
Abstract
Purpose:
To report our initial results of robotic appendicovesicostomy (APV) revision in children.
Patients and Methods:
Three patients (median age 6 years; range 6–13) underwent robot-assisted APV surgery for bladder dysfunction because of posterior urethral valves, myelomeningocele, and traumatic spinal cord transection. Leakage developed in each patient from the APV. After failing more conservative treatments, the patients subsequently underwent robot-assisted APV revision.
Results:
Robot-assisted APV revision was conducted at a median 14 months (range 6–34 mos) after initial surgery. Median operative time was 165 minutes (range 106–232 min), and blood loss was ≤5 mL for all patients. Intraoperative findings ranged from partial to complete separation of the APV from the bladder tunnel. APV leakage resolved for all patients at last follow-up (median 5 months; range 2–9 mos).
Conclusion:
This initial series expands the scope of robotic surgical procedures in children. Robot-assisted APV revision was technically feasible and safe in this early experience.
Introduction
T
As the prevalence of robot-assisted operations increases, its application to reoperative surgical procedures will also evolve and prompt evaluation of safety and efficacy. 9 Lindgren and associates 12 reported a series of 16 children with failed previous pyeloplasty (12 open and 4 robotic) and underwent robotic reoperative repair (13 redo-pyeloplasty and 3 ureterocalicostomy). 12 The authors concluded that robot-assisted surgical procedures were safe and effective in salvage repair.
We present our technique and short-term results for children who underwent robot-assisted APV revision.
Technique
Patient positioning
