
Abstract
Purpose:
To assess the impact of short-term treatment with cyproterone acetate (CPA) on intraoperative and early postoperative complications of transurethral resection of relatively large prostate.
Patients and Methods:
We recruited patients with prostate size of 60–90 g and randomized them into two equal groups. The first one had 50 mg of CPA orally twice a day (bds) for 2 weeks before the operation and maintained it for an extra week postoperatively. The other group received placebo. All patients underwent monopolar transurethral prostatectomy (M-TURP) and the prostatic chips were stained for CD34 specific for nascent blood vessels.
Results:
Ninety-five patients were included. Mean patient age was 60.88±2.5 years and mean prostate size was 72.76±7.21 g. CPA was well tolerated with no serious adverse effects. The mean resection time and the mean weight of the resected tissue were comparable between the two groups. Intraoperative blood loss, fluid absorption, and blood loss per gram of resected tissue (259.47±78.27 mL, 787.38±300.56 mL, and 14.87±4.02 mL/g and 327.25±98.97 mL, 937.4±350.2 mL, and 17.08±5.55 mL/g, respectively) were significantly lower in the treatment group (p<0.05). In addition, excessive postoperative bleeding was encountered in one case in the treatment group and in seven in the control (p<0.05). Finally, the histopathological study revealed that the mean microvessel density in each of the suburethral portion and the hyperplastic nodules of the prostate was significantly lower in the CPA group (p<0.001).
Conclusion:
The perioperative use of CPA with M-TURP of a relatively large prostate may help in decreasing the perioperative bleeding and fluid absorption that usually take place during this procedure.
Introduction
Although transurethral prostatectomy (TURP) is still considered the gold standard for operative treatment of benign prostatic hyperplasia (BPH), it is not a procedure without morbidity. Perioperative bleeding and excessive fluid absorption are usually on the top of the list of TURP complications and are directly related to the size of the gland. 1,2 On the other hand, the prostate is an androgen-dependent organ and it has been shown before that the preoperative reduction of dihydrotestosterone after finasteride administration is associated with a significant reduction in perioperative bleeding with TURP. 3,4 This effect is thought to be mediated by the reduction of androgen-dependent growth factors that is reflected into a significant decrease in angioneogensis and vascularity of the prostate. 5 –10
Cyproterone acetate (CPA) is a synthetic steroidal antiandrogen that acts mainly through competitive inhibition of androgen receptors. Also, it has some progestogenic properties that lead to suppression of gonadotrophins and thereby lowering the plasma testosterone level. CPA has the advantage of immediate effectiveness, but some side effects are described. These adverse effects include loss of libido, erectile dysfunction, and cardiovascular and hepatic toxicities. 11 CPA is usually used for androgen blockade in cases of advanced or metastatic prostate cancer. 12 In addition, it has been also used for some nononcological diseases that necessitate reduction of serum testosterone or its actions such as severe female hirsutism, hormone therapy for male-to-female transsexuals, and precocious puberty. 13 –15
In this project, we hypothesized that the perioperative blockade of testosterone that was achieved with the use of CPA might be beneficial during monopolar transurethral prostatectomy (M-TURP) of a relatively large prostate.
Patients and Methods
The study was conducted at the Tanta University Hospital between June 2011 and December 2013. The study protocol was reviewed and approved by our institutional review board, and an informed consent was obtained from all participants. We recruited 100 patients with large BPH who were scheduled for TURP. We included only cases with prostate size of 60–90 g on abdomino-pelvic ultrasonography (U/S) and with prostate-specific antigen density <0.15 ng/mL/g. We excluded patients with previous finasteride treatment, those with coagulation disorders and patients with hepatic (serum albumin <30 g/L or prothrombin activity <75%) or renal impairments (serum creatinine >1.4 mg/dL). The intake of nonsteroidal anti-inflammatory drugs was discontinued for 2 weeks preoperatively and none of our patients received subcutaneous heparin for prophylaxis. All patients were subjected to careful history taking, complete clinical examination, and routine laboratory investigations.
The selected patients were randomized through a computer-generated block randomization into two equal groups. The first group received CPA 50 mg orally twice a day (bds) for 2 weeks preoperatively and 1 week postoperatively. The second group was the placebo and both the patient and the surgeon were blinded to the drug given.
