
Abstract
Purpose:
To elucidate current practice patterns among Endourological Society members for acutely obstructing ureteral stones necessitating intervention.
Methods:
A practice pattern survey was sent to members of the Endourological Society using Survey Monkey. The following question stem was given: “Patient presents to the ER with acute renal colic and intractable pain, no signs of infection, i.e. afebrile and no pyuria. Stone is obstructing, and causing intractable pain; thus observation or medical expulsive therapy is not appropriate.” A follow-up stem was provided for specific scenarios: “Calculus measuring x mm at x location. What is your preferred management option?” The options given for immediate management included shockwave lithotripsy (SWL), ureteroscopy (URS), stent placement, or percutaneous management.
Results:
Four hundred and sixteen complete responses of approximately 2000 were received. There was a significant difference in management choice based on stone location (P<0.001) and stone size (P<0.001). URS was the predominant modality used for urgent treatment of acute proximal ureteral stones from 5, 10, and 15 mm except for calculi of 20 mm, where the preference was for percutaneous management. Immediate URS was the preferred choice for all distal and midureteral stones, regardless of size. The use of stents vs percutaneous nephrostomy drainage was similar (18% vs 16%, respectively) for proximally obstructing calculi, while stent insertion was preferred over nephrostomy for mid and distal stones.
Conclusions:
Current practice patterns among endourologists indicate a strong preference for immediate URS management over stent placement or SWL for acutely obstructing ureteral calculi. Not surprisingly, 20-mm stones in the proximal ureter had percutaneous management.
Introduction
T
In the ED, after identification of a stone, the patient must first be assessed for signs of infection before further management choices are made. When there is infection, the obvious first step is to decompress the obstruction with either a ureteral stent or nephrostomy tube (NT) and defer surgical treatment of the stone until resolution of the infection. If it is determined that there are no signs of infection, the next steps are to assess pain control and to rule out hydronephrosis and acute renal function impairment. When pain control is adequate with oral analgesics, medical expulsive therapy is an initial approach for ureteral calculi. Surgical intervention or admission, however, is needed when pain is intractable.
The focus of this study is to assess the management approach for patients with intractable pain in the absence of fever or infection. Because the choice of initial management may vary in these presentations, we developed a survey to elucidate current practice patterns in an effort to understand contemporary practice. We hypothesized that urologists will choose immediate treatment (with ureteroscopy [URS] or shockwave lithotripsy [SWL]) of the offending stone over deferred treatment with stent or NT placement in a noninfected case with intractable pain.
Methods
We constructed an online survey with Survey Monkey® and distributed it via e-mail to active members of the Endourological Society. We chose members of the Endourological Society because this reflects a group more likely to have some focus of stones in their practice, compared with members of the American Urological Association (AUA). The entire survey as sent is shown in Appendix 1. The survey was based on an initial question stem: “Patient presents to the ER with acute renal colic and intractable pain, no signs of infection, i.e. afebrile and no pyuria. Stone is obstructing, and causing intractable pain; thus observation or medical expulsive therapy (MET) is not appropriate,” and several scenarios for stone size and location were then given with inquiry into the preferred management.
The options given for immediate management included SWL, URS, stent placement, or percutaneous management. Using e-mail addresses in the Endourological Society's member database, the survey was sent twice, spaced 3 to 4 weeks apart. The responses were anonymized and tabulated, and statistical analysis was performed with cross-tabular and pairwise comparisons with SPSS using chi-square, Fisher exact and pairwise t tests.
Results
Four hundred and sixteen complete responses of 2000 sent e-mails were received. All respondents were active members of the Endourological Society. In the interest of compliance with the survey, we did not collect demographic or practice setting information, and we also believed all respondents would have an approach regardless of background.
The data were categorized by stone size and stone location (Table 1 and Fig. 1 A–D). For distal ureteral stones regardless of stone size, >80% of respondents performed URS as immediate management. For midureteral stones, URS management fell to 70%, with relatively more respondents performing SWL or ureteral stent placement. There were more variations in the management of proximal ureteral stones. URS was the predominant modality for proximal ureteral stones from 5, 10, and 15 mm except for calculi of 20 mm, where the preference was for percutaneous management. More specifically, for proximal stones, URS and SWL were equally preferred for stones <10 mm at 42% and 40%, respectively. Immediate URS was the preferred choice for all distal and midureteral stones, regardless of size. The use of stents vs percutaneous nephrostomy drainage was similar (18% vs 16%, respectively) for proximally obstructing calculi, while stent insertion was preferred over NT for mid and distal stones.
