
Abstract
Introduction and Objective:
Since the introduction of robotic surgery for radical prostatectomy, the cost–benefit of this technology has been under scrutiny. While robotic surgery professes to offer multiple advantages, including reduced blood loss, reduced length of stay, and expedient recovery, the associated costs tend to be significantly higher, secondary to the fixed cost of the robot as well as the variable costs associated with instrumentation. This study provides a simple framework for the careful consideration of costs during the selection of equipment and materials.
Materials and Methods:
Two experienced robotic surgeons at our institution as well as several at other institutions were queried about their preferred instrument usage for robot-assisted prostatectomy. Costs of instruments and materials were obtained and clustered by type and price. A minimal set of instruments was identified and compared against alternative instrumentation. A retrospective review of 125 patients who underwent robotically assisted laparoscopic prostatectomy for prostate cancer at our institution was performed to compare estimated blood loss (EBL), operative times, and intraoperative complications for both surgeons. Our surgeons now conceptualize instrument costs as proportional changes to the cost of the baseline minimal combination.
Results:
Robotic costs at our institution were reduced by eliminating an energy source like the Ligasure or vessel sealer, exploiting instrument versatility, and utilizing inexpensive tools such as Hem-o-lok clips. Such modifications reduced surgeon 1's cost of instrumentation to ∼40% less compared with surgeon 2 and up to 32% less than instrumentation used by surgeons at other institutions. Surgeon 1's combination may not be optimal for all robotic surgeons; however, it establishes a minimally viable toolbox for our institution through a rudimentary cost analysis. A similar analysis may aid others in better conceptualizing long-term costs not as nominal, often unwieldy prices, but as percent changes in spending. With regard to intraoperative outcomes, the use of a minimally viable toolbox did not result in increased EBL, operative time, or intraoperative complications.
Conclusion:
Simple changes to surgeon preference and creative utilization of instruments can eliminate 40% of costs incurred on robotic instruments alone. Moreover, EBL, operative times, and intraoperative complications are not compromised as a result of cost reduction. Our process of identifying such improvements is straightforward and may be replicated by other robotic surgeons. Further prospective multicenter trials should be initiated to assess other methods of cost reduction.
Introduction
F
Analysis of outcomes has shown reduced hospital stays, reduced blood loss, comparable postsurgical margin rates, and higher survival in experienced hands as compared to past laparoscopic or open procedures. 4,6 –9 Given such patient safety, wide physician acceptance, a yearly influx of almost 240,000 new prostate cancer diagnoses, 10 and recent trends toward direct-to-consumer advertising, 11 the demand for RALP will likely continue to rise. As such, reigning in procedural cost becomes an increasingly important consideration.
At a fixed cost of $1 to 2.5 million per da Vinci system 3,12 and a variable cost per procedure estimated to range between $2000 and $40,000, a complete substitution of conventional surgery by robotics would bloat national health spending by an estimated $2.5 billion annually. 3 Furthermore, although many industries witness falling prices as new technologies age, it is so far unclear whether the da Vinci surgical system will follow suit, or at what rate, given its lack of and high regulatory barriers to competition—qualities that dampen such cost reduction. 13 Eventually, competing and novel robotic surgery platforms will arrive and likely lead to reduced costs. 7,14 Until then, procedural changes can be made to improve cost effectiveness.
Specifically, operating room (OR) supplies have been identified in the literature as primary cost drivers. 15,16 As such, our institution aimed to not only eliminate unused equipment but to also replace unnecessary equipment with more cost-effective alternatives. This article summarizes our approach to considering instrumentation costs, not to validate any specific set of instruments but to share with surgeons a novel way of thinking about the costs of their preference cards.
Materials and Methods
We studied improved surgical material selection as one possible method of cost reduction. Two experienced robotic surgeons at our institution were queried about their preferred instrument usage for RALP. Surgical supply preference cards were compared and an exhaustive list of supplies enumerated. Costs of instruments and all materials were obtained from various internet retailers, tabulated, and sorted to identify prominent cost drivers (Fig. 1 and Supplementary Table 1). Finally, high-volume surgeons at three other institutions were consulted to explore possible and novel combinations of surgical supplies, and a minimally viable toolbox was identified. This minimally viable toolbox represents the bare essential combination of RALP instruments and it minimizes the set of recognized cost drivers by eliminating or replacing underutilized equipment with the highest impact to cost. The total price of our minimally viable toolbox—consisting, in our case, of monopolar shears, a prograsp, a fenestrated bipolar, one needle driver, and Hem-o-lok clips—was then compared to more conventional alternatives and relative cost improvements were calculated.
