless, it might well be useful to carry out a study with more patients who individualized each cystoscopist to objectively determine whether it really is a handler-dependent test.
No relationship between age and pain was found. Looking at Figure 2, the pain does not follow an increasing or decreasing trend with increasing age, low scores predominate in the different 10-year age groups. What can be concluded from this aspect is that, in general, male flexible cystoscopy is well tolerated in all age ranges. In a study, which attempted to find factors related to the perception of pain by electrical stimulation, it was concluded that age was a factor that did influence pain perception. 12 In the case of male flexible cystoscopy, however, this relationship was not observed.
The current study may have some limitations. For example, data collection was not anonymous, so patients might have been embarrassed to give an honest answer about their pain. Another bias can be found in those individuals who were not facing their first cystoscopy. In our hospital, we had always waited several minutes after intraurethral lubrication. Thus, those men who faced a second or subsequent cystoscopy already knew from the previous occasion that they had to wait for the topical anesthetic to take effect. We think this aspect may have influenced the slightly higher pain average in the immediate group. As for the relationship between pain and the type of cystoscopist, we know that the results would have had more value if handlers had been individualized and then compared the pain produced by each. However, we think that this would have required a larger sample, just to know whether there are differences in perceived pain depending on the professional performing the test.
Although some studies have concluded that more retention time helps reduce pain, even some specific maneuvers, like allowing the patient to view the test, reduce the degree of nuisance. 13 What we have wanted in this study has been to reproduce and compare a situation we consider common or normal when a flexible cystoscopy is going to be carried out: waiting a reasonable time of 5 minutes with the anesthetic without additional maneuvers.
Conclusions
There is no benefit in delaying cystoscopy by a short interval (5 minutes) after administration of intraurethral lubrication with a local anesthetic in flexible cystoscopy in men. There is also no relationship between the age of the patient or the type of cystoscopist (urologist/resident doctor) and perceived pain.
Footnotes
Disclosure Statement
The authors declare that they have no conflict of interests.