
Abstract
Purpose:
Developments in optical diagnostics have potential for less invasive diagnosis of upper urinary tract urothelial carcinoma (UUT-UC). This systematic review provides an overview of technology, applications, and limitations of recently developed optical diagnostics in the upper urinary tract and outlines their potential for future clinical applications. In addition, current evidence was evaluated.
Literature Search:
A PubMed literature search was performed and articles on narrow band imaging (NBI), photodynamic diagnosis (PDD), Storz professional imaging enhancement system (SPIES), optical coherence tomography (OCT), and confocal laser endomicroscopy (CLE) regarding UUT-UC were reviewed for data extraction. Study quality was reviewed according to Quality Assessment of Diagnostic Accuracy Studies and Innovation, Development, Exploration, Assessment, and Long-term follow-up (IDEAL) standards.
Results:
Four articles available for quality assessment, demonstrated high level of evidence, but low level of IDEAL stage. NBI and SPIES enhance contrast of mucosal surface and vascular structures, improving tumor detection rate. A first in vivo study showed promising results. PDD uses fluorescence to improve tumor detection rate. However, due to the acute angle of the ureterorenoscopes there is an increased risk of false positives. OCT produces cross-sectional high-resolution images, providing information on tumor grade and stage. A pilot study showed promising diagnostic accuracy. CLE allows ultrahigh-resolution microscopy of tissue resulting in images of the cellular structure. CLE cannot be applied in vivo in the upper urinary tract yet, due to technical limitations.
Conclusions:
NBI, SPIES, and PDD aim at improving visualization of UUT-UC through contrast enhancement. OCT and CLE aim at providing real-time predictions of histopathological diagnosis. For all techniques, more research has to be conducted before these techniques can be implemented in the routine management of UUT-UC. All techniques might be of value in specific clinical scenarios and allow for integration, for example, OCT with NBI, and could therefore improve tumor detection and staging and help in selecting the optimal treatment for the individual patient.
Introduction
C
Radiological and cytological evidence on small and/or flat lesions are reported with a low accuracy. 1 –3 Secondly, URS requires anesthesia and does not provide real-time information on stage and grade of the disease. Pathological diagnosis is often inconclusive due to the small samples that are obtained, mainly because of the limitations of the equipment. 4 Furthermore, carcinoma in-situ (CIS) lesions are easily missed on URS due to their flat appearance. Consequently, a high rate of tumor upgrading and upstaging is reported following nephroureterectomy. 5
The standard treatment for UUT-UC has been open or laparoscopic nephroureterectomy. 6 Recently, the EAU guidelines accepted conservative endoscopic treatment using URS for a select group of UUT-UC patients with low-volume, low-grade, and low-stage disease. 6 To select patients eligible for endoscopic treatment, information on tumor stage and grade is essential. With the current diagnostic tools, selection of patients for conservative treatment is still suboptimal. Novel optical diagnostic techniques, based on the interaction between light and tissue, have the potential to improve UUT-UC visualization. These interactions include scattering, absorption, and fluorescence, all of which are characteristic for certain tissue types. Some of these techniques aim at improved visualization of urothelial tumors (narrow band imaging [NBI], Storz professional imaging enhancement system [SPIES], and photodynamic diagnosis [PDD]), while other techniques aim at providing real-time intraoperative information on tumor grade and stage (optical coherence tomography [OCT] and confocal laser endomicroscopy [CLE]). Most research on the application of optical diagnostics on the urothelium has been done in the field of bladder cancer. 7,8 In case of the upper tract, however, the limited space in the ureter and the difficulty to reach the upper urinary tract creates an entirely new spectrum of challenges for new optical techniques.
In this systematic review, the principles of these new optical techniques are described with their applicability in the diagnosis and treatment of UUT-UC and outline their feasibility in current clinical applications. In addition, we evaluate the relevant literature according to standard classifications. 9 –12
Materials and Methods
Literature search
A literature search was conducted (May 22, 2014) in PubMed and the Cochrane library using the search terms: “Upper Urinary Tract OR ureter AND Narrow Band Imaging,” “Upper Urinary Tract OR ureter AND Photodynamic Diagnosis,” “Upper Urinary Tract OR ureter AND Storz Professional Imaging Enhancement System (SPIES),” “Upper Urinary Tract OR ureter AND Optical Coherence Tomography,” and “Upper Urinary Tract OR ureter AND Confocal Laser Endomicroscopy.” Original English-written articles were selected. Review articles, reply to author, and articles describing other than the upper urinary tract were excluded (Fig. 1).
