
Abstract
Purpose:
To assess the feasibility, safety, and efficacy of the laparoendoscopic single-site (LESS) donor nephrectomy (LESSDN) procedure after experience with the LESS-plus-one-trocar donor nephrectomy (LEPODN) procedure.
Patients and Methods:
From 2009 to 2014, 126 left laparoscopic donor nephrectomies (LDNs) were performed, including 59 Standard (Std)-LDN, 30 LEPODN, and 37 LESSDN. In the LEPODN procedure, a 5-mm trocar was added as a right-hand working trocar to the LESSDN procedure. A GelPOINT® platform was applied on a pararectal single incision in both LEPODN and LESSDN procedures. After performing the LEPODN procedure several times, each surgeon performed the LESSDN procedure.
Results:
Std-LDN, LEPODN, and LESSDN procedures were performed by 10, 10, and 7 surgeons, respectively. The mean operative time, estimated blood loss, warm ischemia time, time to ambulation, and length of postoperative hospital stay were the shortest for the LESSDN procedure (P<0.012, P=0.007, P<0.001, P=0.027, and P=0.001, respectively). No significant difference in the complication rate, delayed graft function rate, and mean 7-day post-transplant serum creatinine levels was observed among the three procedures. Individual results of the operative time and estimated blood loss for the LESSDN procedure were not significantly inferior to those of Std-LDN and LEPODN procedures for each surgeon.
Conclusions:
The LESSDN procedure can be introduced safely and effectively without compromising the operative time, complication rate, and graft function after experience with the LEPODN procedure among multiple surgeons. The LEPODN procedure may be an effective bridge from standard multiport LDN to LESSDN.
Introduction
A
Previous studies have shown the technical feasibility and safety of LESSDN. 8 –18 The reports of initial experiences have indicated the need for flexible instruments. 8 –11 Recent reports, however, have not indicated similar requirements. 12,13,15 –18 To replace the use of flexible instruments, the recent LESSDN procedures need a GelPort® or GelPOINT® (Applied Medical, Rancho Santa Margarita, CA) platform on a single incision that is made at the beginning of the procedure. This platform on a single incision of approximately 5–6 cm can provide sufficient instrumental triangulation to complete the procedure without using flexible instruments. The LESSDN procedure, however, has been performed by only a few surgeons even at high-volume centers. This indicates that LESSDN is still considered to be a challenging procedure to be safely taught to multiple surgeons, even without the need for flexible instruments. 15 –17 Previous reports of the LESSDN procedure have alerted that it should be performed only by experienced surgeons who are comfortable with the Standard (Std)-LDN procedure. 11,18
To facilitate the LESS procedure, we previously reported successful experience with LESS-plus-one-trocar living donor nephrectomy (LEPODN). 19 In brief, the GelPort platform was placed on a pararectal skin incision of approximately 5–6 cm, and a 5-mm trocar was inserted under the costal arch to provide a broader trocar triangulation. The technique for the LEPODN procedure has been successfully shared among eight urologic surgeons at our institution and may be an effective technical bridge to safely introduce the LESSDN procedure among multiple surgeons.
In this study, we assessed the feasibility, safety, and efficacy of the left LESSDN procedure after the experience with the left LEPODN procedure of multiple surgeons who were already comfortable with standard laparoscopic procedures. Once each surgeon performed the LEPODN procedure several times as the main surgeon, each performed the LESSDN procedure using the GelPOINT platform on a pararectal single incision without the use of flexible instruments with the guidance of the senior surgeons. The outcome of the LESSDN procedure after the LEPODN procedure was assessed and compared with that of the Std-LDN and LEPODN procedures.
Patients and Methods
From June 2007 to June 2014, 126 donors underwent the left LDN procedure at the Akita University Medical Center, Japan. Four right LDN and two right LEPODN procedures performed during the same period were excluded from this study because it was necessary to insert an additional trocar to retract the liver. Fifty-nine Std-LDN procedures were performed from October 2007 to October 2010, and 30 LEPODN procedures and 37 LESSDN procedures were performed from November 2010 to June 2014. All the surgeons who participated in this study had enough experience with standard laparoscopic radical nephrectomy but no experience with any LESS procedure using flexible instruments. Surgeons already comfortable with the Std-LDN procedure were allowed to perform the LEPODN procedures several times; subsequently, each surgeon performed the LESSDN procedure under the guidance of senior surgeons. Informed consent was obtained from all donors before the procedure. Donor eligibility at our institution has been described previously. 20 –22 The study protocols regarding Std-LDN, LEPODN, and LESSDN procedures were approved by the Akita University Medical Center Institutional Review Board.