Operative technique
The procedure was carried out under spinal or general anesthesia according to the anesthesiologist and patient preferences. All operations were performed by one of the three consultants (O.M.E.-G., T.A.G., M.S.) who have good experience in TURP. In all cases, a 24F resectoscope, continuous irrigation system (Karl Storz), and monopolar diathermy were used. The irrigating fluid was 1.5% glycine to which absolute alcohol (99.5%) was added to get a 1% ethanol tagged solution. The height of the irrigation bottle was maintained at 60 cm above the level of the patient and fluid returns were collected in heparinized 10-L buckets. The hemoglobin concentration in each bucket was measured in two 4 mL samples and the mean of the two values was obtained to get the hemoglobin content in each bucket. Thereafter, the total blood loss was calculated according to the preoperative hemoglobin concentration. On the other hand, fluid absorption was evaluated by measuring the ethanol concentration in the patients' exhaled breath with breathalyzer (Lion Alcolmeter 500®; Lion Laboratories Ltd.) before and every 10 minutes throughout the procedure. 16
At the end of surgery, a 22F urethral catheter was inserted and the bladder was irrigated with physiologic saline. The catheter was removed when the wash had been cleared. Thereafter, the patient was asked for a trial of voiding. If he was able to void satisfactorily with not much residual urine (<100 mL by abdominal U/S), we discharged him. Otherwise, the catheter was reinserted for another 3 days.
Following surgery, the TURP chips were weighed on an electronic scale and subjected to histopathological examination. In addition, liver function tests and complete blood count were repeated for all patients at the end of their treatment (1 week after surgery). The toxicity for CPA was graded according to the National Cancer Institute Common Terminology Criteria for Adverse Events v4.0 (CTCAE).
Histological and immunohistochemical testing
Surgical specimens were classified according to their sites in the prostate:
Site (1): Prostatic suburethral tissue (superficial cuts).
Site (2): Prostatic hyperplastic nodules (deep cuts).
These prostatic chips were examined with routine hematoxylin and eosin staining and also subjected to monoclonal immunohistochemical antibody to CD-34 antigen. This antigen is an endothelial cell antigen specific for nascent blood vessels and it has been established as an effective immunohistochemical marker for prostatic microvessel density (MVD) analysis. 17 MVD was determined by counting positively stained blood vessels in 10 consecutive nonoverlapping fields within a 10×10 reticulated imprinted grid at 400× magnification.
All the histopathological studies were carried out by a single blinded examiner.
Statistical analysis
Data were collected and analyzed by the Student t test or the Pearson chi-square test, as appropriate, with p<0.05 considered statistically significant. These tests were done by the computer software SPSS 17.0 for Windows®.
Results
A total of 100 patients were included. The histopathological examination of the TURP chips revealed adenocarcinoma of the prostate in three cases of the CPA group and in two patients of the control. These five patients were excluded from the study. Mean patient age was 60.88±2.5 years and the mean prostate size was 72.76±7.2 g with no significant difference between the two groups. The other preoperative parameters in the two groups were also comparable (Table 1). CPA was well tolerated by all cases with no major side effects and none of the participants had discontinued it. Five patients reported only some upper gastrointestinal upset in the form of mild nausea (grade 1-CTCAE) and mild vomiting (grade 1) and two cases had pruritus (grade 1).
Preoperative Data in Both Groups
CPA=cyproterone acetate; IPSS=International Prostate Symptom Score; HCT=hematocrit; PSA=prostate specific antigen.
The operation was performed under spinal anesthesia in all cases except for eight patients in the CPA group and six in the control group according to the anesthesiologist and patient preferences (p=0.575) (Table 2). The mean resection time and the mean weight of the resected tissues were 51.75±9.78 min and 29.85±4.6 g in the CPA group. The corresponding figures in the control group were 52.54±5.99 minutes and 28.02±5.54 g with no significant difference between the two groups (p=0.632, 0.08, respectively) (Table 2). On the other hand, intraoperative blood loss was significantly lower in the CPA group (259.47±78.27 mL) compared to the control (327.25±98.97 mL, p<0.001) (Table 2). Meanwhile, the calculated blood loss for each gram of the resection weight was also significantly lower in the treatment group (p=0.029 <0.05, Table 2) However, there was no need for intraoperative blood transfusion during the procedure in both groups. The fluid absorption during resection was also significantly higher in the control group (787.38±300.56 v 937.4±350.2 p=0.028 <0.05) (Table 2).
Operative Data in Both Groups
In the early postoperative period (before catheter removal), excessive bleeding was encountered in four cases in the control group. These patients received 1–2 U of blood to compensate this bleeding. After removal of the catheter, all patients were able to void satisfactorily except for four cases in the treatment group and six patients in the control group. These 10 patients were managed by reinsertion of the catheter for three days. Thereafter, all of them had a good voiding with no significant residual urine (<100 mL).
In addition, there were four patients (one in the CPA group and the rest in the control) who were readmitted in the first month after discharge because of clot retention or gross hematuria. Therefore, the total number of cases with postoperative bleeding was found to be one patient in the treatment group and seven cases in the control and the difference between the two groups was found to be statistically significant (p=0.032).
