
Abstract
Purpose:
Our study sought to demonstrate the effects of remote ischemic preconditioning (R-IPC) on renal function in a large animal (porcine) solitary-kidney model.
Methods:
Twelve pigs were assigned to two groups: Each underwent a right nephrectomy followed by a week of recovery. Group 1 (No-IPC) underwent left renal hilar clamping for 90 minutes. Group 2 underwent right and left iliac artery clamping for 10 minutes each (R-IPC), followed by left hilar clamping for 90 minutes. Serum creatinine was drawn for both groups before ischemia (preoperative), then at 6 hours, 24 hours, 3 days, and 7 days after. Kidneys were harvested at 24 hours or 7 days for histologic analysis, and the degree of acute tubular necrosis (ATN) or lymphocyte invasion was quantified.
Results:
Paired serum creatinine values were analyzed between time points. For Group 1, paired differences existed at 24 hours (P=0.008) but not at 3 days or 7 days. For Group 2, paired differences existed at 24 hours (P=0.006) but not at 3 days or 7 days. The mean preoperative serum creatinine level was similar between groups (P>0.05). The change in serum creatinine level was not significantly different between groups at any time point. Histologic analysis revealed rare evidence of ATN at 24 hours in Group 2, but not in Group 1. At 7 days, neither group showed ATN, and both showed 1-2+evidence of lymphocytic infiltrates.
Conclusion:
R-IPC in a solitary-kidney porcine model does not confer renal protection from warm ischemia either as evidenced by renal function measures or on histologic analysis.
Introduction
P
Originally, IPC was introduced in 1986 by Murry and associates 7 in a study that showed myocardial infarct size could be reduced by IPC in dog hearts subjected to prolonged ischemic insult. Since, multiple small animal studies have shown IPC to be effective 5,8 ; however, these results are less clear in larger animal studies. 9 Initially, the ischemic stimulus was studied by directly targeting the organ itself and was termed local IPC (L-IPC). 5 Over time, a more practical alternative to L-IPC was introduced. This method, termed remote ischemic preconditioning (R-IPC), involves causing a remote organ or tissue to become ischemic resulting in the release of cytokines and other factors that confer protection to the target organ. 4 The majority of R-IPC studies have been conducted looking at cardiac ischemia, such as coronary artery bypass grafting, heart valve surgery, and abdominal aortic aneurysm repair and have generally shown promising results. 8 –11
Within the urologic literature, the effectiveness of R-IPC on renal ischemic injury is limited, 6 and the benefits of R-IPC remain in question. As with L-IPC, studies in small animal models subjected to R-IPC have yielded promising results. 8,10 Within these studies, results appear favorable, although there remains the question of their applicability to human subjects. In this regard, large animal models more closely represent human physiology and thus are the next logical progression in studying this phenomenon. Larger animal studies are scant, however, and have yielded conflicting results. 9,11 In addition, the goals of this study were to evaluate not only the clinical utility of R-IPC, but to also apply R-IPC in a clinically practical manner. We therefore sought to study, for the first time, the effects of R-IPC on renal function after an ischemic insult in a large animal (porcine) solitary-kidney model.
Methods
The study protocol was approved by the Institutional Animal Care and Use Committee. Twelve female pigs weighing 60 to 65 kg each underwent initial right laparoscopic nephrectomy to create a single-kidney model and underwent recovery. After a 1-week period to allow stabilization of renal function, the pigs were assigned to two groups of six.
Group 1 (No-IPC) underwent laparoscopic left renal hilar dissection followed by hilar clamping for 90 minutes. A 90-minute ischemia time was chosen based on work by Laven and colleagues 12 in which this duration showed significant initial renal compromise but avoided the morbidity associated with longer ischemia times. The ischemic clamp time of 90 minutes was chosen based on data from several studies in which 75 minutes of warm ischemia time (WIT) did not cause significant renal compromise, 90 minutes did show some degree of renal compromise, and in which ischemia times greater than 120 minutes showed significant morbidity. 9,12 –14
Group 2 (R-IPC) underwent laparoscopic right and left iliac artery clamping for 10 minutes, followed by a reperfusion period of 30 minutes. The R-IPC protocol was based on a randomized trial in humans in which two cycles of 10 minute intermittent clamping of the common iliac artery yielded improved outcomes during elective aortic aneurysm repair that included a significant reduction in renal impairment. 15 The left renal hilum was then clamped for 90 minutes after R-IPC. A laparoscopic Satinsky clamp was used for renal hilar and common iliac artery clamping. Pneumoperitoneum was maintained at 15 mm Hg, and three ports were used for instrumentation in all procedures.