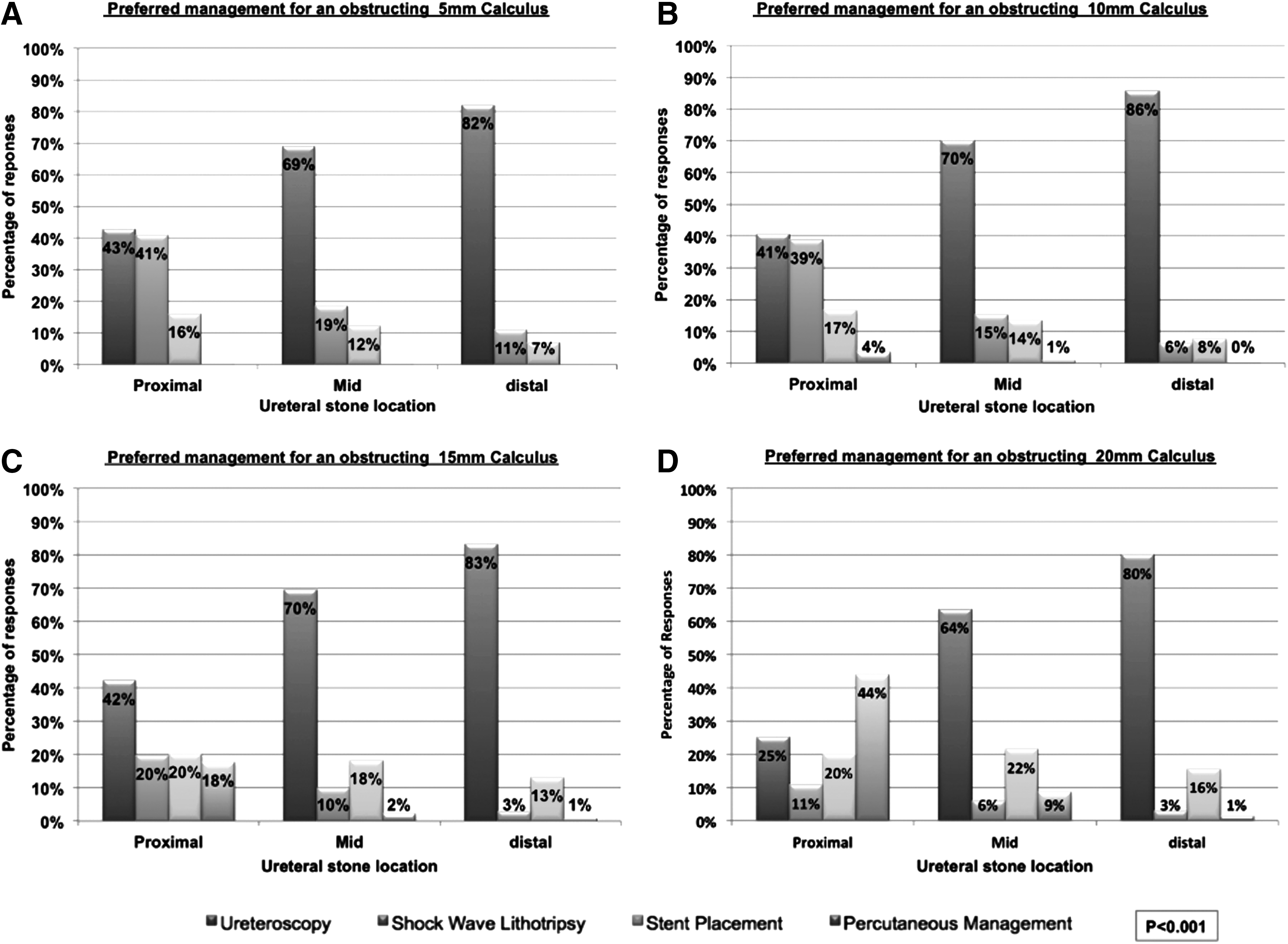
Preferred management choice categorized by stone size and location.
NT=nephrostomy tube; SWL=shockwave lithotripsy; URS=ureteroscopy.
