
Abstract
Purpose:
We created an Internet-based survey of patients treated for urolithiasis to evaluate for trends in treatment, outcome, and patient satisfaction and to establish internet surveys as a feasible medium for future research of patient urolithiasis treatment experiences.
Materials and Methods:
We used the website “kidneystoners.org” to disseminate the online survey, which queried respondents on treatment type, outcome, and satisfaction. Patient satisfaction was correlated with treatment type and outcome. Chi-square and analysis of variance tests were used to compare responses between treatment types.
Results:
Four hundred forty-three respondents completed the survey. The majority (46%) were treated ureteroscopically, followed by extracorporeal shock wave lithotripsy (SWL, 25%) and percutaneous nephrolithotomy (7%). Other treatments included spontaneous passage (13%), medical expulsive therapy (7%), and home remedies (2%). Sixty-four percent of respondents deemed their treatment “successful,” while 36% reported their treatment as either “partially successful” or “unsuccessful.” Unsuccessful treatment was more likely for SWL (17%) and home remedies (14%) (p=0.002). Most respondents (52%) reported being either satisfied or very satisfied with their treatment choice. Satisfaction did not vary significantly by treatment type, but was significantly associated with treatment success (mean satisfaction 3.8/5 for “successful” vs 1.9/5 for “unsuccessful” treatment; p<0.0001).
Conclusion:
Use of the Internet allows rapid gathering of patient information from a large geographic distribution. Our survey is consistent with previous studies in demonstrating an increased use of ureteroscopy to treat both renal and ureteral calculi. In general, patients are satisfied with treatment outcomes despite a large percentage of people reporting needing to have secondary procedures.
Introduction
T
As the Internet becomes more pervasive, its role in medicine will continue to expand. Initially used as a source of information for both patients and healthcare providers, it has developed into a medium for healthcare evaluations, access to personal health information, and a means of communication between the patient and their healthcare providers. 2,3 However, the medical research community has been slow to utilize this resource, with limited literature in most fields of medicine.
The field of urology is no exception. Despite the broad access to the general public that the Internet provides, there has only been limited use of the Internet in the urologic literature. Willard and Nguyen 4 and Breyer et al. 5 both used Google Insights to identify national epidemiologic trends in kidney stone incidence based on Internet searches. However, direct patient interaction through the Internet has been limited to targeted emailed surveys. A few groups sent targeted emails with links to online surveys to specific populations (medical students, 6 –9 Lesbian/Gay/Bisexual/Transgender [LGBT] population, 10,11 patients with overactive bladder [OAB] 12 ) based on patient lists obtained from a third party organization. Sebrow et al. sent emailed surveys to their own patient population, with a focus on post-prostatectomy quality of life. 13 There have not been, however, any prior studies looking at the feasibility of unsolicited Internet-based surveys.
In addition, despite the fact that the incidence of urolithiasis continues to increase in the United States and internationally, 14 –16 within the field of endourology and stone disease, there have been little to no published data on patient satisfaction after treatment of stone burden. What little has been published in this field has typically been limited to evaluation of a single treatment modality at a single institution. There have been no large volume assessments of patients' satisfaction with multiple treatment modalities of stone disease, and indeed, it is feasible that the anonymity of an Internet-based survey may provide a deeper insight into patient satisfaction, eliminating the physician-effect of the patients being reluctant to share adverse outcomes with their treating physician. There is a need for large patient population evaluation of urologic treatment of stone disease.
Materials and Methods
Survey
We utilized the website
All the questions were multiple choice focusing on the following: characteristics of stone burden, modality of treatment, reasons for pursuing specific treatment modalities, success and satisfaction with treatment modality, and what the individual liked and disliked about the treatment modality. The questions pertaining to success and satisfaction were scored on a five-point Likert scale.
Demographics
No identifying or demographic information was obtained from the survey respondents directly. Estimates of demographic information for overall visitors to the website were obtained using Quantcast software (Quantcast Corporation, San Francisco, CA). Quantcast reports that it generates demographic estimates using a combination of a javascript tag, which tracks visitors anonymously, and an inference model to characterize audiences.
