
Abstract
Introduction and Objectives:
It is well known that adipose tissue plays a key role in the metabolic syndrome. We investigated whether visceral fat (VFA) and or subcutaneous fat (SQF) levels are associated with the tumor phenotype of small renal masses. Additionally, we sought to investigate the relationship between VFA and baseline renal function as measured by glomerular filtration rate.
Materials and Methods:
From 2002 through 2011, 144 patients undergoing minimally invasive partial nephrectomy were retrospectively reviewed by a radiologist for VFA and SQF fat measurements, using standard software. A third parameter, visceral adipose tissue percent (VAT%), was also calculated using the formula: (VAT%=[VFA/VFA+SQF]×100%). We used tertiles of VFA and SQF content to compare demographic and clinical characteristics. We also looked at VFA as a continuous variable. Associations between covariables were analyzed using multivariate logistic regression analysis and odds ratios with 95% confidence intervals.
Results:
Eighty-one patients had renal-cell carcinoma (RCC) and 30 patients had non-RCC pathology. On multivariate analysis, increasing BMI (p=0.023), VFA (p=0.048), VAT% (p=0.028), and Charlson comorbidity score (p=0.047) were significantly associated with worse preoperative Modification of Diet in Renal Disease (MDRD). In a subset multivariate analysis of the 81 patients with RCC, increasing VFA was statistically associated with worsening Fuhrman grade (p=0.017).
Conclusions:
VFA may be linked to the pathophysiology of renal function in patients evaluated for renal masses. Additionally, VFA may be associated with worsening tumor grades in patients with small-volume RCC. Interestingly, SQF did not play such a role. This small study proposes an interesting physiologic link between VFA and the biology of both kidney function and tumor histology. Larger studies are needed to corroborate our findings.
Introduction
O
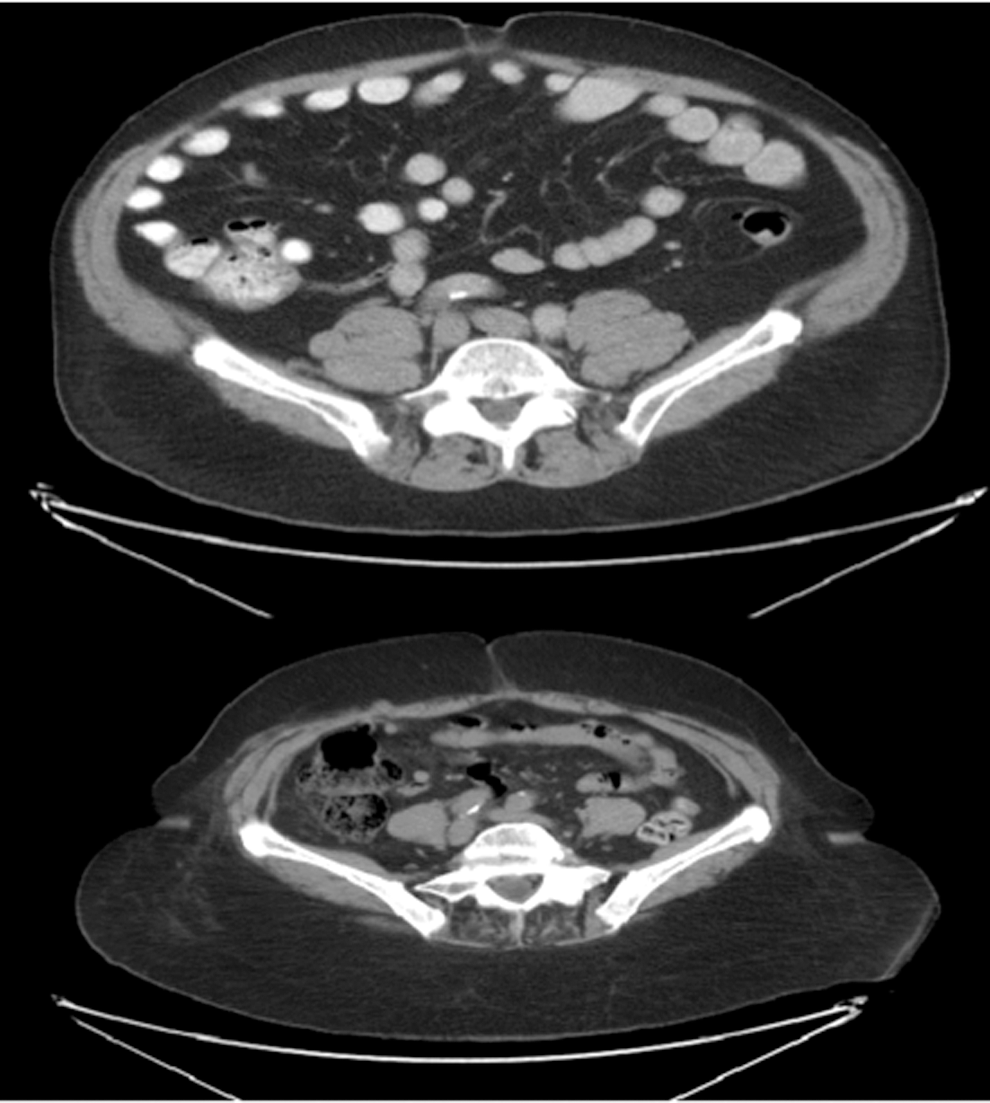