There was a significant difference in management choice based on stone location (P<0.001). For all proximal stones combined, URS was preferred by 38%, SWL in 28%, while ureteral stents and NT were chosen by 18% and 16%, respectively. For midureteral stones, 68% chose to perform URS, followed by 16% for stent placement, 12% for SWL, and 3% for NT. For distal stones, 83% chose URS, 11% chose stent placement, 6% chose SWL, while 1% chose a NT.
Similarly, differences were observed when choices were stratified by stone size irrespective of location (P<0.001). For 5-mm calculi, 65% chose URS, while 24% and 12% chose SWL and stent placement, respectively; none chose NT placement. For 10-mm calculi, the trend was similar, with 66% choosing URS, 20% for SWL, 13% for stent placement, and 2% for NT. In the 15-mm stone category, 65% chose URS, 17% chose stent placement, while 11% chose SWL, and 7% chose NT placement. Finally, for 20-mm stones, the choice for URS dropped to 56%, while only 7% chose SWL. There was a stronger tendency to place a stent or NT at 19% and 18%, respectively.
Discussion
Given the prevalence of renal colic, it is important to know how these patients are treated in the acute setting for an obstructing stone. The diagnosis of an obstructing stone is often made through diagnostic imaging in the ED before urologic intervention. After initial workup and management has been established in the ED with fluid replenishment and pain control, decisions regarding stone management are formulated based on clinical context and surgeon preference.
There is often variability in the management choices in an acute episode of renal colic with intractable pain. In the patient with fever or infection with a coexisting stone, there is very little debate because the vital step in treatment is administration of antibiotics and relieving the obstruction with either a ureteral stent or NT. Patients in this setting can have a ureteral stent placed in the operating room or in the clinic under local anesthesia. 6 If the patient is clinically stable without fever or infection, however, there are more potential treatment options, which include immediate URS or SWL, or stent/NT placement±MET for deferred surgical management of the stone. 7
According to the current AUA guidelines for the management of ureteral stones, both SWL and URS are excellent first-line options for calculi in any location of the ureter. While no differences in overall stone-free rate (SFR) were found between SWL and URS with ureteral stones, the only instance in which SWL yielded slightly better SFRs was for proximal ureteral stones <10 mm, while URS had superior SFRs for proximal stones >10 mm, and distal stones of any size. For all midureteral stones, URS trended toward greater SFRs but did not reach statistical significance. 8