Immunohistochemistry and MVD analysis
The histopathological examination of the TURP chips revealed that the MVD in the suburethral portion of the prostate was significantly lower in patients treated with CPA compared to control (3.89±1.17 v 13.67±1.39 vessels per high-power field) (p<0.001). Meanwhile, a significant decrease in the MVD in the nodular adenomatous portion was also reported in the CPA group. In the treatment group, the mean MVD in the hyperplastic nodules was 5.89±1.17 per high-power field and the corresponding figures in the control were 16.35±1.44 (p<0.001) (Table 3; Figs. 1 and 2).
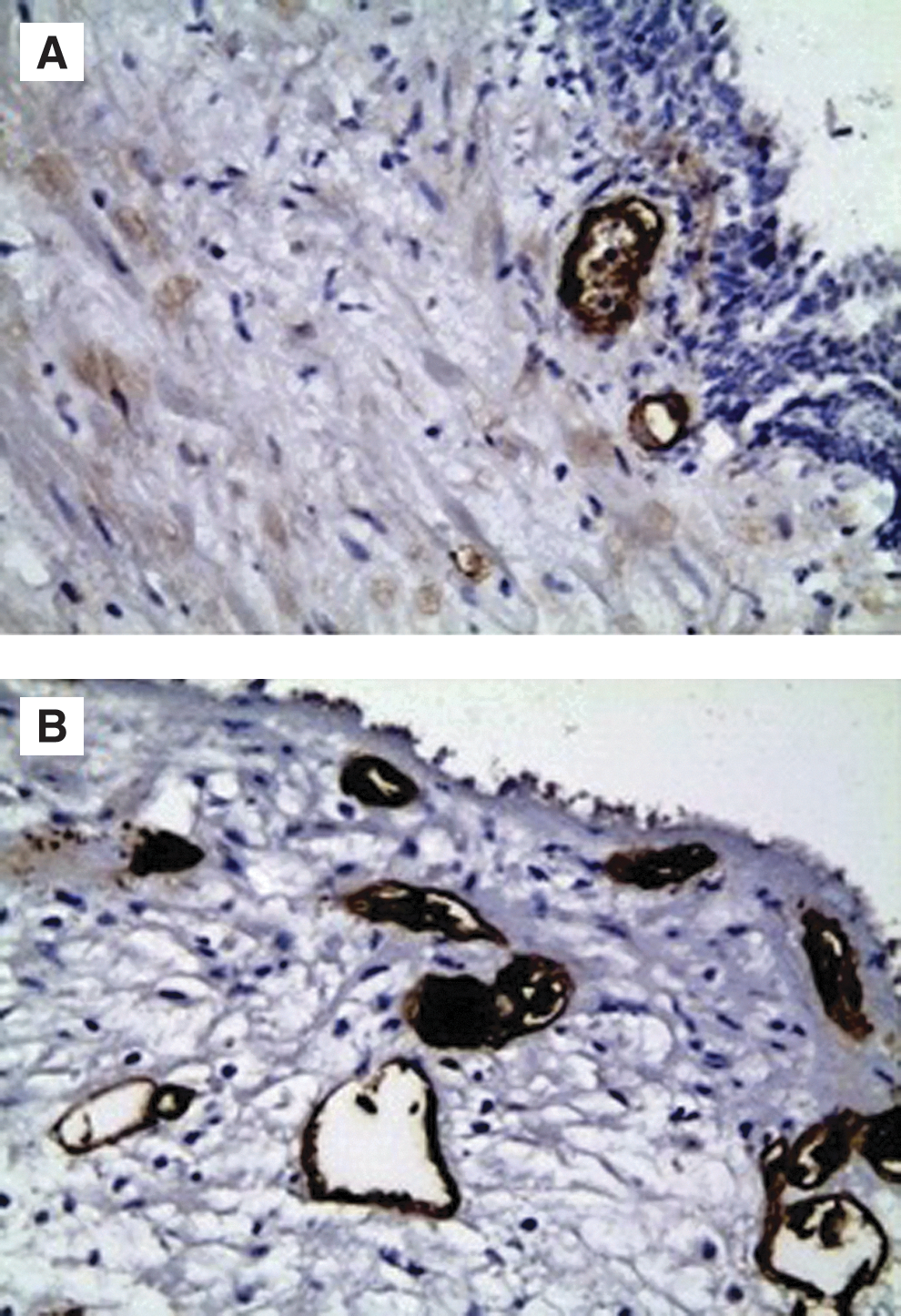
CD-34 staining of the suburethral prostatic tissue showing marked reduction of MVD in the CPA group

CD-34 staining of the hyperplastic nodules showing marked reduction of MVD in the CPA group
Microvessel Density Analysis for Both Groups
Discussion
Perioperative bleeding and excessive fluid absorption are inherent complications of TURP. These complications are related directly to the size of the gland. 1,2,18 Given that patients with small prostate are not at a great risk of these complications, we preferred to not include them in this trial. In addition, we also excluded patients with prostate cancer to have a homogenous sample in this project. In the current series, CPA was well tolerated by all patients with no major adverse effects. This can be attributed to the low dose and the short duration of its administration, as well as the normal liver functions of our patients. This observation was found to be in agreement with that reported by other authors who used CPA for nononcological causes. 13 –15
It has been shown before that prostate regression after androgen deprivation is secondary to regression of the prostate vascular system that leads to cell death due to tissue ischemia or hypoxia. 19 The previous studies also demonstrated that castration results in a rapid and significant reduction of blood flow to the rat ventral prostate and this was found to coincide with the appearance of degenerative changes in the prostatic endothelial cells. 20 –22 Additionally, the beneficial effect of finasteride in the treatment of hematuria associated with BPH has also suggested the inhibitory action of androgen deprivation on prostatic vasculature. 23 –26 This action was confirmed histologically by the significant decrease in the prostatic suburethral MVD that was reported after the use of finasteride. 8 –10 On the other hand, there is some evidence in the literature that androgens can control the vascularity of the prostate through regulation of the different growth factors such as basic fibroblast growth factor, vascular endothelial growth factor, and epidermal growth factor. 5 –7,27
The immunohistochemical examination in our project demonstrated that the MVD is significantly reduced after CPA in both the suburethral part and the hyperplastic nodules of the gland. Nevertheless, the previous trials showed that finasteride can reduce the MVD in the suburethral part only and it has no effect on hyperplastic nodules. 8 –10 This discrepancy between CPA and finasteride in this regard could be attributed to the more inhibitory action of the former.
In the current study, we reported that the intraoperative bleeding was significantly reduced after the use of CPA. A similar finding was also described when finasteride was used before TURP. 3,4 However, patients with small prostate were not excluded in all the finasteride trials. On the other hand, because intraoperative bleeding in this operation is closely related to the resection weight, we have calculated the blood loss per gram tissue resected and compared it between the two groups. This comparison revealed a significant decrease in this parameter in the CPA group. Similarly, Ozdal et al. have shown a comparable finding after the preoperative use of finasteride for 4 weeks. 4