The patient was placed supine, and all potential pressure points were meticulously padded. After adequate general anesthesia was induced and the proper timeout procedure was followed, the patient was prepped and draped in standard surgical fashion.
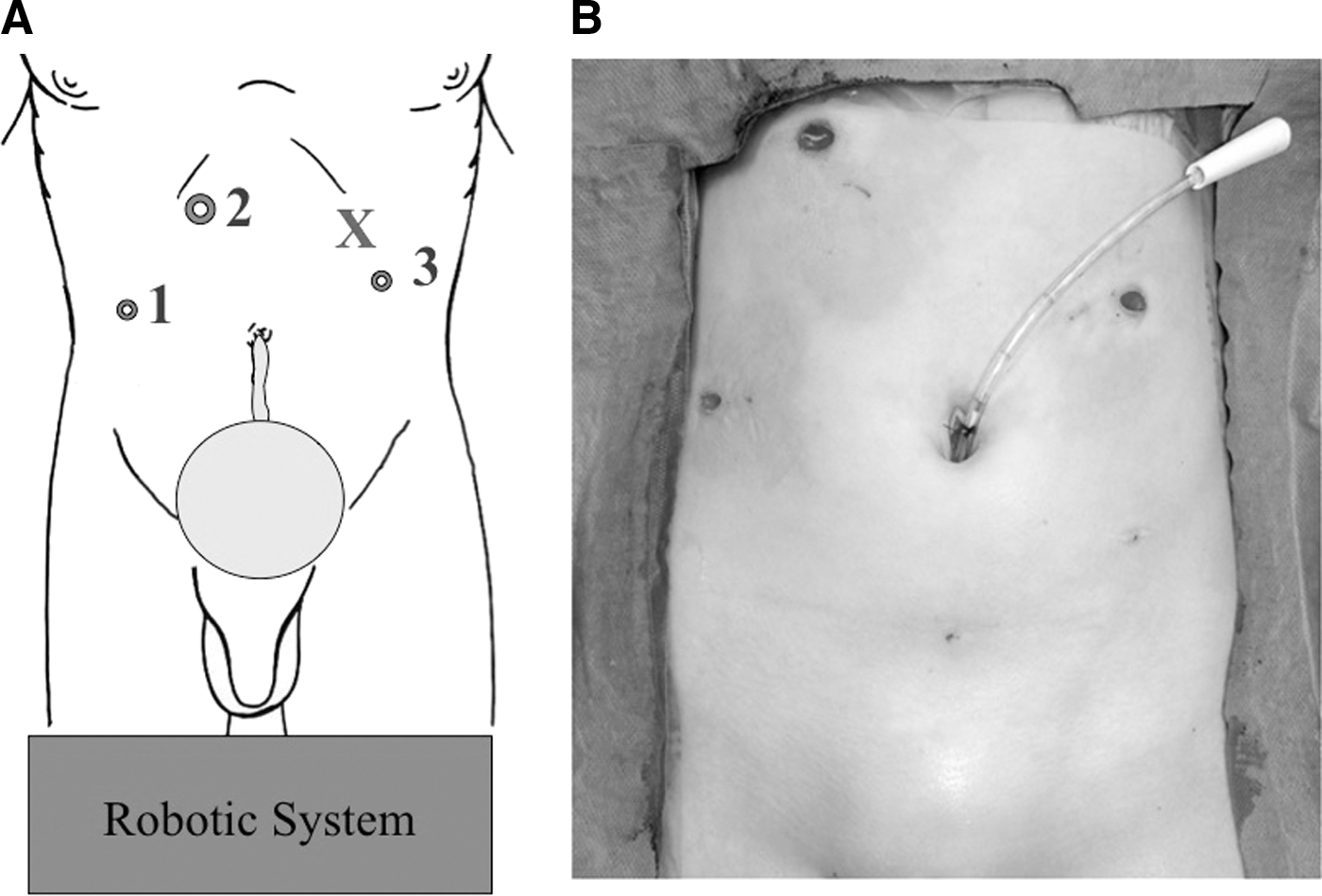
Port placement
The Hassan technique was used to place a 12-mm trocar for the camera in the right upper quadrant (Fig. 1). After insufflation of the abdomen, working trocars of 8 mm were placed under direct vision in the right and left midclavicular lines, superior to the APV. A 5-mm assistant port was used in the left subcostal area between the left working trocar and the camera port. The working ports were secured to the patient's skin using Steri-Strips™ and Tegaderm™ (3M Health Care, St. Paul, MN). Once all ports were secured, the robot (da Vinci Surgical System, Intuitive Surgical, Inc., Sunnyvale, CA) was docked at the foot of the bed.
(
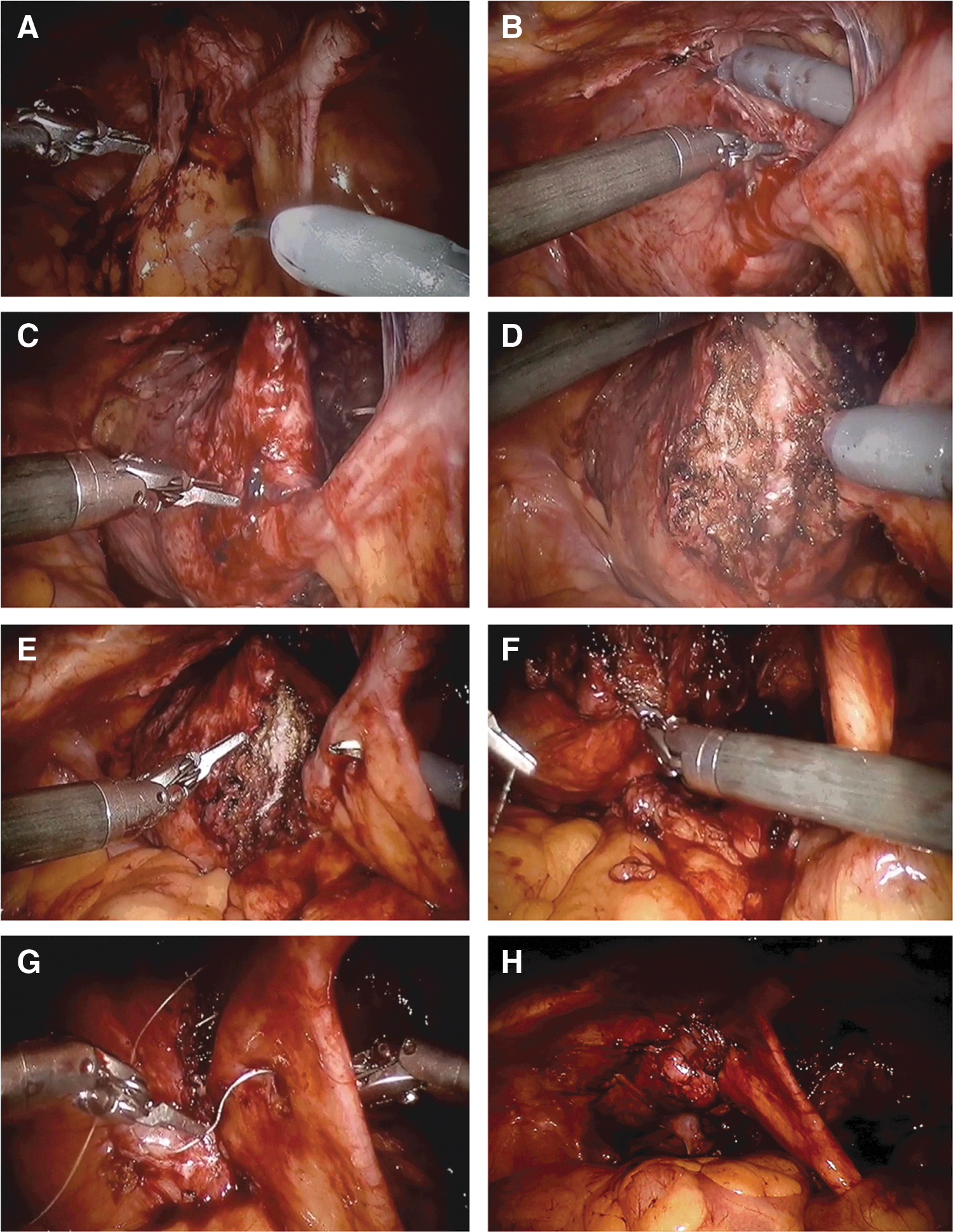
Dissection of the APV
Initial intra-abdominal findings ranged from partial to complete separation of the APV support from the posterior bladder tunnel and anterior abdominal wall; however, the APV was never completely distracted from the bladder or skin anastomoses. A 12F Mentor catheter (Coloplast, Minneapolis, MN) was placed into the APV to drain the bladder and to provide backing to the APV during dissection. Placement of the catheter also confirmed patency of the APV and ruled out any structured portions. The APV was isolated and dissected away from the remaining bladder tunnel and attachments (Fig. 2). The anterior bladder was then dissected away from the abdominal wall to allow for sufficient length of APV tunneling. The bladder was hitched to the anterior abdominal wall with 3-0 polydioxanone suture to allow the bladder to assume an elongated, vertical shape to facilitate with creation of the new APV tunnel in a tension-free manner.