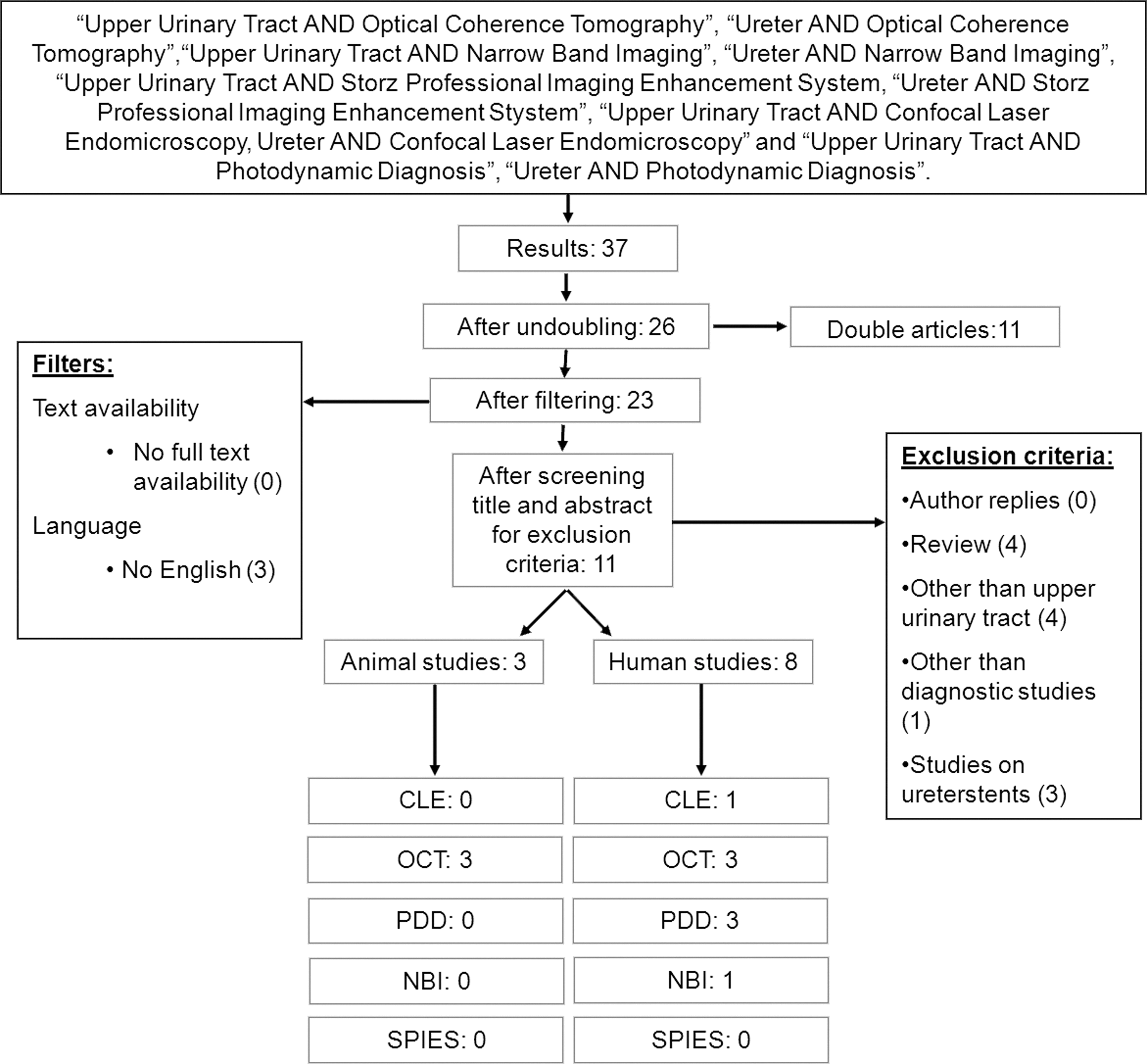
Diagram outlining study selection process.
Data extraction
Full text articles were reviewed for data extraction by two authors (M.T.J.B. and M.P.L.-P.). Study quality of human in-vivo diagnostic studies was reviewed according to Quality Assessment of Diagnostic Accuracy Studies (QUADAS) standards. 11 Innovation, Development, Exploration, Assessment, and Long-term follow-up (IDEAL) stage 9,10 and level of evidence according to the Oxford Center of Medicine for diagnostic tests 12 were subsequently assessed. Ex vivo and animal studies were not included for quality assessment. In case a single research group published multiple articles on a specific optical diagnostic technique, only the most recent publication was taken into account.
Results
The literature search rendered, in total, 37 articles. After undoubling, filtering, and applying exclusion criteria, 11 articles remained for analyses on study quality and data extraction (Fig. 1). CLE rendered one article, NBI rendered one article, OCT rendered six articles, SPIES rendered no articles, and PDD rendered three articles. In total, eight articles reported on human studies, the other three articles were conducted in animals.
Quality assessment
Of the 11 articles, four articles in a human in vivo setting were suitable for quality assessment (Fig. 2). All these prospective studies have a 2B level of evidence. However, all studies have been conducted according to the first steps of the IDEAL standards (1-2a). Evaluation by the QUADAS standards, to assess the quality of diagnostic accuracy, showed minimal bias of the four studies available for quality assessment.

Quality assessment according to Quality Assessment of Diagnostic Accuracy Studies (QUADAS) and Innovation, Development, Exploration, Assessment, and Long-term follow-up (IDEAL) standards and Level of Evidence of human in-vivo studies. Only one optical coherence tomography (OCT) study was included, since two other studies were conducted ex-vivo. Only one study on photodynamic diagnosis (PDD) was included, since the other two studies were conducted by the same study group and likely to be conducted in the same patient group. *Reference test: white-light ureterorenoscopy. **This study was conducted in vivo in the bladder and ex vivo in the upper urinary tract. Since we can imagine that the results of the bladder resemble results in the upper urinary tract, we included this study for quality assessment.
Techniques based on light absorption
Narrow band imaging
NBI Olympus® is an optical image enhancement technique for endoscopic applications, with demonstrated value in gastroenterology and urology (bladder). 13 –15 NBI is based on the principle that the depth of light penetration into the mucosa increases with increasing wavelength and enhances contrast between mucosa and microvascular structures (Table 1). By illuminating the tissue with specific wavelengths (blue 415 nm and green 540 nm), both strongly absorbed by hemoglobin, the vascular structures appear dark brown/green against a pink/white mucosal background (Fig. 3). 13,16 New digital flexible endoscopes with integrated white light (WL) and NBI are already commercially available allowing the application also in the upper urinary tract. Until now, only one report is published on NBI in the upper urinary tract, which consisted of 27 patients undergoing URS. Of these 27 patients, only 15 had UUT-UC. NBI improved the tumor detection rate by 22.7% compared with white light by diagnosing five additional tumors and identifying border extension in another three tumors. 17 Although promising, this study could be subject to observer bias because of its design, in which WL and NBI URS were performed subsequently by the same urologist.
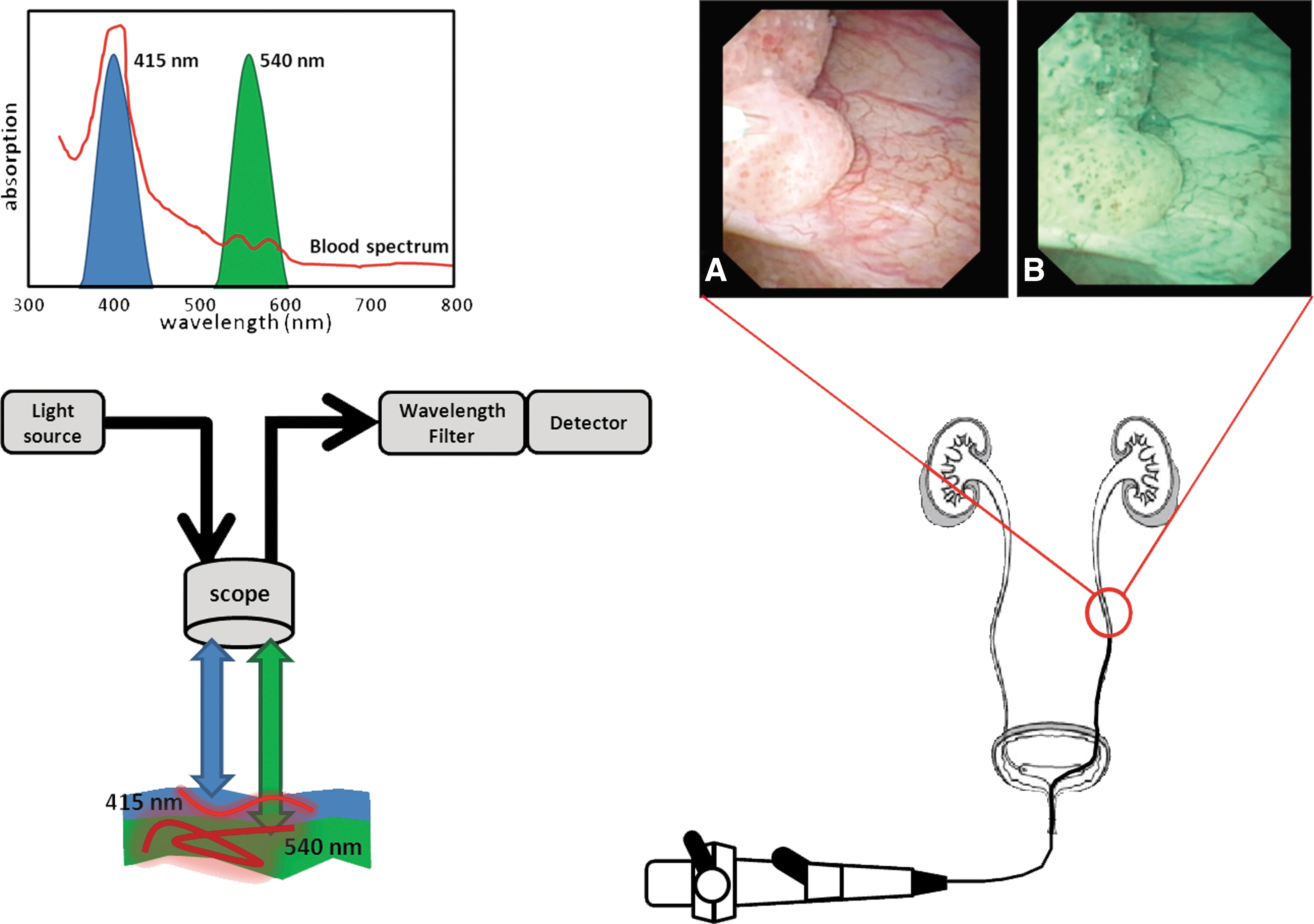
Narrow band imaging is based on the phenomenon that the depth of light penetration increases with wavelength. Tissue is illuminated with light centered on 415 nm (blue) and 540 nm (green), which are both absorbed by hemoglobin more strongly than other tissue. The blue light enhances the superficial capillary network, whereas the green light enhances the visibility of deeper vessels. WL: white light
NBI, SPIES, and PDD have previously demonstrated a high rate of false positives on bladder urothelium. Future research should reveal if this high rate of false positives is also found in the upper urinary tract.
