
Abstract
Introduction:
There has been a significant change in surgical treatment of benign prostatic hypertrophy (BPH) over the last two decades. Most importantly, laser surgery (coagulation, vaporization, or enucleation) has been growing in popularity as an alternative to standard transurethral prostatectomy (TURP) or other procedures. Our goal was to analyze the trends of BPH surgeries and compare outcomes of laser surgery to TURP, the two most common alternative surgeries.
Materials and Methods:
We used the New York Statewide Planning and Research Cooperation System (SPARCS) data to identify patients diagnosed as having BPH who underwent BPH-related surgery from October 2000 to December 2011. Age, insurance, individual comorbidities, and average hospital volumes were assessed. Bivariate and multivariate regression models were used to analyze predictors of laser use. In-hospital outcomes were then compared between laser and TURP in a balanced propensity-matched cohort.
Results:
Ninety thousand six hundred seventy patients underwent BPH surgery. Laser surgery usage increased from 6.4% to 44.5% over 10 years (p<0.0001). TURP declined significantly from 72.2% to 48.3% (p<0.0001). Patients with Medicaid were less likely to undergo laser therapy than those with private insurance (odds ratio [OR]: 0.58, 95% confidence interval [CI]: 0.48, 0.69). Mid- and high-volume institutions were more likely to use laser treatment than low-volume centers (OR: 2.26, 95% CI: 1.22, 4.2; OR: 4.07, 95% CI: 1.75, 9.46, respectively). In the matched cohort, both laser and TURP patients had similar complication rates with more frequent electrolyte disorders in TURP patients (2.9% vs 2.3%, p=0.001).
Conclusions:
TURP remains the most common procedure. However, the rate of use has declined over time. In contrast, laser use has significantly increased. Laser treatment was utilized more in younger patients, in those privately insured, in hospitals with high volumes of BPH procedures, and in patients with fewer comorbid conditions. Both surgeries are safe with no differences in terms of occurrences of morbidity and complications.
Introduction
T
The introduction of novel, minimally invasive BPH surgeries has occurred over the last two decades. This arose due to the need to improve upon the efficiency and morbidity of the standard TURP. Limited prior evidence suggests that TURP rates have decreased and other procedures have increased in usage. 6 –8
Understanding the trends of BPH-related procedures on a state and regional level is important in evaluating how we can improve upon delivery of high-quality health care more efficiently and more cost-effectively. In addition, observing trends over time and related changes in outcomes can help us identify dynamic associations and deficits in our delivery of care to our patients. 9 Accordingly, we sought to determine trends, safety, and utilization of surgical treatments for BPH over time in the state of New York.
Materials and Methods
The New York Statewide Planning and Research Cooperation System (SPARCS) is a collection of patient-level details from every hospital discharge and ambulatory surgery patient in New York State. Its current format, available since 1994, contains patient demographics, diagnoses, procedures, and statuses from every hospital discharge and ambulatory surgery patient in New York State. 10 All patients from October 1, 2000 to December 31, 2011 who were treated in a hospital inpatient or outpatient ambulatory surgery center for a diagnosis of benign prostatic hyperplasia (BPH) were initially included in our study, excluding those with a history of prostate cancer. Those who were treated with laser coagulation, vaporization, or enucleation of the prostate (Laser), TURP, TUMT, TUNA, open prostatectomy (Open), or radical and other prostatectomy (Other) as determined by CPT-4 and International Classification of Diseases, 9th revision (ICD-9-CM) procedure codes make up our surgically treated sample.
Patient age on the procedure date (<45, 45–65, 65–75, 75+ years) and patient race (White, Black, Other Race) were provided by SPARCS, as well as insurance type (Private, Medicare, Medicaid, Other) and year of treatment. We assessed individual comorbidities (congestive heart failure, renal failure, chronic pulmonary disease, cerebrovascular disease, hypertension, diabetes, obesity, depression, coronary artery disease) and a comorbidity score based on validated ICD-9 coding algorithms 11,12 using patient claims from the procedure date and year before surgery. Additionally, we grouped hospitals by their average annual volume of BPH procedures (low: 0–100 cases, med: 100–200 cases, high 200+ cases) (Table 1).