(
Tunneling of the APV
Detrusororraphy using monopolar electrocautery was performed lateral to the APV on both sides. It was extended to the anterior bladder to allow for sufficient tunnel length (3–5 cm). To create the tunnel, the detrusor was wrapped over the APV using 3-0 V-Loc™ (Covidien, Mansfield, MA) suture in running fashion. A hole was created in the mesentery to allow for passage of the suture and to facilitate tunneling in this intermediary area. Once the APV was adequately covered, the bladder was filled, and the APV was tested for leakage and integrity. The mesentery has proved to be durable and resilient during redo operations, which we attribute to appropriate mesentery selection during primary surgery and delicate handling during revision surgery. We endorse limited tissue handling of the APV and recommend manipulating the mesentery without directly grasping it and aggressively adjusting camera angles to see around it.
Closure
The peritoneal defects were closed with running 4-0 V-Loc™ suture. The Mentor catheter was secured in place with a 3-0 nylon suture. The fascia was closed with 2-0 polyglactin and the skin with 5-0 polyglecaprone sutures. Dry sterile dressings were applied.
A video demonstrating this technique is available at
Postoperative care
Patients were admitted postoperatively and discharged once a regular diet was tolerated and pain was controlled. Patients were discharged home with the Mentor catheter in place and receiving anticholinergic therapy unless intolerant. Patients returned for indwelling APV catheter removal and teaching 3 weeks postoperatively.