Statistical analysis
Data were summarized with means and proportions. Chi-square and analysis of variance tests were used to identify significant associations between treatment modalities. Analysis was performed using STATA 12.1 (StataCorp, College Station, TX).
Results
Demographics
Based on data obtained by Quantcast.com, visitors to the website were more likely to be female (69%), college graduate (Bachelor's degree 45%, Graduate degree 16%), Caucasian (81%), and from the United States (72%). The peak age range of visitors was 35–44 years old (22%).
Response accrual
The survey had accrual of 443 responses in a 4.5-month time frame. As seen in Figure 1, the response accrual was steady during that time period, suggesting that had the survey been maintained, the responses would have continued to accrue.

Response accrual to online survey over time.
Survey responses
Table 1 highlights key patient responses to the survey questions.
IP=Internet Protocol; SWL=extracorporeal shock wave lithotripsy; PCNL=percutaneous nephrolithotomy.
The location of the stone burden was evenly split between the kidney (48%) and the ureter (46%).
The majority of individuals reported being treated ureteroscopically (46%), followed by extracorporeal shock wave lithotripsy (SWL, 25%) and percutaneous nephrolithotomy (PCNL, 7%). Other treatment modalities reported included spontaneous passage (13%), medical expulsive therapy (7%), and home remedies (2%).
When split by location of stone burden (Table 2), there is a shift in the treatment modality. For kidney stones, there is an equal usage of SWL (34%) and ureteroscopy (35%), and an 11% reported utilization of PCNL. For ureteral calculi, however, ureteroscopy is the predominant method of treatment, with 63% utilization—SWL (17%) and PCNL (4%) are much less commonly utilized.
URS=ureteroscopy; MET=Medical Expulsive Therapy.
The most common reason for choosing a treatment modality was physician recommendation (61%) or for highest chance of success (18%). When analyzed against treatment modality, physician recommended and highest chance of success correlated strongest with the more invasive procedures (PCNL and ureteroscopy), while least pain and safest treatment correlated with SWL.
The majority of respondents (64%) deemed their treatment “successful,” while 36% reported their treatment as either “partially successful” or “unsuccessful.” When analyzed against modality of treatment, as seen in Figure 2, unsuccessful treatment was more likely for SWL (17%) and home remedies (14%) (p=0.002). On the other hand, ureteroscopy and spontaneous passage had the highest rate of successful treatment (p=0.002).
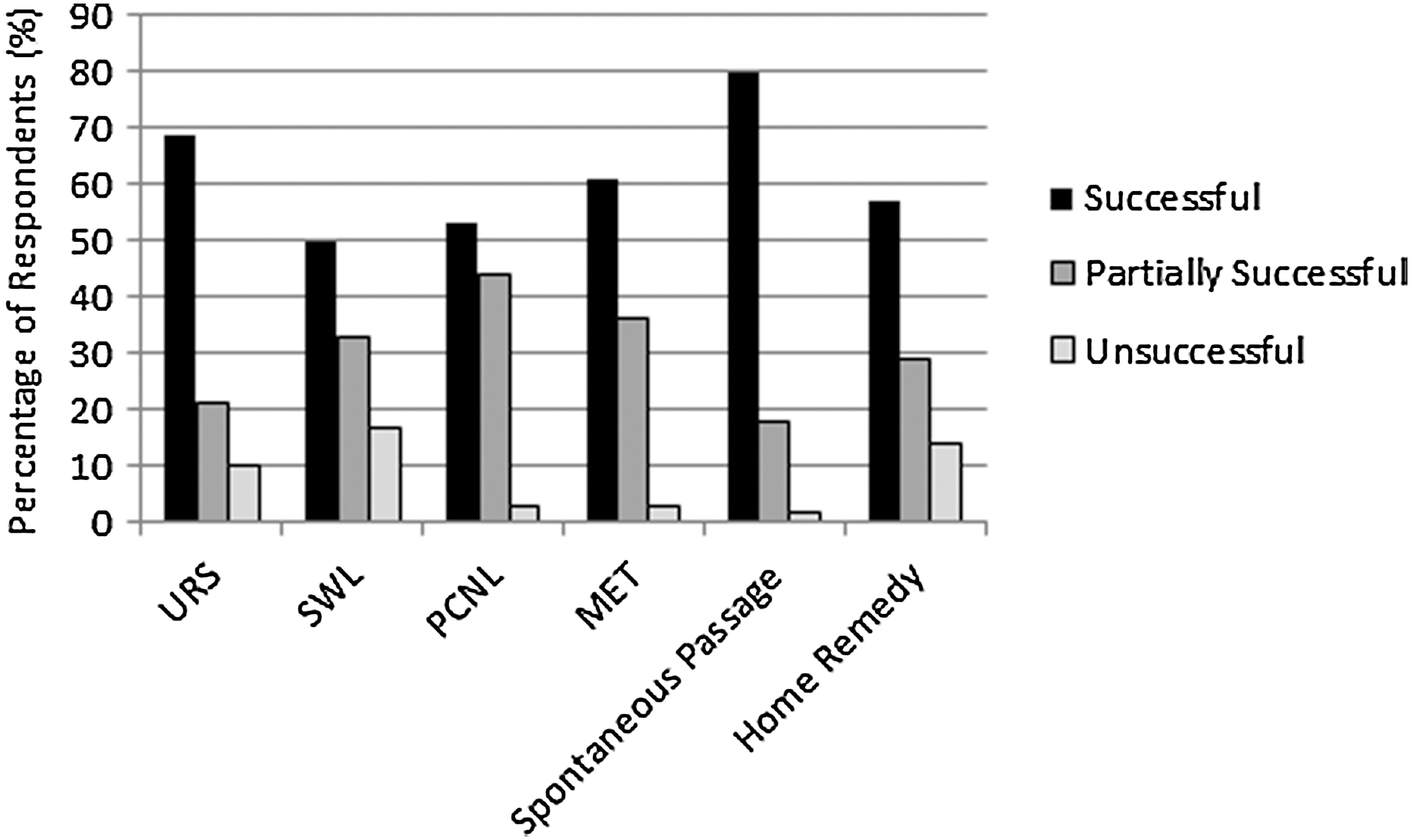