TURP=transurethral prostatectomy.
Temporal trends were analyzed over time both graphically and with Cochran–Mantel–Haenzel χ 2 tests. Percentages of laser utilization by patient age, comorbidity, and hospital volume were further examined graphically. To determine factors that influence laser utilization, we used bi- and multivariate mixed-effects logistic regression models with a random facility-level intercept to account for clustering of patients in hospitals. Bivariate models included only the factor of interest, whereas the multivariate model included all factors under consideration. Resulting odds ratios are presented with 95% confidence intervals (CIs). Additionally, the percentage of laser utilization (with 95% CI) is presented graphically at a hospital level in 2000, 2001, and 2011 to illustrate this variation.
We also compared the safety of laser to TURP, the two most popular surgical treatments for BPH. A propensity score for the probability of being treated with laser was created using logistic regression with potential confounding patient demographic and hospital variables. χ 2 tests and Cochran–Mantel–Haenzel χ 2 tests are used to detect differences in outcomes for the paired data. We then created a balanced cohort using a one-to-one nearest neighbor matching algorithm, which pairs patients who have the closest propensity score within a defined limit or caliper. 13 The logit of the propensity score was used for matching with a caliper of 0.2 times its standard deviation as recommended by Austin. 14 Outcomes of interest were in-hospital mortality rate, a composite outcome of mortality rate, stroke, and myocardial infarction, cardiovascular, pulmonary, infectious, iatrogenic, and urinary complications, as well as electrolyte disorders. Differences between groups are assessed using χ 2 tests and analogous Cochran–Mantel–Haenzel χ 2 tests for paired data in the matched cohort.
Results
There were 1,027,775 patients evaluated for BPH and 90,670 were treated surgically in New York State from October 1, 2000 to December 31, 2011. In the overall sample, TURP was used in 58.3% of procedures, Laser in 21.3%, TUMT in 0.1%, TUNA in 0.4%, open surgery in 5.2%, and other in 14.7%. Laser was the most rapidly increasing method of treating BPH, growing from 6.4% in 2000 to 2002 to 44.5% in 2009 to 2011 (p<0.0001). At the same time, the use of TURP has declined significantly from 72.2% in 2000 to 2002 to 48.3% in 2009 to 2011 (p<0.0001). Open prostatectomies decreased from 6.6% in 2000 to 2002 to 3.6% in 2009 to 2011. Procedure utilization and trends over time are shown in Figure 1.
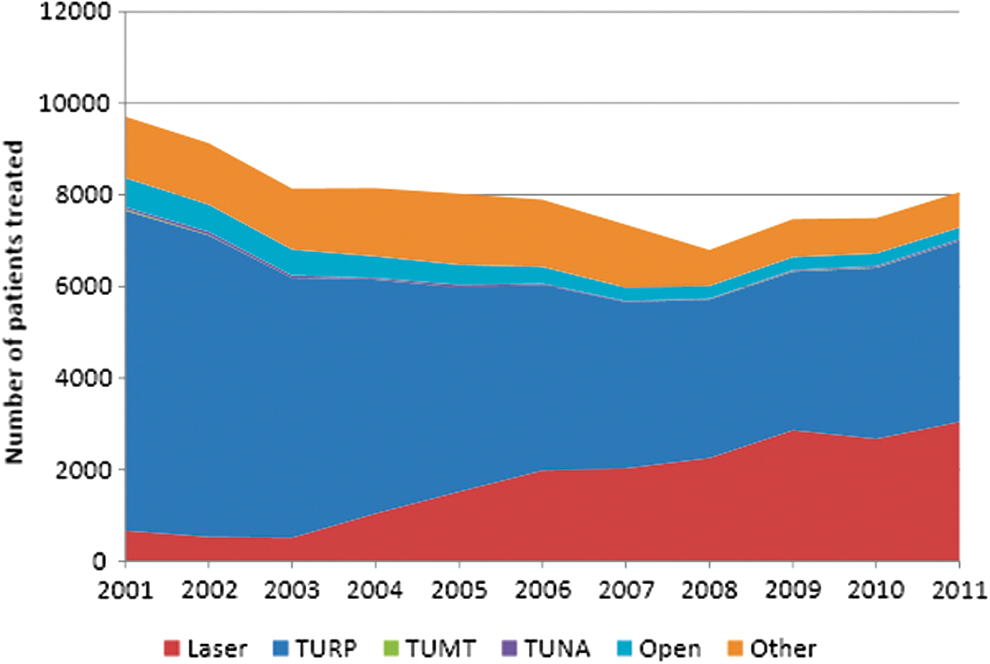
Cumulative number of patients diagnosed as having benign prostatic hyperplasia (BPH) who were treated surgically as indicated below in New York State from 2001 to 2011. TUMT, transurethral microwave thermotherapy; TUNA, transurethral needle ablation; TURP, transurethral prostatectomy.