Examples of predominantly visceral obesity (upper image) and predominantly subcutaneous obesity (lower image). Both patients' body–mass index is 33.
The association between obesity and renal-cell carcinoma (RCC) has been studied. A large meta-analysis recently observed a relative risk (RR) of 1.34 and 1.24 for developing RCC in obese male and female patients, respectively. Additionally, White et al. recently demonstrated a similar but higher RR of developing RCC in those patients with a BMI of >35. 4 Such research has demonstrated that obesity is linked to RCC. However, obesity is a gross term and we feel that examining adiposity more finely, as into compartments, may lead to a more refined understanding of this association. As such, we sought to examine the association of both visceral and SQF to the Fuhrman grade and to renal function in a group of patients with small renal masses.
Materials and Methods
From 2002 through 2011, 144 patients undergoing minimally invasive (laparoscopy or robot-assisted) partial nephrectomy were retrospectively examined from an IRB-approved database generated at our institution. Preoperative CT or MRI was then reviewed by two radiologists for VFA and SQF measurements using image software on the basis of predefined Hounsfield unit thresholds (−190 to −30). Both radiologists were blinded to the clinicopathological outcomes. VFA (cm2) was measured as an anterior-posterior diameter measurement from the anterior abdominal wall to the superior mesenteric vein at the level of the uncinate process of the pancreas. SQF (cm2) was defined as the largest anterior-posterior distance from the skin surface to the anterior abdominal wall at the level of the umbilicus (Fig. 2). Visceral adipose tissue percent (VAT%) was calculated using the formula: VAT%=[VFA/VFA+SQF]×100%. 5 The utilization of a VFA ratio allowed for further comparison of fat compartments. Renal function was calculated using the Modification of Diet in Renal Disease (MDRD) equation, and we defined chronic kidney disease (CKD) stage III as a glomerular filtration rate <60.