All pigs were administered antibiotics (enrofloxacin) for 48 hours after surgery. Intramuscular Telazol 3–6 mg/kg was used as the anesthetic followed by isoflurane inhalation in all cases. For the second surgery, standardized intraoperative and perioperative intravenous hydration with 500 mL of physiologic saline was administered perioperatively. No mannitol, furosemide, heparin, nephrotoxic drugs, or renal hypothermia was used. The rectal temperature was maintained between 36°C and 39°C with the use of heated blankets and warmed intravenous fluids. Pulse oximetry, heart rate, and temperature were monitored continuously during the operation. For pain control, intravenous buprenorphine was used intraoperatively, and oral Carprofen was used on postoperative day 1 and day 2.
Serum creatinine levels were checked for both groups just before the second surgery (preoperative), then at 6 hours, 24 hours, 3 days, and 7 days after. Two animals from each group were sacrificed at 24 hours, and the remaining 4 animals were sacrificed at 7 days. In each case, the kidneys were harvested and prepared for histologic analysis. Hematoxylin and eosin staining was performed in the standard manner. The pathologist reported the degree of lymphocytic infiltration/lymph node aggregates (inflammation) and the degree of acute tubular necrosis (ATN) separately on a 1 to 5 scale. This system was constructed based on previously published methods incorporating the lesion size in the kidney where: 1=no abnormality, 2=lesion less than 25% of sample, 3=lesion 25% to 50%, 4=lesion 50% to 75%, 5=lesion greater than 75%. 16 The pathologist was blinded to the study groups.
IBM SPSS statistics V19 was used for statistical analyses, and differences were considered to be statistically significant at P<0.05.
Results
Serum creatinine values were compared between preoperative and each specified postoperative time point for both groups. Figure 1 demonstrates the progression of serum creatinine values at each time point for the two groups. In all but two pigs, the serum creatinine peaked at 24 hours. For group 1 (No-IPC), paired differences existed at 24 hours (P=0.008) but not at 3 days (P=0.240) or 7 days (P=0.254). For group 2 (R-IPC), paired differences existed at 24 hours (P=0.006) but not at 3 days (P=0.063) or at 7 days (P=0.081). There was no difference between the mean serum creatinine levels for both groups at preoperative baseline (P>0.05). The change in serum creatinine level from preoperative values between Groups 1 and 2 was higher for Group 2 (R-IPC) at each time point after baseline, but this was not significantly different at 24 hours, 3 days, or 7 days (P=0.136, 0.256, 0.425, respectively) (Table 1).

Trend in serum creatinine level over time for Group 1 (No-ischemic preconditioning [IPC]) and Group 2 (remote IPC [R-IPC]). Error bars designate the standard deviation of the mean creatinine level at each time point.
Preop=preoperative; CR=serum creatinine; R-IPC=remote ischemic preconditioning.