When adjusting for patient and hospital factors simultaneously, patients older than 45 were progressively less likely to be treated with laser (Table 2). Patients with Medicaid were less likely than those with private insurance to be treated with laser surgery (odds ratio [OR]: 0.58, 95% CI: 0.48, 0.69). However, Medicare patients were more likely (OR: 1.06, 95% CI: 1.01, 1.12) to be treated with laser surgery. Mid- and high-volume institutions were also more likely to use a laser treatment than low-volume institutions (OR: 2.26, 95% CI: 1.22, 4.2; OR: 4.07, 95% CI: 1.75, 9.46, respectively). Patients with many of the considered comorbidities were found to be less likely to receive laser treatment, including renal failure (OR: 0.57, 95% CI: 0.51, 0.65), cerebrovascular disease (OR: 0.6, 95% CI: 0.45, 0.8), hypertension (OR: 0.83, 95% CI: 0.79, 0.86), obesity (OR: 0.84, 95% CI: 0.73, 0.96), depression (OR: 0.82, 95% CI: 0.73, 0.92), and coronary artery disease (OR: 0.92, 95% CI: 0.87, 0.97).
All models include a random hospital-level intercept.
Unknown category introduced for multivariate model to replace missing values, estimates not shown.
Seven percent missing.
Fifteen percent missing.
CI=confidence interval.
Over time, utilization across age groups has remained constant, whereas high-volume institutions began using the laser more rapidly than low- and mid-volume facilities, and laser treatment was adopted more rapidly for patients with a lower comorbidity score (Fig. 2). Additionally, uptake of laser appears to differ greatly at a hospital level (multivariate model random intercept variation across facilities=3.288, standard error=0.4002). Figure 3 depicts utilization at an institutional level in three distinct years of our study.