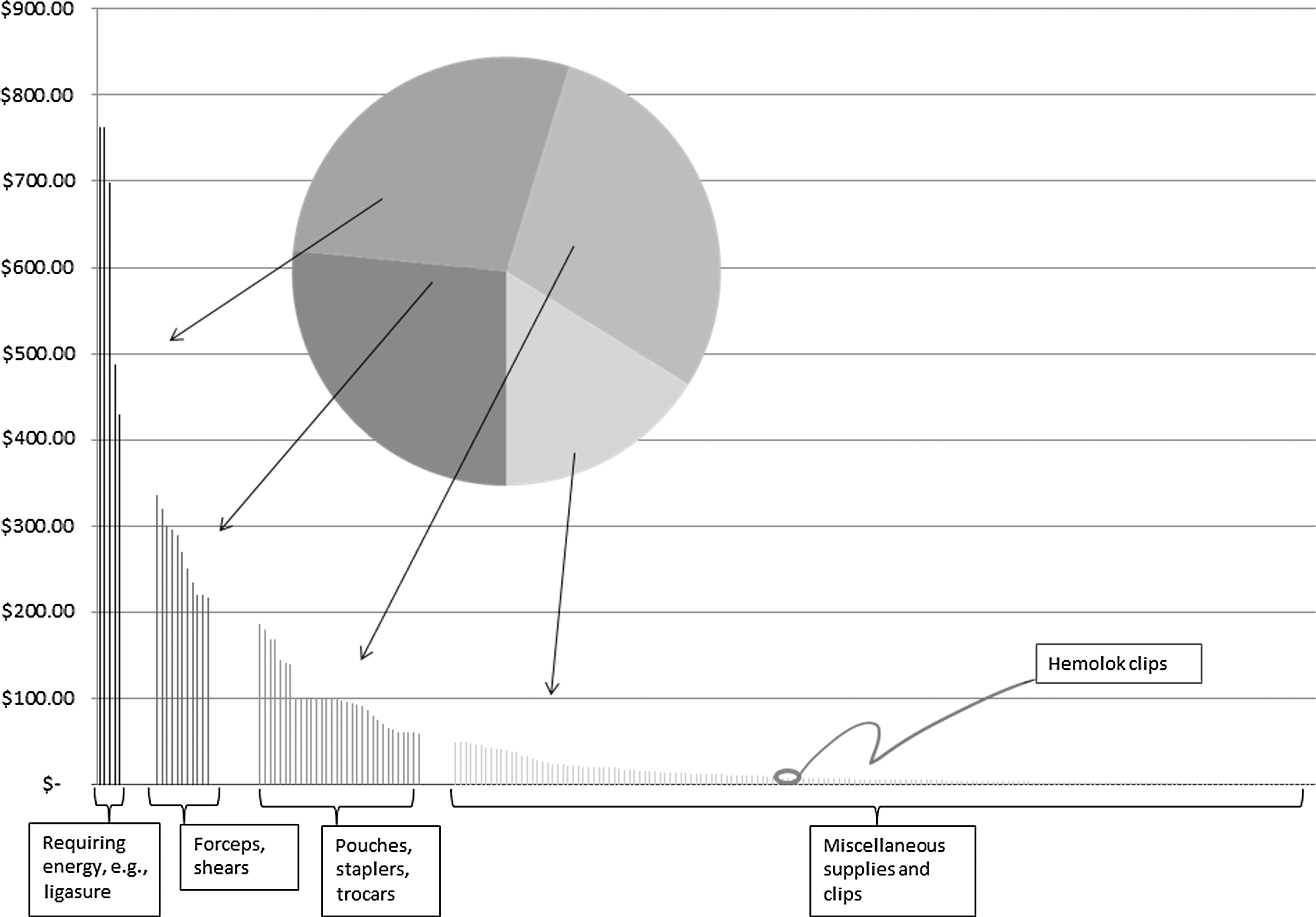
The bar graph ranks 20-month supply prices per use, divided into four categories and compared by proportion of spending in the overlying pie chart.
Thereafter, our surgeons have been encouraged to consider the minimally viable toolbox as a baseline for selecting instruments, keeping in mind the percent change in cost due to various choices. Our institution-specific pricing data are restricted, but online retailer pricing serves effectively as a frame of reference for calculating these proportional changes. Of course, retail data should be substituted, when possible, by any specific cost schedule being analyzed.