Success of urolithiasis treatment as defined by treatment modality.
Most respondents (52%) reported being either satisfied or very satisfied with their treatment choice. Satisfaction did not vary significantly by treatment type, but as seen in Table 3 was significantly associated with treatment success (mean satisfaction 3.8 for successful treatment vs 1.9 for unsuccessful treatment; p<0.0001).
Analysis of variance p<0.0001.
Along the same lines of treatment satisfaction, 55% reported either being “definitely” or “pretty likely” to choose the same treatment again. Likelihood did not vary significantly by treatment type. Figure 3 correlates dissatisfaction and unwillingness to repeat treatment modality, separated by treatment modality.

Percentage of respondents unsatisfied with treatment and unwilling to repeat treatment, by treatment modality.
When queried about what they liked most about their treatment modality, 51% stated the “success of treating stones.” Less commonly, people reported “avoiding surgery” (12%), “avoiding hospitalization” (13%), and “quick recovery” (12%).
On the other hand, when queried about what they liked least about their treatment modality, the responses were more varied. The most commonly reported complaints were the need for a stent (29%), delay in treatment (23%), and pain during recovery (18%) associated with their stone treatment.
Discussion
The purpose of this study was twofold: to assess the current management and effectiveness of urolithiasis in a large patient population (from the patient perspective) and to investigate the use of unsolicited Internet surveys as a medium for future population-based medical research.
Looking at the survey responses with relation to stone treatment specifically, we find that the responses regarding treatment modality correlate with recent literature. The growing predominance of the ureteroscopy as a treatment modality for urolithiasis is being established, 15,17 –19 and our data support ureteroscopic treatment predominance for ureteral stones. There is more of an even distribution of treatment modalities for treatment of renal calculi with 34% treated with SWL, 35% treated with ureteroscopy, and 11% treated with PCNL. For ureteral calculi, however, ureteroscopy appears to be the treatment modality of choice (63%), with SWL (17%) a distant second. However, there may be a component of selection bias that may not be accounted for—indeed, patients undergoing ureteroscopy may either be better informed (and have better access to the Internet and Internet-based surveys) or may have more stent or procedural discomfort (and therefore more likely to go to an Internet website dedicated to stone management).