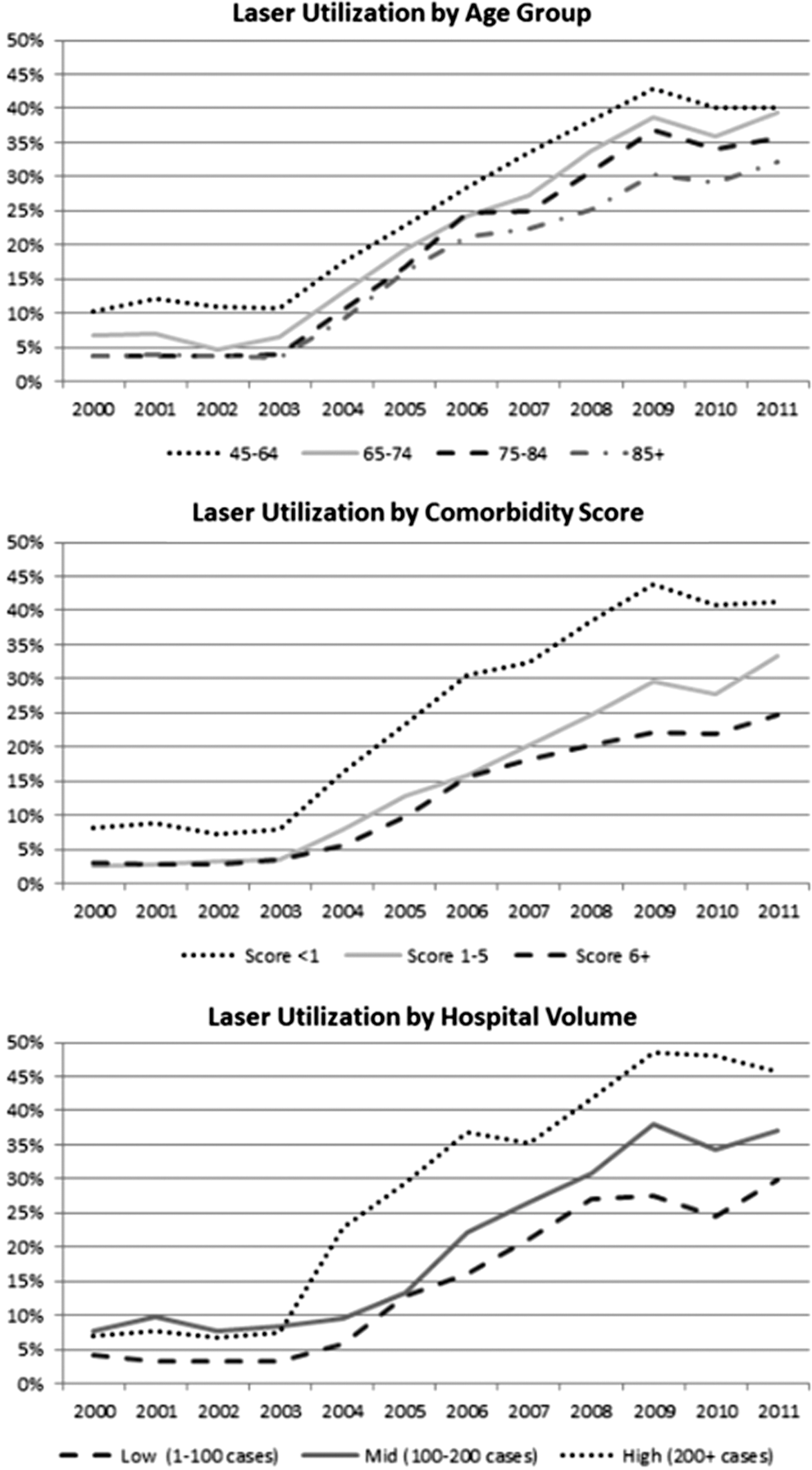
Percentage of patients who were treated surgically for BPH in New York State from 2000 to 2011 by age group, hospital volume, and Elixhauser comorbidity score.
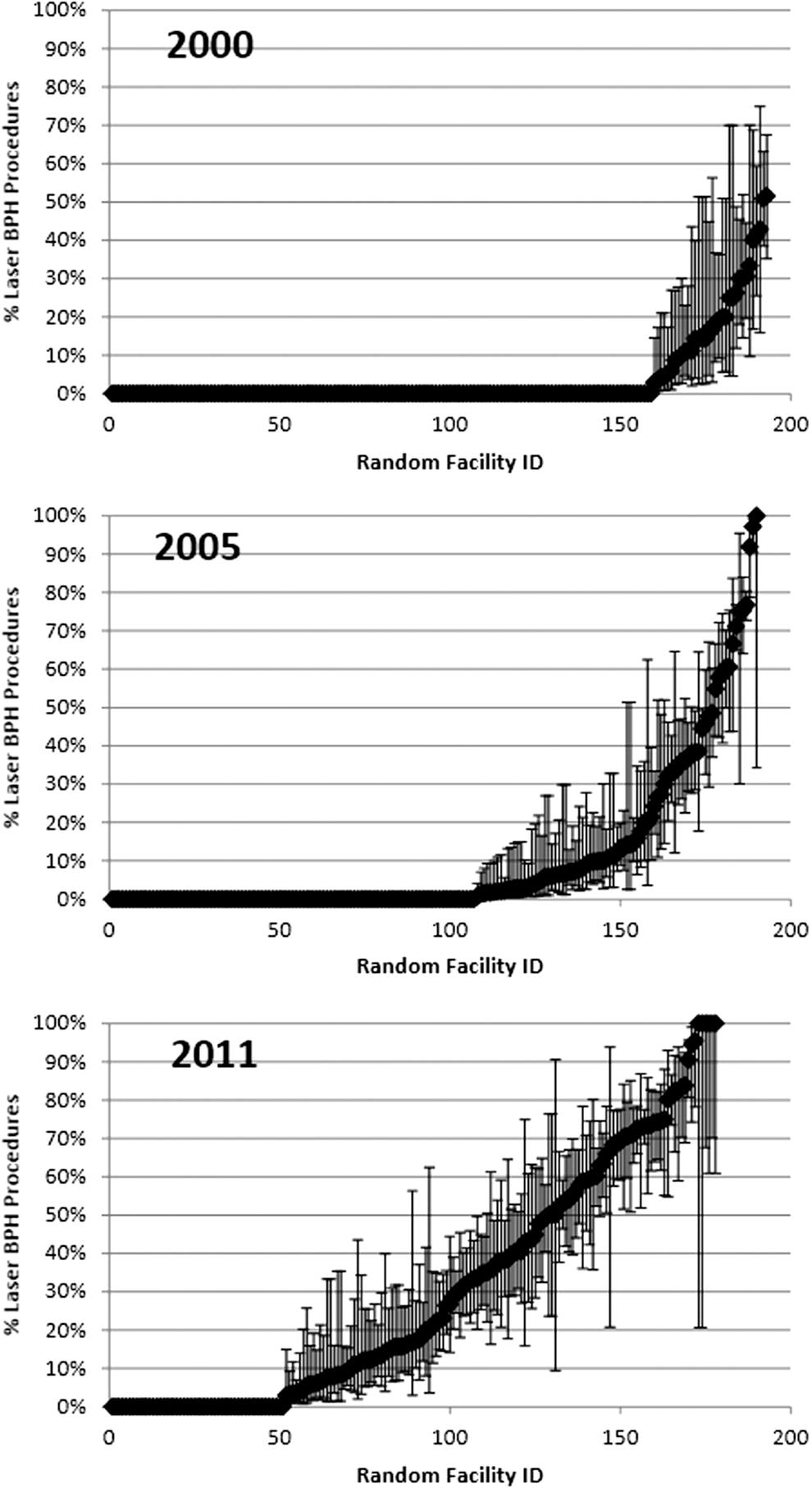
Uptake of laser (% of surgical BPH patients treated) within each hospital in 2000, 2005, and 2011.
In the focused, propensity score-matched comparative analysis of patients treated with laser versus TURP, we found that both laser and TURP patients have similarly low occurrence of in-hospital mortality rate and major complications, which include urinary retention, incontinence, and strictures. There were significantly lower electrolyte disorders in the patients treated with laser (2.9% vs 2.3%, p=0.001) (Table 3). For both laser and TURP patients, the reoperation rate was 0.1% in the time frame that we analyzed.
Stroke, myocardial infarction, or death.
Discussion
We present the largest population cohort study to date, representing one of the largest states in the country. We report that TURP remains the most common treatment to treat BPH, but the use declined over the last decade from 72.2% in 2000 to 2002 to 48.3% in 2009 to 2011 (p<0.0001). Using Medicare data, Malaeb et al. 6,7 also reported declining rates of usage of TURP in the elderly patients. The study reported that use of laser therapy in the elderly increased by 51.1% on a national level. In our current study examining patients of all age groups, laser prostatectomy was also found to be a rapidly increasing