Several perioperative clinical factors were compared among the three procedures, including the operative time (min), estimated blood loss (mL), warm ischemia time (WIT) of the graft kidney (sec), time to oral intake (days), time to ambulation (days), length of postoperative hospital stay (days), occurrence of delayed graft function (DGF), and serum creatinine levels (mg/mL) of the donors and recipients. DGF was defined as the requirement for dialysis therapy within 7 days after renal transplantation. Results of the operative time and estimated blood loss of the three procedures were individually assessed for each surgeon. Postoperative surgical complications were assessed using the Clavien–Dindo classification system. 23
The donors were placed in the right lateral decubitus position during the procedures. All intraperitoneal procedures were essentially similar because all three procedures involved only the use of straight instruments. The renal artery and vein were stapled and divided using a Multifire Endo-TA™ 30 stapler (Covidien, Boulder, CO) and scissors. The details of our intraperitoneal procedures have been described previously. 19
The Std-LDN procedure
The Std-LDN procedure has been described previously. 24 In brief, a 12-mm camera trocar was inserted in the pararectal line at the level of the umbilicus using an open laparotomy technique. A rigid 10-mm 30-degree digital laparoscope was used. A 5-mm left-hand trocar and a 12-mm right-hand trocar were inserted into the pararectal line 6–7 cm cranial to the umbilicus and under the costal arch of the anterior axillary line. A 12-mm assistant trocar was inserted at the side of the umbilicus, and the assistant trocar wound was extended by 5 or 6 cm to allow loading of a LapDisk® (Hakko Medical, Tokyo, Japan) immediately before division of vessels. The Multifire Endo-TA 30 stapler was inserted through the 12-mm right-hand trocar. The graft kidney was extracted using an ENDO CATCH™ II 15-mm specimen pouch (Covidien) inserted through the LapDisk. A 5-mm diameter drain was placed using a 5-mm left-hand working trocar.
The LEPODN procedure