OCT=optical coherence tomography; NBI=narrow band imaging; SPIES=Storz professional image enhancement system; PDD=photodynamic diagnosis; CLE=confocal laser endomicroscopy; URS=ureterorenoscopy; na=not applicable; CIS=carcinoma in situ.
Storz professional image enhancement system
A new technology using spectral separation is recently introduced called Storz professional image enhancement system (SPIES®) (Table 1). White-light images are acquired with an RGB camera, after which several different digital imaging modes can be used to modify the displayed image (Fig. 4). The system comprises two modes (SPECTRA A/B), which pronounce the imaging spectral separation using different color renderings, highlighting the contrast between different tissues and structures. A third mode (CLARA) uses a local brightness adaptation to achieve clearer visibility of darker regions within the image, and a fourth mode (CHROMA) enhances the structures within the displayed image using an increased color contrast. The clinical value of SPIES is currently under investigation and no clinical data of the upper urinary tract are available yet.
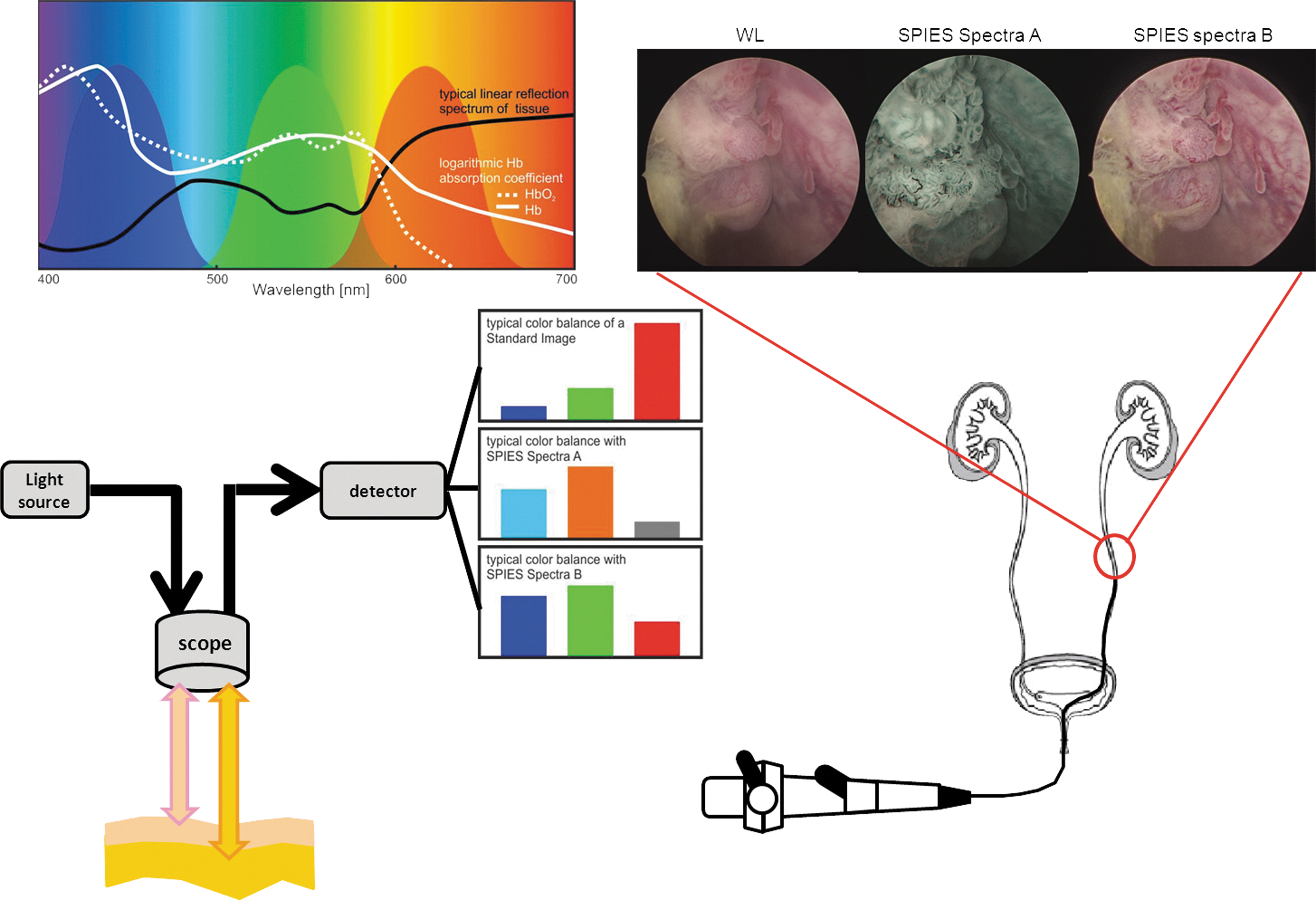
Storz Professional Image Enhancement System (SPIES) filters acquired white-light images digitally to produce enhanced contrast images. Several modes can be used to increase viewing comfort for the endoscopist, enhancing sharpness of the displayed images, and providing specific color renderings. Spectral separation within the camera is amplified by adapted color processing algorithms of the whole spectral light information. Inserts demonstrating upper urinary tumor seen with white light and SPIES Spectra A and Spectra B.