modality for treatment of BPH with 6.4% in 2000 to 2002 to 44.5% in 2009 to 2011 (p<0.0001). A recent Canadian study by Hueber and Zorn also reported an overall progressively growing trend of minimally invasive laser procedure alternatives to TURP. 8
Laser surgery and other new technologies continue to change the landscape of BPH-related procedures. As TURP has been the gold standard for surgical treatment of BPH, there is need to understand if new technologies such as laser prostatectomy can be as safe as TURP. Our study provides supportive evidence that laser and TURP have similar in-hospital morbidity as well as low occurrence of complications. In a randomized study, including 120 patients, that compared laser vaporization with TURP, Al-Ansari et al. 15 demonstrated similar outcomes in terms of symptom improvement and urinary flow. 15 Additionally, there are a number of other randomized clinical trials (RCTs) that provide evidence that TURP and laser therapies offer similar outcomes. 16 –18 Most recently, a study from Canada by Bhojani et al. used American College of Surgeons National Surgical Quality Improvement Program Database (ACS-NSQIP; 2006–2011) and found no differences in outcomes among TURP or laser treatments (enucleation or vaporization). 19 Our study is from a large state that is all inclusive and captures patients of all socioeconomic levels with hospitals ranging from public to private. Our cohort is representative of real-world care over the past 12 years and should be reassuring for surgeons and patients. We confirm and advance prior evidence that laser and TURP are equivalent from a safety perspective.