The LEPODN procedure has been described previously. 19 In brief, the GelPOINT (or the GelPort in the first half of the cases) platform was placed on the pararectal incision (Fig. 1A). The three ports of the GelPOINT system were inserted in the gel cap (Fig. 1B). A rigid 10-mm 30-degree digital laparoscope with a 90-degree light adapter was also used. A 5-mm right-hand trocar was inserted under the costal arch at least 5-cm lateral to the edge of the GelPOINT (Fig. 1B, Fig. 2A). The Multifire Endo-TA 30 stapler and the ENDO CATCH II pouch were directly inserted through the opening in the gel that was manually created on the GelPOINT platform (Fig. 1B). The Multifire Endo-TA 30 stapler was inserted through the 12-mm left-hand trocar during the process of using the GelPort platform. A 19F diameter drain was intraperitoneally placed using a 5-mm right-hand trocar.

(
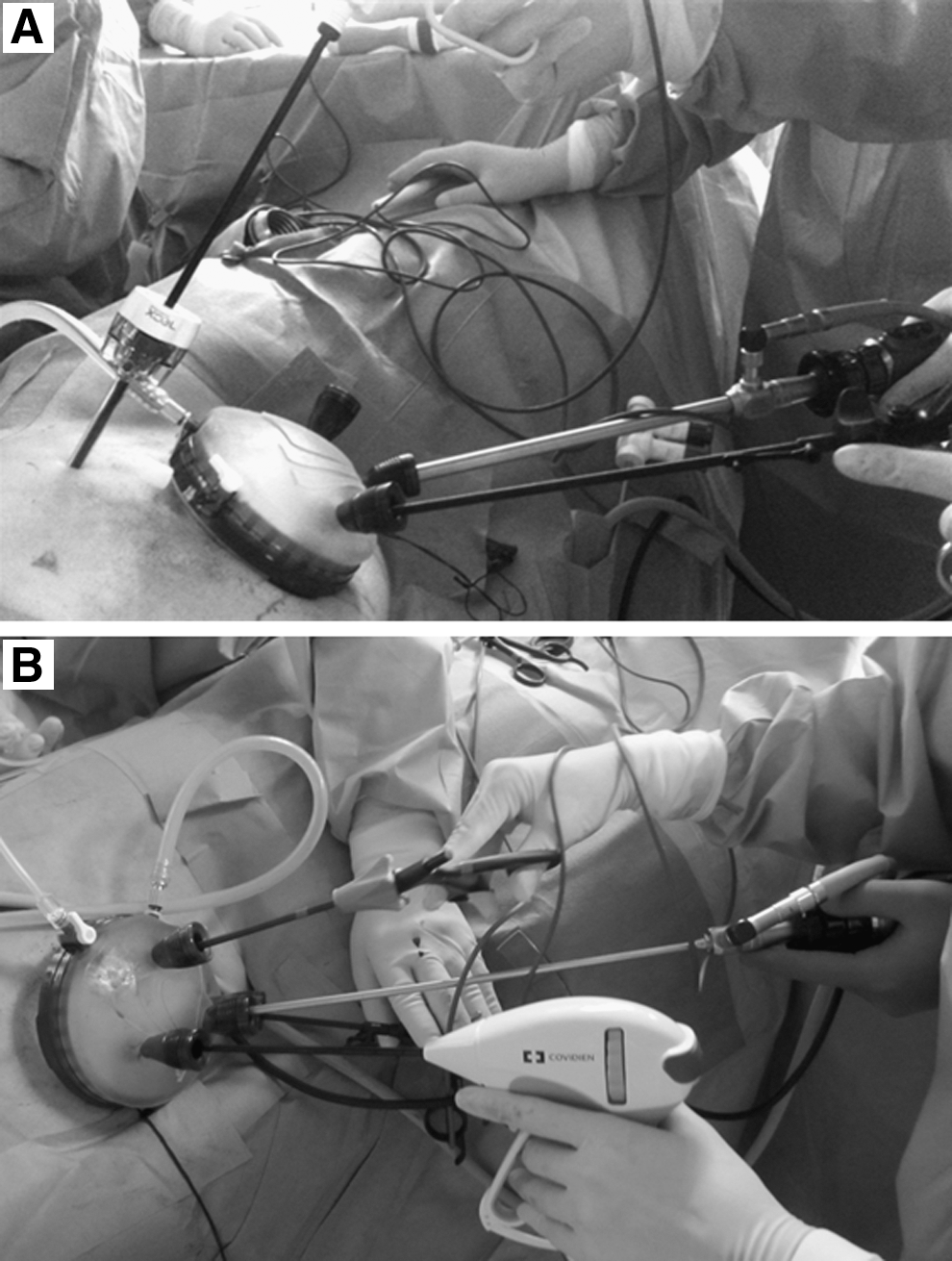
Intraoperative photographs of the GelPOINT® configuration in the laparoendoscopic single-site-plus-one-trocar donor nephrectomy (
The LESSDN procedure
The GelPOINT platform was placed on the pararectal incision (Fig. 1C). The four ports of the GelPOINT system were inserted in the gel cap (Fig. 1D, Fig. 2B). A rigid 30-degree long digital laparoscope (5 mm in diameter and 50 cm in length) or a standard rigid 10-mm 30-degree digital laparoscope with a 90-degree light adapter were selected, depending on the procedure conditions. A long, straight laparoscopic forceps was used at the left side. The Multifire Endo-TA 30 stapler and the ENDO CATCH II pouch were directly inserted through the opening in the gel that was manually created on the GelPOINT platform (Fig. 1D). A 10F diameter drain was intraperitoneally placed in the middle of the single pararectal incision.
Statistical analyses
Statistical analyses were performed using the SPSS ver. 22.0 software (SPSS, Inc., Chicago, IL). Fisher exact test, one-factor analysis of variance (ANOVA) test, and Tukey-Kramer test were used to examine differences among the three procedures. A P value of<0.05 was considered statistically significant.
Results
The demographic characteristics of all donors, who underwent the Std-LDN, LEPODN, and LESSDN procedures, are shown in Table 1. No significant differences in the donor age, height, weight, body mass index, preoperative creatinine clearance, and serum creatinine levels were noted among the three procedures (Table 1).
Std-LDN=standard laparoscopic donor nephrectomy; LEPODN=laparoendoscopic single-site-plus-one-trocar donor nephrectomy; LESSDN=laparoendoscopic single-site donor nephrectomy; SD=standard deviation; BMI=body mass index.