As mentioned previously, there is a dearth of literature focusing on patient satisfaction following urolithiasis treatment. Based on these survey results, we found that the majority of patients deemed their stone treatment successful (64%), with a significant correlation to treatment type. Patients found the highest relative rate of success with ureteroscopy and spontaneous passage of stone burden and the least with SWL. When we then queried about treatment satisfaction, a majority of patients (52%) reported being satisfied with their treatment choice—but there was no correlation to treatment modality, only with treatment success. Ultimately, patient satisfaction is best predicted by success of treatment, not by treatment modality. This is corroborated by the fact that 55% of respondents reported being “definitely” or “pretty likely” to choose the same treatment again.
Physician recommendation was the strongest motivation for choosing a specific treatment modality, with 61% of respondents reported choosing their treatment modality for that reason. This is important to consider when counseling patients about treatment options, especially with regard to urolithiasis. Although an emphasis is placed on shared medical decision-making, physician bias may impact how a patient is counseled and ultimately what procedure is selected.
While there were no significant unexpected findings from the survey results, we did note that the absolute rates of patient satisfaction and success were lower than we expected. Prior reports focused mainly on success as dictated by the physician (usually in terms of effectiveness of stone clearance), with few rare reports in the literature looking at patient-reported success and satisfaction. This may explain the lower rates of satisfaction and success in our study, as this survey was from a patient perspective. Prior studies in other fields have established patient–physician discordance with regard to the management of chronic illness and postsurgical management. 20,21
Patient responses about their likes and dislikes about their management are also revealing. In concordance with our above findings, the most important aspect of their care that respondents liked—and the factor most important to them—was the success of their treatment. All other factors were much less important to most respondents—including factors such as length of hospitalization and speed of recovery, etc. However, the responses to the question focusing on patient dislikes were less homogenous—the need for stent, delay in treatment, and pain with recovery were all equally bothersome for patients. This provides us with insight regarding opportunities for improvement, with a focus on pain management, earlier access to treatment, and management of stent discomfort.
In the end, however, this survey is not a validated questionnaire. It is therefore difficult to make any broad statements about the nature of stone treatment based on these results alone. The main purpose of this study was to establish the Internet as a medium for future research and its ability to reach a larger patient population in a short period of time.
The Internet has become an integral part of the daily lives of patients and healthcare providers, playing a role in both education and delivery of healthcare. However, despite this growing role in other aspects of medical care, there has been limited use of this medium as a resource for research purposes. Within the field of urology, the use has been limited to use of Google Insight to track trends in Internet searches or to generate targeted surveys of preselected patient populations, typically other healthcare professionals. There have been no prior published data on the use of the medium to directly query the general population about treatment and satisfaction.
The accrual of 443 responses in a 4.5-month period for this survey demonstrates that using an Internet-mediated patient survey that is open to the general Internet traffic can generate a large-volume response in a short period of time.
While demographics were not obtained directly, the data from
Our study has its limitations as well. As can be expected, with any new medium, there are unique limitations and biases that need to be accounted for. However, just as with initial patient surveys done on paper, we need to establish validation of online surveys with further studies. Bernstein et al. have started this process by demonstrating that the online administration of the previously validated SHIM tool maintained validity. 22
In addition, there may potentially be a selection bias—individuals voluntarily submitting a survey on stone disease management on a website dedicated to stone disease may not represent the overall urolithiasis population. If anything, however, there is likely a bias toward patients who were unhappy with their stone management—so our response rates would underestimate the treatment success and satisfaction scores of the overall population. However, as the results for the management of stone disease correlated well with the published literature, it is unclear how much of a role selection bias actually plays.
Conclusion
Ultimately, despite its limitations, our findings establish that an unsolicited Internet-based survey can provide access to a large diverse demographic—and is a tool that should be utilized in future medical research. Further research needs to be done to validate surveys completed online to allow for substantive patient-centered evaluation of current treatment modalities for a variety of medical conditions.
Footnotes
Disclosure Statement
No competing financial interests exist.