We performed a retrospective review of 125 patients who underwent RALP for prostate cancer from January 2012 to August 2013 by these two surgeons. We compared estimated blood loss (EBL), operative times, and intraoperative complications.
Results
The two surgeons queried for material utilization each performed 64 and 61 RALP procedures in the 20-month period. Their use of surgical supplies is summarized in Figure 1. Four categories of supplies emerge: (1) energy-requiring vessel sealing instruments, comprising 28% of expenditures, (2) forceps and shears instruments, making up 27% of spending, and (3) expensive and (4) inexpensive miscellaneous equipment, comprising 29% and 16% of spending, respectively. Miscellaneous equipment consists of sutures, clips, draping, various trocars and specimen pouches, as well as other items whose use varies by procedure and may be difficult to predict. The two most expensive (by item) categories consisting of far fewer, more predictably, and consistently used items—for example, Ligasure, monopolar shears, and needle drivers—together make up 55% of OR supply expenditures. Hence, we predicted that it would be easier to find savings by streamlining these two top-priced categories.
Both surgeons use monopolar shears and a prograsp. In addition to these instruments, surgeon 1 utilizes a fenestrated bipolar doubling as a forceps grasper and thus he uses only one needle driver. Surgeon 1 does not use an energy source (e.g., Ligasure or vessel sealer) and instead utilizes Hem-o-lok clips. Thus, surgeon 1 utilizes what we have dubbed as the minimally viable toolbox for RALP. Alternatively, surgeon 2 utilizes two needle drivers and either a fenestrated bipolar or PK® dissector. In addition to this, surgeon 2 also uses a Ligasure that is operated by a bedside assistant.
As a result of the above modifications, the cost of the minimally viable toolbox was ∼40% less than the second surgeon's. The largest cost savings are through the elimination of an energy source and the usage of Hem-o-lok clips, which are inexpensive, retailing nearly 2 dollars each (Figs. 1 and 2). An energy source accounts for 25% to 30% of the cost of total robotic instruments. Utilizing the fenestrated bipolar as forceps can eliminate the need for a second needle driver, saving 12.5% of total instrument costs for surgeon 2. There is no significant cost saving when utilizing the bipolar over the PK® dissector (1.2%).

The minimally viable toolbox uses no Ligasure and one needle driver leading to a 40% cost reduction compared to instrumentation combinations within our institution.
In assembling our minimally viable toolbox, surgeons at three other institutions were consulted, and some of their preferred instrumentation is compared in Figure 3. Again, sacrificing a needle driver and making do with as few instruments as possible accounts for significant savings, ranging between 16% and 32%.
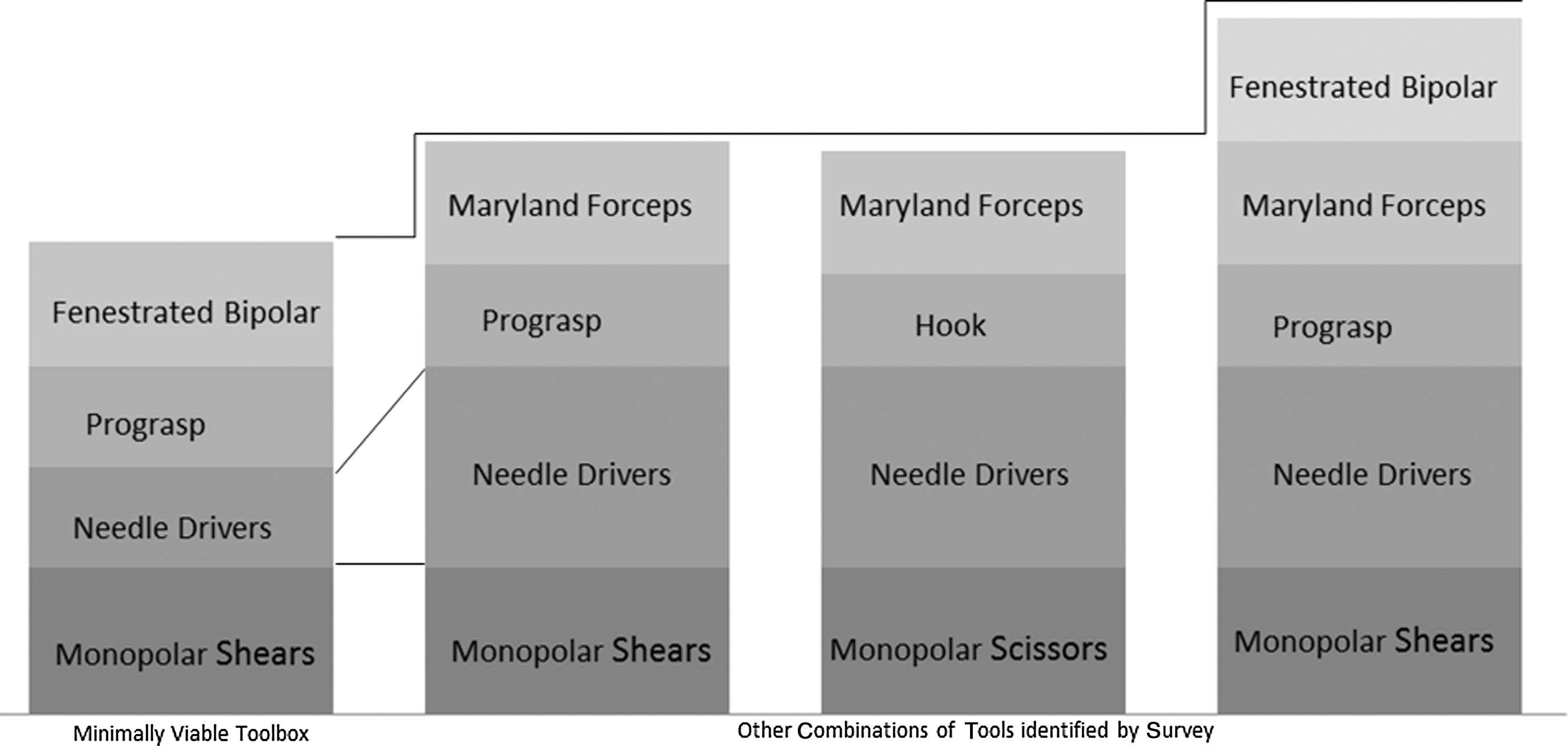
Left to right: surgeons from other institutions would save 18%, 16%, and 32% if using our minimally viable toolbox; identifying one's own minimally viable toolbox may yield similar savings.
In addition to promising cost reductions, our records indicate a potential improvement in both average blood loss (148 vs. 265 mL; p=0.045) and operative time (132 vs. 158 minutes; p=0.001) associated with our adoption of the minimally viable toolbox and an overall absence of intraoperative complications in the 20-month period.
Discussion
Robotic surgery is becoming more widely used for prostatectomy. 17,18 The benefits of minimally invasive surgery—including decreased operative time, blood loss, length of hospital stay, and postoperative pain—have overcome the choice of open prostatectomy, 19,20 however, the costs incurred by robotic surgery can be overwhelmingly expensive compared to open or pure laparoscopic prostatectomy. 21 –23
Several studies have attempted to identify and understand the predominant drivers of robotic surgery costs. Rebuck et al. reported that direct costs (surgical supplies, OR time, room, hospital stay) of robotic surgery are significant. 16 Tomaszewski et al. compared the cost of open versus RALP among four experienced surgeons in one institution. They reported that robotic surgery was more expensive than the traditional method. They demonstrated that cost differences were rooted in OR supplies and indirect costs, such as the purchase and maintenance of the robot. 15
A study by Bolenz et al. aimed to predict factors responsible for direct costs associated with RALP using preoperative, intraoperative, and postoperative variables. They demonstrated that higher costs are driven by events occurring during the procedure (increased OR time and use of a pelvic drain) or by those occurring postoperatively (transfusion, complications, and length of hospital stay). Thus, although many of these higher costs could not be predicted preoperatively, the authors hypothesized that RALP cost reduction may be achieved by decreasing operative times and complications. 24
Other studies have tried to minimize costs of robotic surgery. Rebuck 16 also found significant improvements in both cost and time by using a dedicated nursing and anesthesia team familiar with RALP, scheduling tasks in parallel (e.g., opening equipment while bringing the patient into the OR instead of in series), setting time goals for trainees for each step of surgery, and by eliminating unused supplies—that is, an extra needle driver, an extra stapler, and unused irrigation fluid. They reported a cost reduction of 28%. 16 In fact, other studies have identified surgical instruments as primary RALP cost drivers ripe for reductions. 7,25,26
Similarly, we attempted to improve our conceptualization of costs, which we hope will translate to sustained cost reductions. We surveyed two surgeons at our institution to better understand the minimum instruments required to effectively perform RALP. We report a simple method of identifying an institution's instrumentation cost drivers and establishing a minimally viable toolbox of instruments for performing the procedure. This toolbox can then be compared to more traditional combinations of instruments. Notably, our analysis relies, in part, on the gathering of retail price information because medical supply price negotiations are contractually sealed and unpublishable at our institution. Nonetheless, assuming similar retail markups on all supplies, an analysis that compares product prices proportionally would not change at a different scale—that is, 40% calculated savings would still be 40%, regardless of the nominal price. Undoubtedly, however, any use of this analysis procedure would be greatly improved with access to exact prices, avoiding such assumptions.