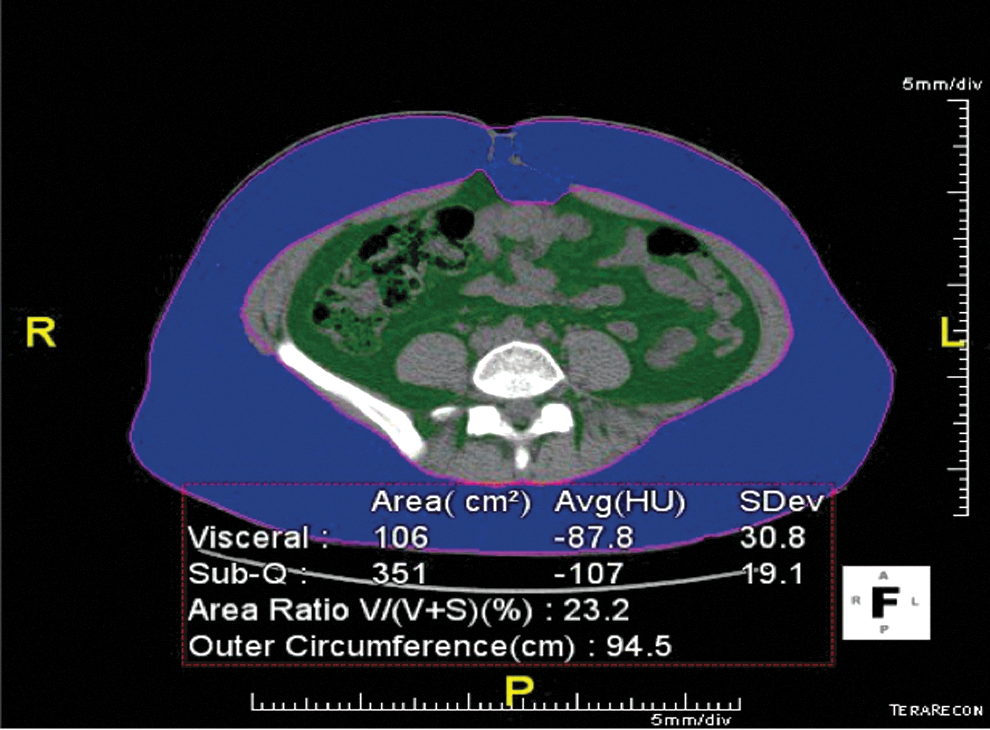
Software-generated calculation of VFA and SQF. Blue is SQF, while green represents VFA. SQF, subcutaneous fat; VFA, visceral fat.
Statistical analyses
We compared demographic and clinical data between patients, who were divided into tertiles of VFA and SQF, using one way analysis of variance models for continuous normally distributed variables and chi-square tests for categorical variables. The associations between covariables were further analyzed using multivariate logistic regression analysis and odds ratios (ORs) with 95% confidence intervals (CIs). To better define the predictive value of VFA with different variables, we constructed multivariate models to assess the chance of association over baseline variables. Variables utilized in the multivariate model included age, race, fat parameters, and a Charlson index, which corrected for baseline comorbidities. Given our small sample size, we used the validated Charlson index to evaluate for confounders rather than analyze each morbid condition separately. All statistical analyses were carried out using SPSS version 20 (Statistical Product and Service Solutions; IBM Corporation, Armonk, NY).
Results
Of the 144 patients evaluated, 19 patients did not have adequate imaging to calculate VFA/SQF and 44 patients had benign pathology. Table 1 summarizes demographic, clinical, and pathological information. Average age was 63. Fifty-seven patients (45.6%) were African-American, and 21% of the patients in our cohort had baseline CKD III. Table 2 describes patient characteristics as they relate to VFA tertiles. Patients in the highest tertile of VFA were found to have increasing BMI (p=0.001), worse postsurgical renal function (p=0.047), and a trend toward worse preoperative renal function (p=0.061) (Table 2). Specifically, 81% of patients with CKD were found to have the largest quantity of VFA.
BMI=body–mass index; cr=creatinine; IQR=interquartile range; MDRD=Modification of Diet in Renal Disease; RCC=renal-cell carcinoma; SubQ=subcutaneous; VAT%=visceral adipose tissue percent; VFA=visceral fat.
On multivariate analysis, with VFA as a continuous variable, increasing BMI (p=0.023), Charlson comorbidity score (p=0.047), VFA (p=0.048), and VAT% (p=0.028) were found to be associated with worsening baseline renal function (Table 3). On a subset multivariate analysis of the 81 patients who had RCC pathology, increasing VFA was significantly related to increasing Fuhrman grade (p=0.017), while BMI and SQF were not (Table 4). Fourteen of the 16 patients with high-grade disease (88%) were found to be in the highest tertile of VFA. VFA did not demonstrate an association with the benign renal mass. Neither SQF, VAT%, nor VFA had statistically significant relationships with tumor size, pathology, or other demographic predictors.
CI, confidence interval; OR, odds ratio.