Techniques based on fluorescence
Photodynamic diagnosis
PDD employs fluorescence as a contrast mechanism to localize abnormal tissue (Table 1). PDD is based on the selective accumulation of a fluorochrome in malignant tissue. Absorption of high-energy light of the appropriate wavelength (i.e., ∼400 nm) excites the electro-vibrational state of the fluorochrome. When the molecule relaxes to the ground state, a photon is emitted (i.e., 590–700 nm) to account for the energy difference. The fluorescent photon has less energy than the excitation photon; since the energy of light is inversely proportional to its wavelength, the emitted light has a longer wavelength than the illuminating light. Therefore, discrimination between the two types of light is possible (Fig. 5). Several exogenous fluorochrome agents have been investigated to induce exogenous fluorescence. Most research in the upper urinary tract has been conducted using the approved porphyrin-related fluorochrome 5-aminolaevulinic acid (5-ALA).
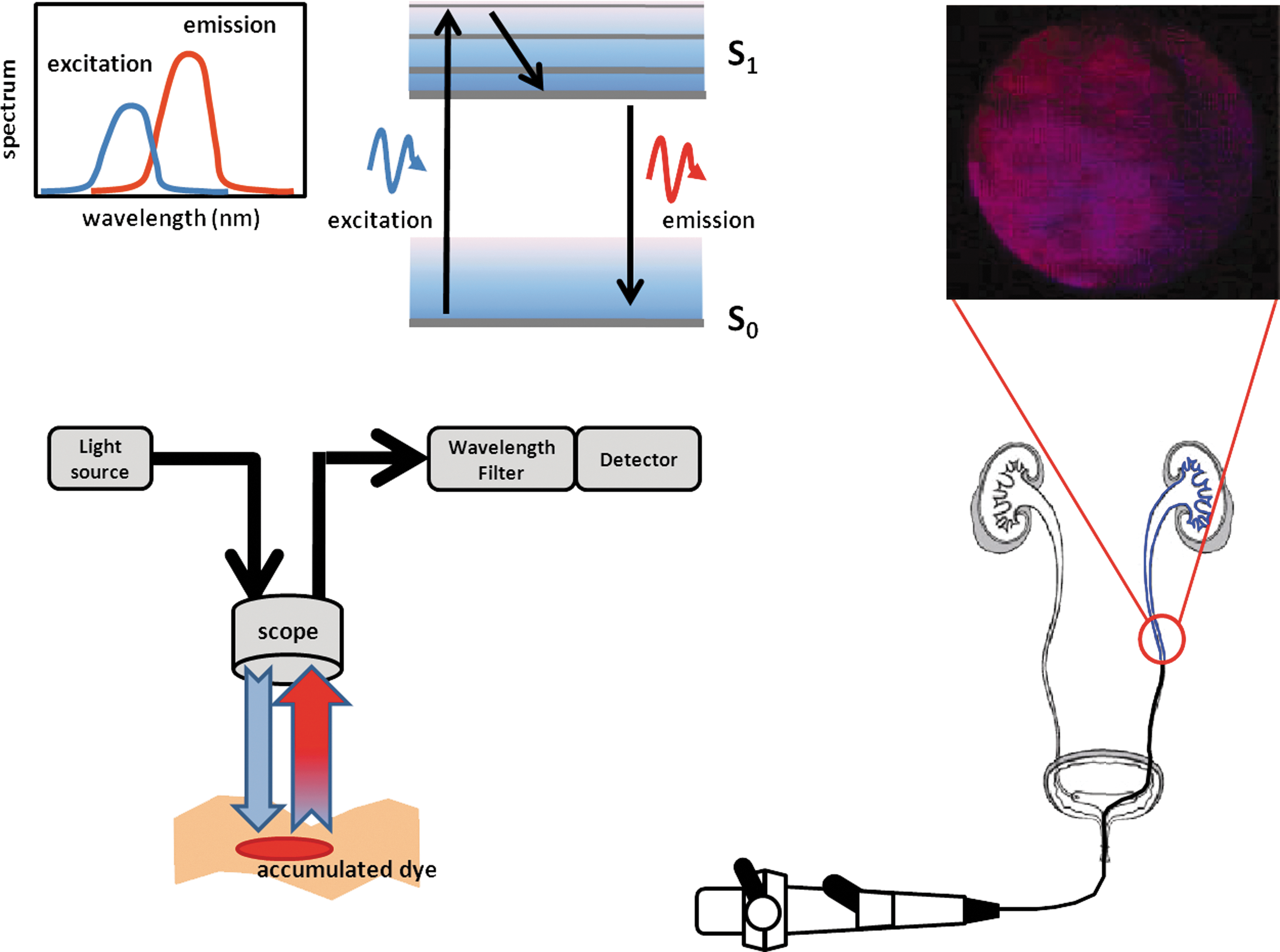
PDD is based on fluorescence of externally applied dyes that accumulate in tumors. When a dye absorbs light, it is excited from the ground state (S0) to a higher energy level of the first excited state (S1), before relaxing to the lowest vibrational energy level of S1. Subsequently, the dye returns to the ground state while emitting a photon of lower energy (higher wavelength) than used for excitation. Appropriate filtering separates the emitted light from the excitation. Insert shows a PDD image of urothelial carcinoma in the ureter. Since a tangential light beam is almost inevitable in the ureter, the result interpretation is hampered and causes more false positives.