Equipment
• da Vinci Surgical System
• 12 mm (1), 8 mm (2), and 5 mm (1) trocars
• Steri-Strips and Tegaderm
• 12F Mentor catheter 3-0
• 4-0 V-Loc suture
• Open surgical set
Role in Urologic Practice
Results
Leakage from the APV developed in three patients (mean age 8 years; range 6–13) who underwent robot-assisted APV. Each patient failed conservative treatments, which included intermittent catheterization, anticholinergics, bladder botulinum toxin injection, and APV dextranomer/hyaluronic acid injection (Deflux®, Salix Pharmaceuticals Inc., Raleigh, NC). The patients subsequently underwent robot-assisted APV revision. Patient demographics, medical history, perioperative parameters, and continence status were collected retrospectively (Table 1).
APV=appendicovesicostomy.
Initial APV surgery was performed for bladder dysfunction because of posterior urethral valves, myelomeningocele, and traumatic L2 spinal cord transection. No patient had a ventriculoperitoneal shunt or a bladder augment. On preoperative urodynamics, bladder capacity ranged between 220 and 230 mL. One patient had uninhibited bladder contractions at 50 to 80 mm Hg. No patient had end full pressures >40 mm Hg.
Two patients underwent APV revision alone. The third patient underwent simultaneous APV revision and bladder neck closure. APV revision was conducted a mean 14 months (range 6–34 mos) after initial surgery. Mean operative time was 168 minutes (range 106–232), and EBL was ≤5 mL for all patients. No procedure needed conversion to open surgery. Intraoperative findings ranged from partial to complete separation of the APV from the bladder tunnel. Only the patient who underwent bladder neck closure needed more than an overnight stay. One patient needed postoperative catheter placement because of a false passage, which resolved. No other complications occurred, and no APV leakage was identified for all patients at last follow-up (median 5, range 2–9 mos).
Discussion
The Mitrofanoff APV was first described in 1980 and remains to this day an integral component of the treatment for patients with neurogenic bladder. 13 The incontinence rates for open APV have been reported at 0% to 9%. 14 The use of robotics in pediatric surgical procedures is increasing and is being applied to a greater complexity of operations, including APV. The first report of a completely robot-assisted APV was described in 1994 and was performed in a 7-year-old boy with a history of posterior urethral valves.
Early robotic series describe an APV incontinence rate of 10%. 15,16 Nguyen and associates 15 reported APV incontinence at a median follow-up of 14.2 months in 1 of 10 children who underwent robot-assisted APV. The patient continued to leak despite maximum anticholinergic therapy, but was successfully treated with dextranomer/hyaluronic acid injection. The patient eventually needed augmentation cystoplasty because of poor bladder compliance. Wille and colleagues 16 reported APV incontinence at a median follow-up of 20 months in 1 of 11 children who underwent robotic APV. The patient was successfully treated with dextranomer/hyaluronic acid injection. On retrospective review, the patient was noted to have a submucosal tunnel length of 3 cm, the shortest of the series (median 4 cm, range 3–5 cm). The authors concluded that a ≥4 cm tunnel length is important for obtaining APV continence.
APV incontinence developed in three children who underwent robotic APV at our institution. These three patients failed less invasive treatments before undergoing robot-assisted APV revision. Although we did not directly measure or annotate tunnel length at the time of initial operation, we did identify partial to complete separation of the APV, explaining why dextranomer/hyaluronic acid injection failed. The three patients needed a brief hospital stay, and all reported APV continence at a median follow-up of 5 months. The only complication involved one patient in whom a false passage developed after resuming intermittent APV catheterization. The patient needed cystoscopy-guided catheter placement. The false passage resolved after a short treatment with an indwelling catheter.
Concerns have been raised regarding the density of intra-abdominal adhesions that may be faced during repeated robot-assisted operations. Adhesiolysis was at a minimum with this series of patients and did not subjectively increase the complexity or length of our operations. With appropriate patient selection, we believe it is safe to perform repeated robot-assisted procedures, rather than reflexively selecting an open approach in fear of intra-abdominal adhesions.
Conclusion
This initial series of robot-assisted APV revisions expands the scope of robot-assisted revision surgical procedures in children. Robot-assisted APV revision was technically feasible and safe in this early study but will benefit from a larger patient cohort and longer follow-up.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviation Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.