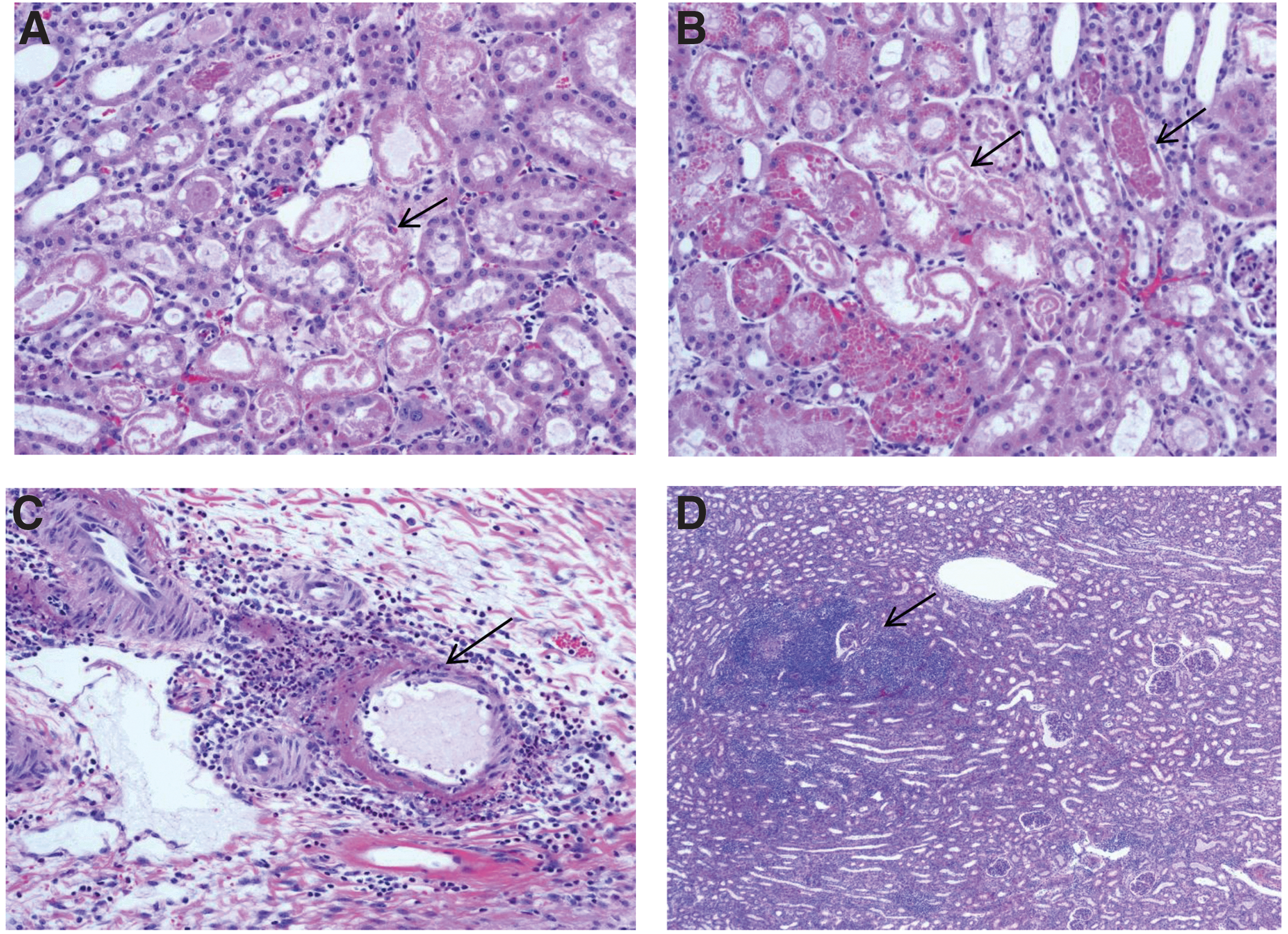
Histologic analysis revealed rare (1+) evidence of ATN at 24 hours in Group 2 (R-IPC) (Fig. 2a, 2b) but not in Group 1 (No-IPC). At 7 days, neither group showed evidence of ATN; however, both showed 1–2+evidence of lymphocytic infiltrates/lymph node aggregates (Fig. 2c, 2d).
(
Discussion
Several methods have been reported that minimize renal ischemic damage during PN. These include early hilar unclamping, 17 renal hypothermia, 18 segmental renal artery clamping, 19 and selective branch microdissection. 20 Each has drawbacks and limitations, some more so during minimally invasive PN. Early renal hilar unclamping has been reported to have greater blood loss and longer operative times than a standard clamping, 21 while there is also yet to be a consistent and reliable means of cooling the kidney during laparoscopic or robot-assisted PN. 6 Segmental renal artery clamping and renal artery branch microdissection are promising techniques; however, these are technically challenging and necessitate advanced laparoscopic or robotic skills.
One strategy theorized to reduce renal injury during PN is IPC. This refers to the induction of a brief episode of ischemia followed by reperfusion. Theoretically, the initial ischemic insult results in tissue tolerance to subsequent renal ischemic injury 6 ; however, the mechanism and overall effects of IPC are not well understood. The current hypothesis is that IPC induces biphasic protection from ischemia injury where short-term mediators, such as adenosine, bradykinins, and catecholamines, provide the initial protection. Here, the early phase develops rapidly through posttranslational modification of preexisting proteins. IPC also produces a later, less powerful but longer-lasting effect regarded as the later phase or second window of protection. This involves activation of transcription factors and de novo protein synthesis with an end result being the up regulation of inducible nitrous oxide and cyclooxygenase-2, both of which offer cell protection against ischemia. 9
IPC has further shown promise in preventing renal injury in small animal studies. 5,10 In a meta-analysis of 32 trials examining the effect of IPC in laboratory animals, a higher efficacy was found in smaller animals (mouse and rat) vs larger animals, with only one study finding a decrease in efficacy with IPC. Seeming to confirm this analysis, two additional studies showed no benefit to local IPC in a porcine model. 9,22
An equally effective, but potentially clinically more practical approach to preventing ischemic injury is remote ischemic preconditioning (R-IPC). This method entails inducing ischemia to an organ or tissue away from the target organ in an attempt to up-regulate protective mediators. One of several approaches studied has been hind limb occlusion. Wever and coworkers 23 performed R-IPC by brief hind limb occlusion in rats subjected to renal ischemia and reported this to improve renal function by 30% to 60% and reduce renal tubule damage.