Endoscopes with special light sources and filters are used to illuminate tissue with blue light (380–470 nm) that corrects for heterogeneous illumination and distance variations. It also largely compensates for varying blood absorption, and accumulated 5-ALA in malignant tissue appears pink/red on a blue background.
In the upper urinary tract, several impediments exist for application of this technique. Concern is optimal delivery of fluorochromes and visualization in the setting of anatomic obstacles. Delivery of fluorochromes seems technically possible by nephrostomy or urinary stent, 18 but equal administration of fluorochromes and optimal duration of urothelial exposure to fluorochromes are more difficult to establish because of the small cavity sizes. 16 Furthermore, visualizing fluorescent thin normal urothelium of the ureter requires a perpendicular viewing angle. The ureteroscope's longitudinal axis creates a tangential viewing angle, in which the urothelial layer appears as a thicker layer with a corresponding increase in fluorescence, potentially resulting in false positives.
An alternative for 5-ALA instillation is oral administration of the same fluorophore, which has been described in three studies. The first in-human study demonstrated the feasibility on oral 5-ALA in patients with suspicion of UUT-UC. 19
In two larger studies, more lesions were found in the upper urinary tract compared with standard white-light imaging. 20,21 Although a study on sensitivity and specificity of UUT-PDD revealed an increased sensitivity compared with standard white-light endoscopy, this difference was not statistically significant. 20,21 In summary, PDD enables improved visualization of upper urinary tract tumors. However, major limitations are the administration of 5-ALA and the higher false-positive rate due to the tangential viewing angle of the ureteroscopes.
Confocal laser endomicroscopy
CLE is an ultrahigh-resolution microscopy technique that allows imaging of tissue as much as a depth of 400 μm (Table 1). This imaging depth and resolution is achieved using lasers and optics, which are combined with a very small hole (pinhole) that acts as a diaphragm in the microscope objective. This ensures that only light from the focus in the tissue is collected. The light that is out of focus is rejected by the pinhole (Fig. 6). CLE uses fluorescence from fluorescein to stain tissue microarchitecture and small vessels, which rapidly diffuses through the body after intravenous injection. Recent advantages in instrument miniaturization have led to the development of flexible fiberoptic confocal microscopes that can be used with standard endoscopy to provide real-time information on tumor grade. In an ex vivo study, urothelial cells and lamina propria were clearly recognized. 22 A drawback of CLE is sensitivity to tissue movement leading to motion artifacts that could result in blurred images. Although commercially available CLE devices are now available with decreased probe size, with a wider field of view, and an improved imaging of the microarchitecture of tissue, it also results in a lower cellular resolution, which is needed for grading. 23