The use of laser modalities was found in our study to be associated with age, private insurance, Medicare coverage, hospital volume, and comorbidities. It is important to highlight that Medicaid patients were least likely to be treated with laser therapy. These findings are consistent with the findings from Schroeck et al., 20 where they found a differential adoption of laser technology for treatment of BPH in Florida (2001–2009) in 114 health care markets based on the socioeconomic environment. We substantiate prior evidence that disadvantaged socioeconomic patient groups are less likely to get new laser technologies. In our study, Medicaid patients were evenly distributed throughout the state, type of hospital, and volume of procedures. No clear discrepancy could be identified.
Our study also demonstrated a rapid adoption of laser therapy by high-volume hospitals, defined as having greater than 200 BPH cases per year. There are no other studies that addressed this question. It is unclear if the reduced use of laser therapy in lower volume hospitals was related to surgeon preference/training or whether it was related to availability of laser therapy. The most likely reason is that high-volume hospitals have more resources, are more likely to adopt new technologies, and therefore would have more access and training in the use of laser technology.
We also found that older patients and those with comorbid conditions were less likely to be treated with laser. This is an interesting observation since laser therapy is minimally invasive and there is evidence that it is safe and effective in patients who are at high risk for surgical complications, such as the elderly and in those who require anticoagulation therapy. 21 –23 It is unclear if some surgeons are still concerned about safety and prefer to use laser in younger and healthier patients or whether this phenomenon was related to patient preferences. We believe that the former is a more likely explanation and surgeon concerns/inexperience in using a new technology is at least partially related to this observation. Most likely, the reason why we see this trend is that our data are reflective of the beginning of laser therapy when surgeons are getting used to a new technology. Perhaps, if we evaluate a more contemporary cohort where surgeons have gained more expertise and experience with laser technology, we will see more older patients with comorbid conditions who have been treated with laser therapy.
Limitation
There may be several factors that can affect the differential usage of laser treatments, which cannot be captured in our study. One limitation of our study was that we were unable to distinguish among the various laser modalities, coagulation, enucleation, or vaporization. Another limitation is that we were unable to differentiate between monopolar and bipolar TURP. Although we were also able to comment on the safety of laser and TURP treatments, we were unable to capture or classify the specific nature of the complications or when they occurred.
Conclusion
TURP remains the most common treatment overall. However, TURP is currently declining, whereas laser-based alternatives have significantly increased in terms of utilization. We found that younger age, privately insured or Medicare status, greater surgical volume of BPH, and having fewer comorbidities were more often associated with use of laser surgery. Patients with laser therapy had outcomes similar to those who underwent TURP in the real-world settings.
Footnotes
Acknowledgments
The authors thank the WCMC Male Health Center (Director Steve Kaplan) and Patient-Centered Comparative Effectiveness Program/US FDA's Medical Device Epidemiology Network's (MDEpiNet) Science and Infrastructure Center (Director: Art Sedrakyan, MD, PhD). The Center is a collaborative entity jointly funded by the US Food and Drug Administration and Departments of Urology, Vascular Surgery, and Cardiothoracic Surgery to advance the comparative effectiveness, quality, and regulatory science for devices and surgical procedures. Bilal I. Chughtai, MD, is a urologist and senior investigator/clinical codirector within the Center.
Disclosure Statement
No competing financial interests exist.