In a somewhat indirect study examining renal protection using R-IPC, Ali and associates 15 conducted a randomized trial looking at human patients undergoing abdominal aortic aneurysm repair. Their algorithm involved using two cycles of intermittent clamping of the common iliac artery for 10 minutes followed by 10 minutes of reperfusion. This study found that R-IPC reduced the incidence of not only postoperative myocardial injury and myocardial infarction, but also renal impairment.
Although there are a multitude of additional studies in which R-IPC was performed during cardiac surgeries, its use in kidney surgery is limited. In a single-kidney porcine model, Hernandez and colleagues 22 used 12 female pigs divided in two groups; 60 minutes of complete warm ischemia (WI) or 10 minutes of L-IPC followed by 60 minutes of complete WI. IPC consisted of 5 minutes of hilar clamping followed by 5 minutes of reperfusion. Mean serum creatinine values were significantly increased at all time points in both groups. The study groups were also histologically indistinguishable in terms of degree of tissue injury.
Similarly, Orvieto and coworkers 9 evaluated the ability of L-IPC to confer protection against renal WI using a single-kidney porcine model. Based on serum creatinine values, this study demonstrated no difference using 25 minutes of L-IPC. When examining the group subjected to 60 minutes of L-IPC, not only was there no improvement in renal function, but significant morbidity also was observed.
These study findings are very similar to the findings of our study. In our study, no significant differences between the control group and R-IPC group were identified either based on serum creatinine level or on histologic evaluation. If anything, the R-IPC group showed a consistently increased serum creatinine level, although statistical significance was not reached. In addition, despite a 90-minute ischemic insult, all kidneys recovered to near baseline at 7 days (Fig. 1), and only the change at 24 hours was significant from preoperative values. This would suggest that the innate porcine response to renal ischemia is robust and perhaps an even longer ischemic time would be needed to accurately test any model of ischemic prevention in the porcine kidney.
Although the large animal experience to date would suggest that IPC, performed as either local or remote, does not prevent ischemic injury, this should be interpreted cautiously. A recent randomized, controlled study in humans looking at the protective effects of R-IPC in patients undergoing laparoscopic partial nephrectomy (LPN) was recently published. 6 R-IPC in this study consisted of three 5-minute cycles of right lower limb ischemia followed by 5 minutes of reperfusion. While the estimated glomerular filtration rate was significantly decreased in the control group compared with the R-IPC group at 1 month (15% vs 8%, P=0.034), there were no differences in the glomerular filtration rate at 6 months. The study concluded that R-IPC using transient lower limb ischemia in patients undergoing LPN may reduce renal impairment in the short term and commented that there was a trend toward improvement in the long term.
Some points are worth noting regarding this study. First, the two groups were no different in terms of all demographic variables, most notably preoperative renal function, WIT, and comorbid conditions making meaningful comparisons between groups possible, although there was no mention of comorbidities. The study, however, reported renal function of the affected kidney based on nuclear renal scans. While renal function was significantly better for the affected kidney, the overall renal function of the patients at 1 or 6 months was not significantly different between groups. In addition, of the multiple outcomes examined, the only other variable significantly different between the two groups (other than the renal function at 1 month of the affected kidney) was a urinary marker at 24 hours that normalized by 48 hours. Last, the renal function was not reported in the immediate post-operative period and thus the amount of early phase protection provided is not known.
As previously discussed, there is a second phase of protection that is longer acting and seems to confer a more substantial benefit in terms of renal protection on meta-analysis. Comparing this study to ours is difficult given the different species and length of follow-up. It would seem that humans lack the robust resistance to ischemic damage seen in pigs, and it may be that R-IPC does indeed confer some protection in the later phase, but this was not studied in our model. Future studies using the porcine model would therefore need to include longer periods of ischemia to ensure adequate renal damage as well as potentially longer survival times to identify the benefit of the second phase of protection.
Conclusions
A total of 20 minutes of R-IPC in a solitary-kidney porcine model does not confer renal protection from WI either as evidenced by renal function measures or on histologic analysis in the early phase. Our data further add to the body of literature suggesting the effect of R-IPC is likely species dependent and that the porcine kidney demonstrates a robust response to even prolonged periods of ischemia.
Footnotes
Acknowledgment
This work was previously presented as an abstract in a moderated poster session at the World Congress of Endourology, September 4, 2014, Taipei, Taiwan.
Disclosure Statement
No competing financial interests exist.