All 37 LESSDN procedures were completed with the use of only straight instruments and without any additional trocars beyond the working port on the GelPOINT device. Significant differences in the mean operative time, estimated blood loss, and WIT were found among the three procedures (P=0.012, P=0.007, and P<0.001, respectively, one-factor ANOVA). The estimated blood loss and WIT were significantly shorter for the LEPODN procedure than the Std-LDN procedure (P=0.027 and P=0.017, respectively, Tukey-Kramer test). The mean operative time, estimated blood loss, and WIT were significantly shorter for the LESSDN procedure than for the Std-LDN procedure (P=0.009, P=0.022, and P<0.001, respectively, Tukey-Kramer test). No significant differences in perioperative variables were found between the LEPODN and LESSDN procedures (Table 2).
Std-LDN=standard laparoscopic donor nephrectomy; LEPODN=laparoendoscopic single-site-plus-one-trocar donor nephrectomy; LESSDN=laparoendoscopic single-site donor nephrectomy; SD=standard deviation; WIT=warm ischemic time; DGF=delayed graft function.
Conversion to open surgery and blood transfusions were not needed in any of the three procedures. With the Std-LDN procedure, three patients experienced Clavien grade I complications, including two wound infections and one pneumothorax because of diaphragm injury, which did not necessitate any intervention. With the LESSDN procedure, two patients experienced a Clavien grade I complication, including a case of wound infection and a case of chylous ascites. There were no complications with the LEPODN procedure.
No significant differences in postoperative surgical complications and DGF rates were observed among the three procedures. No significant differences in the mean time to oral intake were observed among the three procedures. The time to ambulation and length of postoperative hospital stay were significantly shorter with the LESSDN procedure than with the Std-LDN procedure (P=0.022 and P=0.001, respectively, Tukey-Kramer test). No significant differences were found in mean serum creatinine levels of donors or recipients 7 days postoperatively among the three procedures. DGF occurred in two recipients undergoing both LEPODN and LESSDN procedures. With the LEPODN procedure, acute tubular necrosis of the graft caused DGF in two patients. With the LESSDN procedure, acute tubular necrosis caused DGF in one patient and heart failure from fluid overload for postoperative bleeding in another patient.
A total of 126 consecutive LDNs were performed by 12 surgeons, including 2 senior (T.H. and N.T.) and 10 junior surgeons. The Std-LDN, LEPODN, and LESSDN procedures were performed by 10, 10, and 7 surgeons, respectively. Of the 10 junior surgeons who performed the Std-LDN procedure, 8 performed the LEPODN procedure and 5 performed the LESSDN procedure. With regard to Std-LDN and LEPODN, two and three junior surgeons did not follow the next procedure because of job relocation, respectively. The five junior surgeons performed 3–5 LEPODN procedures before they performed the LESSDN under the guidance of senior surgeons. Individual data of the 4 junior surgeons, including the operative time and estimated blood loss, are shown in Table 3. The data of the fifth junior surgeon were excluded because he performed only one LESSDN procedure (Table 3).
Std-LDN=standard laparoscopic donor nephrectomy; LEPODN=laparoendoscopic single-site-plus-one-trocar donor nephrectomy; LESSDN=laparoendoscopic single-site donor nephrectomy; SD=standard deviation.
There were no statistically significant differences in the operative time and estimated blood loss among the three procedures for the four junior surgeons. The operative time, however, with the LESSDN procedure was significantly shorter than that with the Std-LDN procedure for one junior surgeon (P=0.004, Tukey-Kramer test).
Discussion
We developed the LEPODN reduced-port procedure before the application of the LESSDN procedure as a useful technical bridge. 19 An additional 5-mm right-hand trocar was added to the LESSDN procedure to broaden the triangulation of straight instruments and to facilitate the LESSDN procedure. Acceptable morbidity rates and favorable graft function were observed with the use of the LEPODN procedure. All 30 LEPODN procedures in this series were performed by 10 surgeons who were comfortable with conventional laparoscopic surgery using standard straight instruments. The results of the LEPODN procedure suggest that the technical concept and difficulty of the LEPODN procedure were similar to those of the Std-LDN procedure.
The additional 5-mm right-hand trocar used in the LEPODN procedure was removed in the LESSDN procedure after the LEPODN procedure was performed several times. A similar procedure concept using the GelPort in the single pararectal incision was initially reported by Ponsky and associates 25 for radical nephrectomy. The trocar formation on the GelPOINT platform was modified from that of the LEPODN procedure to optimize the LESSDN procedure in this series (Fig. 1B, 1D). To avoid hand collisions between the instruments and the camera, a rigid 30-degree camera 5 mm in diameter and 50 cm in length, a 90-degree light adapter, and a relatively long (43 cm) bipolar straight forceps were used in the LESSDN procedure. With these three instruments, the surgeons' hands could be kept at a sufficient distance, allowing smooth movements of the straight instruments.