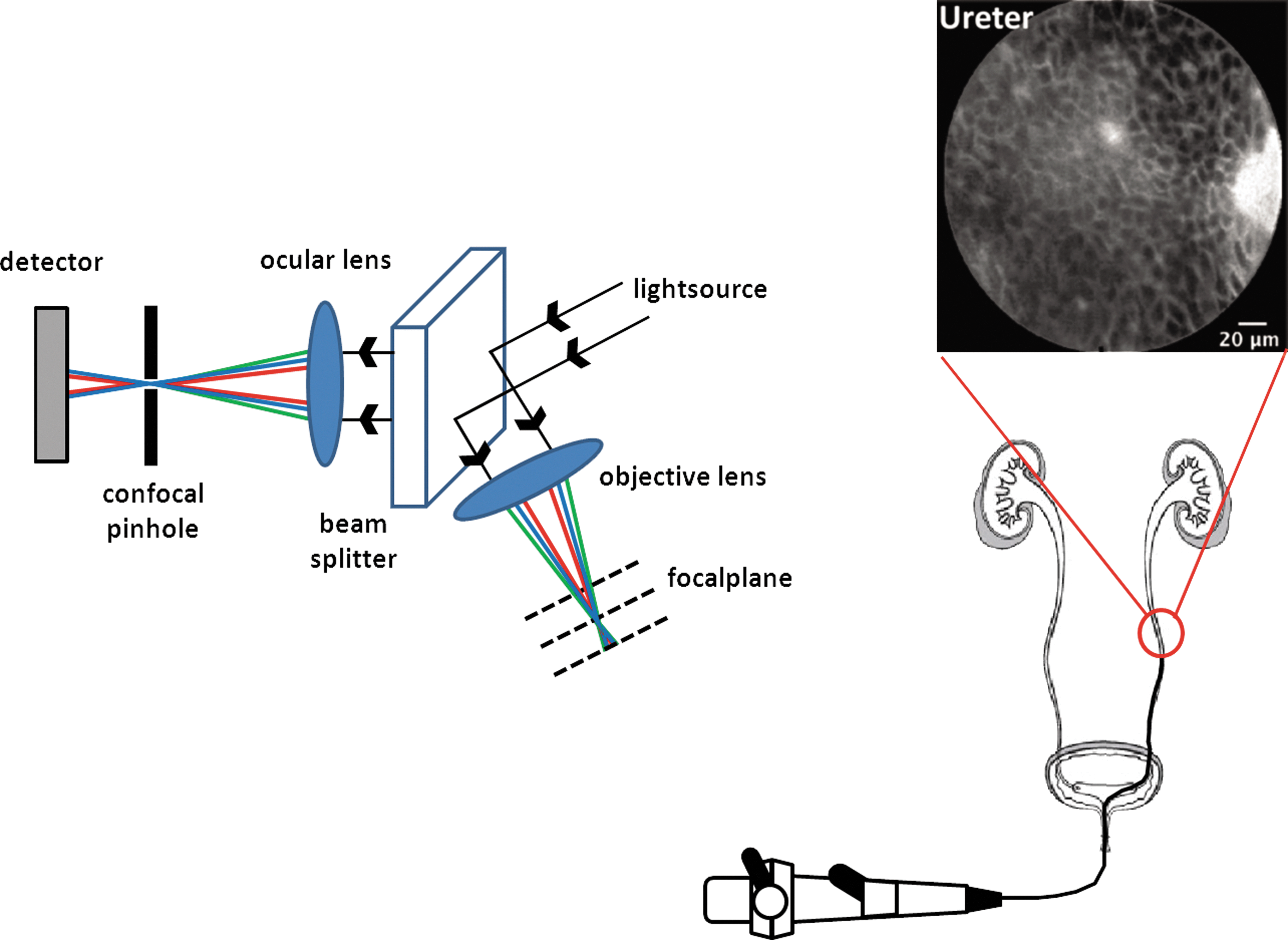
Confocal endomicroscopy is based on the suppression of out-of-focus light by the insertion of a pinhole before the detector. This results in the detection of back-scattered light that originates from the focal plane only (red and blue in the overview), while light that is back-scattered outside the focal plane (green in the overview) is stopped by the pinhole. Miniaturization of a confocal microscope affects the numerical aperture of the system, which will directly influence the resolution of the system. Insert shows ex vivo confocal laser endomicroscopy of the normal proximal ureter from a radical nephrectomy specimen. Normal urothelium showing uniform monomorphic cells consistent with intermediate cells. Insert image courtesy of Aristeo Lopez and Joseph Liao, Stanford University.
Techniques based on light scattering
Optical coherence tomography
OCT is analogous to ultrasonography, using back-scattered light instead of back-reflected sound waves to produce micrometer-scale resolution cross-sectional images (Table 1). 24 Recent OCT research investigates this technology in the diagnostic work-up of several epithelial cancers. 25 –27 In OCT, layered tissue anatomy can be distinguished. Interruption or absence of layered tissue under a visible lesion is indicative for tumor stage. However, light scattering causes a decrease of OCT signal magnitude over depth and limits the imaging range to ∼2 mm depth. The rate of OCT signal decrease with depth is quantified by the attenuation coefficient (μoct) that allows in vivo differentiation between different tissue types (Fig. 7). 26 –29 This distinction results from differences in intra- and extracellular organization of the tissue, which is reflected in the light scattering properties. Measurement of μoct is therefore sensitive to the differences in organization associated with different grades of the lesion. The combination of real-time high-resolution images and extraction of the optical attenuation coefficient gives OCT the ability to provide real-time information on tumor stage and grade in the upper urinary tract.

OCT, the optical equivalent of ultrasound imaging, measures light reflectivity vs depth. It is based on white-light (large wavelength bandwidth) interferometry, where interference signals are only detected if the light in the sample and reference arm has traveled equal distances. Thus, by varying the length of the reference arm, the imaging location in the tissue can be controlled. Modern embodiments of OCT do not use moving reference mirrors; instead, technical complexity is shifted toward either the light source (that sequentially provides each wavelength within the source bandwidth at high speed) or the detector (which detects each wavelength within the source bandwidth in parallel).