To summarize, our analysis led us to eliminate a second needle driver with a fenestrated bipolar used in its place, reducing overall equipment costs, and, possibly, OR time. The fenestrated bipolar is able to both cauterize and grasp, thus theoretically reducing the time required for multiple instrument exchanges when hemostasis is desired. Further observations would, however, need to be carried out to determine if this is, in fact, the case. Furthermore, obtaining hemostasis with inexpensive yet effective Hem-o-lok clips virtually eliminates the cost of an extra hemostatic instrument.
Of course, these specific changes may not be readily adoptable by all surgeons, but the process of identifying a comfortable minimum instrumentation can provide surgeons with an easy and effective method of viewing their instruments as proportional expenditures, rather than as any specific dollar value without the context of a baseline minimal instrumentation. Again, our specific adjustments may not suit all surgeons who should use our analysis to guide only their perceptions of cost, still considering other variables vital to selecting instruments: operative time, complications, blood loss, etc.
Our study did not aim to validate our own minimally viable toolbox in this context, but nonetheless analyzed these factors. Blood loss and operative time were sampled by convenience, and an independent sample t-test was used to compare means in these metrics. Interestingly, surgeon 1, using the minimally viable toolbox, had a statistically significant improvement in both blood loss (148 vs. 265 mL; p=0.045) and operative time (132 vs. 158 minutes; p=0.001) over surgeon 2. Surgeon 1 did not have any intraoperative complications, while surgeon 2 reported one rectal enterotomy that was simply repaired. Such results, however, again only aim to report a cognizance of costs: reporting of blood loss is subjective and operating time may depend more on the surgeon and bedside assistance than on tools. Factors for intraoperative complications can be multifactorial, including difficulty of the case, patient anatomy, and surgeon and assistant skill.
Moreover, our study is by no means a well-controlled randomized experiment. Nonetheless, our results demonstrate that supply costs may be reconsidered and contained without compromising important metrics of efficiency and patient safety. Future studies should be undertaken to include such variables in the process for choosing a minimally viable toolbox or to ever validate a universal one. Still, surgeons seeking to establish their own minimally viable toolbox should take these variables into consideration.
Instrumentation is only one aspect of robotic prostatectomy cost. In a review, Bolenz concluded that, over all, RALP has not been shown to be cost effective in the perioperative period, however, long-term follow-up should consider the cost of future derivative procedures (salvage therapy, stricture dilations, procedures for incontinence and erectile dysfunction), which may significantly impact a true assessment of costs. 27 Until long-term data for oncologic, continent, and potency outcomes of robotic surgery demonstrate superiority over conventional prostatectomy, it may be difficult to economically justify the use of robotics. Furthermore, even if RALP costs could be reduced, passage of savings to patients and in what ratio could not be guaranteed. 15 Nonetheless, Steinberg et al. postulate that a significant increase in caseloads can be profitable for high-volume nonacademic (no residents or fellows) institutions. 28 One can hope that the patient will eventually share in the benefits of said profitability. Despite such uncertainty, RALP continues to gain favor and is likely to remain a staple for prostatectomy and, as such, cost reduction should continue to be explored, particularly on an individual level.
Conclusion
Robotic surgery costs can be minimized by identifying a minimally viable toolbox of instruments, eliminating the use of an energy source like the Ligasure or vessel sealer, and utilizing an inexpensive tool such as Hem-o-lok clips. Additionally, the use of the fenestrated bipolar as forceps eliminates the need for a second needle driver. These changes can reduce costs incurred on robotic instruments alone by 40% or greater. Moreover, EBL, operative times, and intraoperative complications were not compromised as a result of cost reduction. Further prospective multicenter trials should be initiated to assess other methods of cost reduction. Although such changes may not be suitable to all surgeons, our straightforward process of identifying a minimally viable toolbox allows one to view costs not as nominal prices but as proportional deviations from a baseline. Thus, one can more fluidly remain cognizant of long-term costs before they accumulate.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.