Discussion
In this study, we demonstrated in 125 patients with T1a renal masses that VFA measurements were an independent prognostic factor for high-grade RCC and decreased renal function preoperatively. It is well documented that BMI is a risk factor for RCC. 6 Nevertheless, contrary reports exist. For example, Kamat et al. reported that increasing BMI was found to confer a more favorable prognosis in RCC patients, possibly by surrounding the tumor and preventing cancer spread. 7 In their series of 400 patients, the postsurgical disease-specific death rate was 13.6% for patients with normal BMI and 6.2% for the obese patients (p=0.011). Additionally, Steffens et al. in 2011 reported that subcutaneous adiposity was a significant predictor for longer progression-free and overall survival in patients with advanced-stage RCC. 8 In our investigation, we found that increasing VFA parameters increased the risk for high-grade tumors in RCC, while BMI and SQF did not. The contrary reports in the literature suggest that there may be complex metabolic signaling between the various fat compartments and the kidney that deserves further investigation. Additionally, the use of a global obesity measure like BMI may lead to confounders, as it is likely that the various fat compartments may each act separately in varying individuals and may not be in direct relationship to BMI.
Although no direct mechanisms have been defined in how visceral adiposity alters physiology, recent advances have improved our understanding of the relationship between VFA and carcinogenesis. 9 VFA releases high levels of adipokines, such as IL-6, VEGF, and plasminogen activator inhibitor-1, while decreasing the expression of adiponectin, a known metabolically active polypeptide secreted by adipose tissue. 10 Recently, several reports have highlighted the inverse correlation between circulating adiponectin levels and the incidence of breast, 11 colon, 12 endometrial, 13 prostate, 14 and kidney cancer. 15 In a series of 42 patients with RCC, Pinthus et al. found that low levels of adiponectins were significantly associated with a larger tumor size and risk of metastasis. 16 They additionally suggested a trend toward significance in the inverse relationship between the level of adiponectin and Fuhrman grade. In our cohort, only two patients with high-risk Fuhrman grade were found to be in the lowest tertile for VFA, while 87.5% of those with high-risk Fuhrman grade were found to be in the higher two tertiles of VFA quantity. An analysis of cytokines in such patients has been initiated.
VFA has only recently been examined in the urology literature. Zhu et al. recently reported on a series of 186 patients with surgically treated T1a RCC. 17 They found significant relationships between the percentages of visceral adipose tissue and tumor size with higher Fuhrman grades. Similar to our findings, multivariate analysis showed that the percentages of visceral adipose tissue (OR 1.06, p=0.0018) and tumor size (OR 1.91, p=0.047) were independent predictors of high-grade cancer. While the association of tumor size with Fuhrman grade has been well studied in RCC, 18 the association between VFA and Fuhrman grade is novel. Interestingly, the 186 patients evaluated in their study were all Asian, who as the authors point out, tend to have lower BMI with higher probability of visceral obesity compared with Western populations. 19 In our demographic obesity is wide spread, with the average BMI falling just under 30, and 83% of patients were defined as overweight or obese. Historically, such obesity was considered as a whole. However, these findings suggest that the various fat compartments deserve a more refined study to further elucidate the significant relationship between VFA, renal tumor biology, and renal function.
Given the obesity epidemic, it is of interest that increasing VFA was independently associated with worsening preoperative renal function such that 81% percent of those with high VFA presented with stage 3 renal disease. Of the 26 patients who had baseline CKD III, 21 fell into the higher two VFA tertiles, while only 5 of those patients resided in the lower VFA tertile. It is well established that increasing BMI is a risk factor for CKD 20 ; however, the suggestion that VFA may be the driving force behind this association is newly emerging. Although not fully defined, we believe there is a complex interplay between metabolically active visceral adipose tissue and the renal parenchyma that alters kidney physiology. Further investigation as to the exact mechanism of these relationships is warranted.
Limitations to this study include its retrospective nature and relatively small size of 125 patients. There was a possible selection bias, since all of the patients evaluated had already been treated with laparoscopic surgery and were therefore medically suitable for those interventions. Finally, our population was composed mostly of African-American and South American individuals, and our results should be validated in other ethnic groups.
Conclusion
The measurement of VFA was found to be an independent prognostic factor for Fuhrman grade and baseline kidney function, as defined by MDRD. The study of fat compartments may help focus future obesity research, as we attempt to better understand the relationships between adipose tissue and renal and tumor biology.
Further studies are needed to confirm these findings and to define the mechanism by which fat compartments communicate with the kidney.
Footnotes
Disclosure Statement
No competing financial interests exist.