The potential of OCT for staging/diagnosis of UUT-UC has been investigated ex vivo in the porcine and human ureter where it clearly distinguished the ureteral wall layers, particularly the urothelium and lamina propria. 30 –32 When compared with endoluminal ultrasonography, OCT can significantly better distinguish the wall layers of ex vivo porcine ureter. 33 An in vivo human pilot study in the ureter showed that in normal appearing urothelium, the layered tissue anatomy, including basement membrane, CIS, and visible protrusions, can be visualized on OCT images. Toward grading, UUT-OCT was able to visually differentiate between noninvasive and invasive tumors and to differentiate between low- and high-grade lesions by quantifying μoct. 34
Current commercially available OCT systems are limited to image lumina with a maximal diameter of 10 mm, compromising visualization of the pyelum as a whole. Furthermore, if tumor thickness transcends scattering-limited imaging depth in tissue (∼2 mm), invasiveness cannot be assessed.
Discussion
We performed a systematic review of the current literature on optical diagnostics in the upper urinary tract. Only 11 articles were available, most of them were conducted ex vivo in humans or animals. Four articles were available for quality assessment, demonstrating the lack of evidence. All studies are in an initial phase of human research according to IDEAL stages for surgical innovations. All in vivo human studies showed high quality of diagnostic tests and low-bias risk.
From a clinical point of view, the ideal adjunct modality for endoscopic procedures in the upper urinary tract should (1) detect malignant and premalignant lesions with a high sensitivity and specificity, (2) provide real-time reliable information on grade and stage, (3) reliably identify the extension and deep margins to achieve complete resection and consequently identify residual tumor within resection margins, (4) be physician friendly; easy to apply with a short learning curve for image interpretation, (5) avoid the use of exogenous contrast agents, and (6) preferably be low in costs. 8,23 URS with conventional biopsy does not meet all of these conditions. Tumor detection and knowledge about grading and staging should be the ultimate diagnostic objective. Therefore, the potential combination of endoscopy with optical diagnostic techniques could increase diagnostic accuracy and improve treatment selection and may reduce costs.
NBI, SPIES, and PDD aim at improving visualization of upper urinary tract tumors during URS. OCT and CLE aim at providing minimally invasive, real-time, and objective predictions of histopathological diagnosis.
However, endoscopy in the upper urinary tract is challenging due to its small diameter and vulnerability of tissues. This environment creates many limitations that have to be overcome before optical diagnostics can be reliably applied in the upper urinary tract. In our opinion, the most optimal optical device should be able to detect urothelial tumors, to provide depth-resolved tissue information, which allows staging and specific information on biochemical or intracellular changes in the tissue, which allows grading, all in real time. A combination of NBI, SPIES, or PDD with OCT or CLE could be such a real-time optical adjunct modality.
Further research needs to be conducted to evaluate the true value, before they can be implemented in the management of UUT-UC. Current available data are too preliminary to evaluate these new technologies and implement them into the diagnostic work-up of patients with UUT-UC. Therefore, we would plea for more and better conducted studies for the evaluation of diagnostic technologies in the upper urinary tract. Studies on optical technologies in the upper urinary tract involve translation from a biomedical engineering technology, sometimes already applied in routine care for other specialties, for example, gastroenterology, cardiology, and ophthalmology. As it involves the use of a medical device instead of a pharmacological product, the optimal way to proceed is following the IDEAL evaluation criteria, 1,2 described by the Balliol collaboration. This evaluation equals surgical innovation to the different phases of the pharmacological research. CLE has been described for the IDEAL stage 1 (Innovation phase). PDD, OCT, and NBI are framed as IDEAL stage 2A or developmental phase. To develop these technologies into a diagnostic test, results should be compared with the standard test at use. In the case of PDD and NBI, the standard test is WL-URS (including biopsies), where OCT uses histology as gold standard. It is recommended to combine the IDEAL methodology with the QUADAS for assessing accuracy of a diagnostic test.
These clinical studies should provide a full diagnostic accuracy analysis according to the QUADAS recommendations, including sensitivity, specificity, positive predictive value, and negative predictive value. However, upper urinary tract tumors are rare, resulting in a limited study population and therefore require a multicenter approach when entering IDEAL phase 2b (exploration phase) or 3 (assessment phase).
So far, only two studies on optical diagnostics in the upper urinary tract are registered at clinicaltrials.gov, using similar search terms as described in the method section. Both studies comprise optical coherence tomography, and only one study is recruiting patients at this moment.
Conclusions
NBI, SPIES, and PDD aim at improved detection of upper urinary tract tumors.
OCT and CLE aim at providing real-time, minimally invasive, and objective predictions of histopathological diagnosis. Optical diagnostics might overcome the limitations of the current diagnostic standard of upper urinary tract tumors to determine which tumors can be treated endoscopically. Although these optical techniques show promising results, more and better conducted prospective studies should be done before they can be implemented in the diagnostic work-up of upper urinary tract tumors.
Footnotes
Acknowledgment
The authors would like to thank Aristeo Lopez and Joseph Liao, Stanford University for generously providing the CLE figure used in this article.
Disclosure Statement
No competing financial interests exist.