Systemic absorption of the irrigating fluid always takes place in TURP and it is usually increased with the increase in blood loss and resection time. The previous studies showed that a large scale of fluid absorption (1–1.5 L) was reported in 5%–10% of cases. 28,29 In this study, we demonstrated that fluid absorption is significantly reduced after the use of CPA. On the other hand, when finasteride was used for three months before TURP, Sandfeldt et al. showed no significant decrease in this parameter, but the proportion of patients with high fluid absorption was reduced. 30
In the literature, excessive postoperative bleeding and clot retention are reported in 3.9% and 3.3% after TURP and they are related directly to the prostate size and the resection weight. 2 In our series, the incidence of these complications in the control group was 8.3% and 6.3%, respectively. This high rate is attributed to our selection criteria that involved only patients with large prostate. Similarly, in a study by Hagerty et al., there were 19 patients with a resection weight of 30 g or more and seven of them (36.8%) developed perioperative bleeding. 18 On the other hand, with the use of CPA in our project, a significant reduction of these complications was observed. These results are in accordance to those of Hagerty et al. and Ozdal et al. who used finasteride before surgery. 4,18
It is noteworthy to mention that none of the previous trials that used finasteride before TURP maintained it after surgery. However, in our trial, we maintained CPA for an extra week postoperatively to get the beneficial effects of its action in this critical period as well. Nevertheless, we are not sure about the time interval that is needed for the microvessels of the prostate to return to its normal level after cessation of CPA. This piece of information could be crucial in determining the optimum postoperative period of CPA after this surgery.
Finally, we have to admit that the resection of large prostate usually necessitates a surgeon with good experience in this task because intraoperative bleeding can make it a relatively difficult procedure. Therefore, the reduction of operative bleeding and the clear operative field after the use of CPA may make the resection of large gland more easier specially for the less experienced surgeons, but more studies are needed to confirm this idea. On the other hand, the decrease in intraoperative bleeding and fluid absorption after the use of CPA can be of outmost importance in cardiac or critically ill patients. The main limitation of this study is the relatively small number of patients and indeed a randomized trial with finasteride is warranted before the final conclusion. In addition, more studies are needed to determine the optimum dose and duration for the use of CPA in this procedure. Furthermore, if the future studies confirmed the safety and efficacy of CPA in this operation, it could be tried in lager prostates (>90 g) and this might be helped with the use of bipolar diathermy.
Conclusion
The perioperative use of CPA in M-TURP of moderately enlarged prostate is well tolerated in the properly selected patients and it can help in decreasing the perioperative bleeding and fluid absorption during this surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.