Stamatakis and colleagues 17 reported the successful use of the “extra-long nondeflectable instruments” in a series of LESSDN procedures using the GelPOINT in the umbilical single incision, similar to that reported in our study. The optimization of device arrangements seems indispensable for the execution of the LESSDN procedure, although these arrangements may be influenced by the familiar customs at each institute.
The operative time was the shortest with the LESSDN procedure in the present series. Compared with the Std-LDN procedure, previous LESSDN series have shown equal 10,14 –16 or increased 11,12,17 operative time. Moreover, the estimated blood loss was less in the LEPODN and LESSDN procedures than in the Std-LDN procedure. The success of the LESSDN procedure in this series may result from the improvement of the surgeon's technique as well as the effectiveness of the introductory LEPODN procedure, which provided an ideal technical bridge for surgeons to learn the LESSDN procedure.
The concepts and techniques involved in the LESSDN procedure were shared among the seven surgeons, including the two senior surgeons. All surgeons successfully and safely completed the LESSDN procedure without using flexible instruments. The shortened operative time of one of the junior surgeons in the LESSDN procedure suggested that the surgical technique of the surgeon could be improved and refined despite the technical burden of the LESS surgery. In their LESSDN report, Stamatakis and coworkers 17 stated that they had abandoned their earlier approach to place the additional 6-mm port in a subxiphoid location because of their technical improvement. Our strategy, however, consisted of using the same concept as the LEPODN procedure to teach multiple surgeons instead of abandoning the approach.
In the present series, WIT was the shortest with the LESSDN procedure. Stamatakis and associates 17 also reported shorter WIT with the LESSDN procedure than with the Std-LDN procedure because of the usefulness of the GelPOINT platform. With the LEPODN and LESSDN procedures in this series and other recently reported studies, the single incision was made at the beginning of the surgery to extract the kidney graft quickly without extending the incision. 12,13,15 –19 In some initial reports of the LESSDN procedure, however, the laparoscopic procedure was performed using a small 2-cm single incision, then the incision was extended to 4–5 cm to extract the donor kidney after dividing the renal vessels. In this strategy, WIT with the LESSDN procedure was reported to be significantly longer than that with the Std-LDN procedure. 10,14 During our Std-LDN procedure, the extraction site was extended right before dividing the renal vessels, and the LapDisk was applied instead of the GelPOINT platform.
The shortened WIT with the LESSDN procedure in this series may not be a result of the wound extension timing of the extracting site but rather a result of the higher stability of the GelPOINT device than the LapDisk in the extracting procedure or improvement of our extraction technique during these three procedures.
There are some limitations of this study. First, to assess the real effect of the LEPODN procedure as the technical bridge, the control results of the transition from Std-LDN to LESSDN procedures directly without the LEPODN procedure should be evaluated. The direct strategy, however, should not be recommended because the LESSDN procedure is still an investigational procedure and donor safety must be prioritized. 16 Second, the number of cases in this series was small for each procedure and for each surgeon. Third, we did not compare the pain score and wound length to confirm whether there was less morbidity with the LESS procedure because of lack of these data in the Std-LDN procedure era. The shorter ambulation and hospitalization days in this study, however, may indicate lesser morbidity with the LEPODN or LESSDN procedure than with the Std-LDN procedure.
These results should be interpreted with care, considering the technical improvement during the three procedures, because the data of the Std-LDN procedure were historical retrospective data in this series. Further prospective investigation in a large sample is warranted to assess the real effect of our strategy to use the LEPODN procedure before the LESSDN procedure.
Fourth, the incision of our procedure was not placed umbilically but was placed pararectally, which could be relatively conspicuous but safer for donors. The reason is that we have performed conventional laparoscopic nephrectomy safely with a pararectal camera port in many patients. From the standpoint of cosmesis, the next step may be LESSDN with an umbilical camera port.
Conclusion
The LESSDN procedure can be introduced safely and effectively without compromising the operative time, complication rates, and graft function after multiple surgeons have gained technical experience by previously performing the LEPODN procedure. Thus, the LEPODN procedure may be an effective bridge from standard multiport LDN to LESSDN. The GelPOINT platform facilitated the LESSDN procedure and helped avoid the use of articulating instruments. Although the LESSDN procedure should still be considered as investigational and challenging, previous experience with the LEPODN procedure may be helpful in safely incorporating LESS procedures in the field of LDN.
Footnotes
Disclosure Statement
No competing financial interests exist.