In our survey, we elucidated that for all distal calculi, regardless of size, >80% of urologists preferred to perform URS, which is congruent with the superior SFR outcomes as outlined in the guidelines. Similarly, in keeping with the guideline recommendations, in the proximal ureteral calculi group, both URS and SWL were performed equally for 5- or 10-mm stones, but a negative correlation was noted with SWL use and stone size in stones >10 mm. Although there was a similar use of ureteral stents and NT for all proximal stones combined, there was a positive correlation with stone size or proximity and preference for NT, with 44% choosing NT as the initial step in management for large proximal stones >20 mm (Figs. 2, 3), presumably for future percutaneous nephrolithotomy or antegrade URS. SWL was the least popular approach for large calculi >20 mm and in distal calculi (Figs. 2, 3). In all scenarios except large proximal stones, however, URS remained the preferred choice.
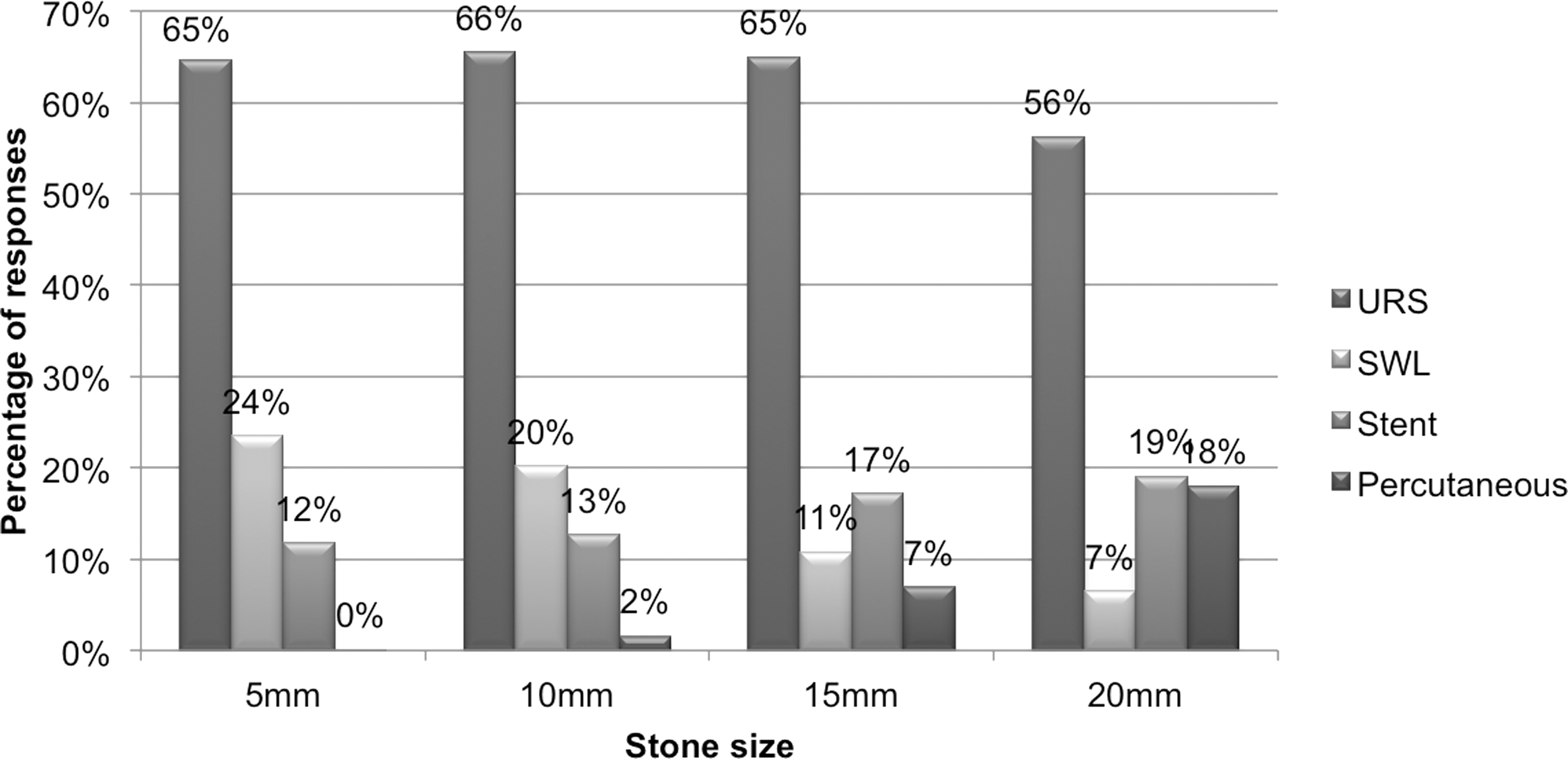
Treatment preference categorized by stone size. SWL=shockwave lithotripsy; URS=ureteroscopy.

Treatment preference categorized by stone location.
Most respondents offered immediate surgical management rather than stent placement in the acute setting. Despite the perceived theoretical advantage to stent placement and deferred surgery, our survey indicates that most urologists attempt immediate URS to treat the offending stone. This is perhaps a reflection of improved endoscopic equipment that facilitates URS in an acute setting. In addition, there is recent evidence supporting immediate URS in an emergency setting to be safe and efficacious compared with delayed treatment. 9 –11 Regarding stent placement, the impact of preoperative stent placement has shown equivocal results, with some studies showing no clear advantage, 12 while others show a significant benefit. 13,14
A limitation of this study is the relatively low response rate of 21% (416 participants); we suspect that many of the listed e-mails within the Endourological Society's directory are duplicate and potentially outdated. Nonetheless, among the 416 respondents, significant noteworthy trends were observed. This assessment of the emergency management of ureteral calculi when intervention is needed is encouraging, given that the management choices of respondents are consistent with the evidence-based recommendations of the current ureteral stone guidelines.
Conclusion
Our survey indicates strong concordance with the ureteral stone guidelines in the practices of Endourological Society members. Our survey suggests that endourologists may prefer immediate over delayed treatment for acutely obstructing ureteral stones. Further studies are needed to assess outcomes and complications of each approach.
Disclosure Statement
No competing financial interests exist.
Footnotes
Abbreviations Used
Appendix 1. Survey Template
Patient presents to the ER with acute renal colic and intractable pain, no signs of infection, i.e., AFEBRILE and NO pyuria. Stone is obstructing, and causing intractable pain; thus observation or MET is not appropriate.
Of the following options, please select your preferred management for each of the scenarios: