
Abstract
Purpose:
Robot-assisted sacral colpopexy (RASC) utilization trends and influencing factors were examined. RASCs were compared with nonrobotic vaginal suspension procedures (non-RASC) used to treat patients with vaginal prolapse. Hospital costs associated with each approach were also examined. The presence of certain factors may predict increased use of RASC.
Methods:
The National (Nationwide) Inpatient Sample database was queried from 2009 to 2011 to identify patients undergoing RASC and non-RASC. Multivariable logistic regression was used to evaluate variables associated with RASC utilization, adjusting for age, comorbidities, concurrent procedures, hospital region, primary payer, and year. Multiple linear regression was used to evaluate variables associated with hospital costs when adjusting for operative approach, concurrent procedures, comorbidities, presence of complications, hospital region, and year.
Results:
Of the 125,869 patients who underwent vaginal vault suspension of any type, 14,601 (12%) were RASC. Total in-hospital complication rates were similar between RASC and non-RASC (8% RASC, 7% non-RASC, P=0.360). The proportion of patients undergoing RASC increased throughout the study period (odds ratio [OR] 1.58, P<0.001), with this increase being most pronounced in the South (OR 2.22, P<0.001). Fifty-four percent of RASC patients vs 48% of non-RASC patients underwent concurrent hysterectomy (P=0.007). Patients with private insurance (OR 1.73, P=0.001) or Medicare (OR 1.43, P=0.033) as their primary payer were at significantly increased odds of RASC compared with Medicaid patients, and private insurance was associated with increased reimbursement. On multiple linear regression, RASC was independently associated with a $4825 increase in hospital costs (95% confidence interval $4161–$5490, P<0.001). There were independent regional differences in cost associated with vaginal suspension, with the West being the most expensive (P<0.001).
Conclusion:
While RASC utilization increased over the study period as a treatment option for vaginal prolapse, the majority of vaginal suspension procedures were still performed via non-RASC methods. RASC was associated with equivalent complications yet significantly higher costs.
Introduction
L
Increased degrees of articulation along with three-dimensional imaging 5,6 afforded by use of robot assistance have dramatically eased the barrier to entry for surgeons training in minimally invasive surgery. Indeed, in examining the learning curve of robot-assisted laparoscopic sacral colpopexy (RASC), multiple studies report significant reductions in operative time after completion of a surgeon's first 10 cases, with Akl and associates 5 noting that mean operative time decreased by 25% and Geller and colleagues 7 reporting a decrease in median operative time of more than an hour. Furthermore, review and meta-analysis by Serati and coworkers 4 reveals no significant difference in severe complications or objective cure rate after laparoscopic sacral colpopexy vs RASC.
Given the opportunity to offer patients similar benefits with a shorter learning curve, many surgeons performing vaginal suspension have begun to incorporate robot assistance in their practice. Because of a paucity of research examining regional patterns in utilization of RASC, little is known as to whether access to this new technology is equally distributed among those whom it could benefit. We hypothesize that certain regions will adopt this technique faster because of a number of variables: Primary payer, university setting, and patient age and comorbidities, to name a few. To investigate this hypothesis further, the objective of our study was to explore the factors influencing regional uptake and utilization of RASC using data from the National (Nationwide) Inpatient Sample (NIS). Because utilization is so closely tied to costs, our secondary objective was to examine hospital costs related to RASC.
Methods
Database and patients
The NIS, made available from the Healthcare Cost and Utilization Project (HCUP) of the Agency for Healthcare Research and Quality in the United States (US), is an administrative database with capture of 20% of all US inpatient hospitalizations annually. 8 Using NIS, only data from the index hospitalization are included. Any readmission or posthospital complication associated with an operation is not identifiable. International Classification of Disease version 9 (ICD-9) hospital codes are used to identify diseases and procedures. 8 HCUP provides discharge weights that generate national estimates of patients undergoing inpatient procedures. HCUP also provides hospital specific cost-to-charge ratios that are used to calculate the cost associated with the hospitalization, excluding physician fees. 9
Using 2009 to 2011 NIS database files, we identified all adult (>17 years) patients undergoing vaginal suspension using ICD-9 codes 70.77 and 70.78. We determined surgical approach using ICD-9 17.4x for robot assistance and 54.21 and 54.51 for the laparoscopic approach. Because the ICD-9 coding system does not contain individual codes for each of the specific procedures of interest, some assumptions were made about the other procedures captured by this method. Accordingly, all cases without modifiers were considered vaginal or open vaginal vault suspension procedures such as vaginal sacrospinous ligament fixation, vaginal uterosacral ligament suspension, or open sacral colpopexy. Data analysis was limited to the 2009 to 2011 NIS data because robotic coding was not available until the final quarter of 2008.
Laparoscopic cases (n=3808) represented fewer than 5% of cases in each region each year, and, because of variability in physician coding practices, it was uncertain whether these cases represented true robot assistance or traditional laparoscopy. To limit our focus only to changes in robotic utilization, these cases were eliminated from analysis. Variables were assessed for completeness, and only race and cost had more than 5% of data missing (certain states do not report race). To account for missing 17% of race data, we included race in descriptive analyses but excluded it from regression analyses. Cost was missing for 10%; however, because cost was missing nondifferentially from specific institutions (not entire states or regions), we included it as the outcome of a multiple linear regression model as described below.
Outcomes and variables
The primary outcome of interest was identifying factors that affect regional utilization of RASC. The secondary outcome was identifying factors affecting hospital costs associated with RASC. Patient-specific variables included demographic characteristics, median zip-code income quartile, and Charlson Comorbidity Index (CCI). Because median zip-code income quartile was significantly correlated with primary payer (κ=0.072, P<0.001), primary payer was used in the majority of analyses. It is important to note that Medicare is a federal national health insurance plan available to all US citizens age 65 and above, as well as those meeting certain qualifying factors such as a medical disability. US Medicaid is a state- and federal-funded health insurance plan for those persons having income below a certain threshold based on the federal poverty level. Hospital variables were region and teaching status.
Inpatient characteristics included concurrent procedures (sling or hysterectomy), primary payer, length of stay (LOS), complications, total charges, and hospital cost. CCI was generated using the methods of Deyo and associates 10 and was categorized as 0, 1, or ≥2 comorbidities. Complications, although not explicitly captured by the NIS database, were identified using ICD-9 codes 997.x-999.x, 560.81, 568.0, 518.x, 415.11, 593.3, 598.2, 338.18, 512.1, and 458.29 as described previously. 11 A more detailed description of variables is available through NIS. 8
Statistical analyses
Statistical analysis performed by author MFM used descriptive comparisons between RASC and non-RASC using the Pearson chi-square test, Student t test, and the Mann-Whitney test, as appropriate. In addition, a multivariable logistic regression model was created assessing the relationship between patient-specific variables, hospital variables, and operative approach. Variables included age, CCI, concurrent procedures, hospital region, primary payer, and year of operation. A multiple linear regression model was created to assess the impact of the robotic approach on hospital costs, adjusting for CCI, concurrent procedures, in-hospital complications, hospital region, and year of operation.
Generalized estimating equations were used to address confounding from multiple cases reported from individual institutions and year. A priori, we accepted P<0.05 as statistical significance. All statistical analyses were performed using Stata version 12.1 (StataCorp LP., College Station, TX). Institutional Review Board exempt status was granted for the conduct of this unfunded study.
Results
There were 125,869 patients who underwent vaginal vault suspension from 2009 to 2011, and 13% of the operations were performed with robot assistance (Table 1). The number of robotic cases increased, with 3195 in 2009, 4514 in 2010, and 6894 in 2011. Non-RASC cases were 38,545, 38,744, and 33,976, respectively. Sixty-eight percent of RASC and 55% of non-RASC were performed on patients living among the highest income brackets (P<0.001). Medicaid and private insurance were the most common primary payers for RASC and non-RASC. More than one-third of both RASC and non-RASC procedures were performed in the South (Table 1). Overall, 93% of patients were considered to have no comorbidities by the adapted CCI.
P values reflect Pearson chi-square test, Mann-Whitney test, and Students t test.
Race missing for 17% of patients.
RASC=robot-assisted laparoscopic sacral colpopexy; SD=standard deviation.
As shown in Table 2, 48% of non-RASC patients underwent concurrent hysterectomy and 11% received concurrent sling placement. A significantly higher proportion of the RASC patients underwent concurrent hysterectomy (P=0.007). Examining within individual regions, there was no difference in the proportion undergoing concurrent sling (12% Northeast, 10% Midwest, 10% South, 11% West). There were regional differences noted, however, in the proportion of patients undergoing concurrent hysterectomy (54% Northeast, 51% Midwest, 44% South, 47% West, P<0.001). This difference was more striking when examining concurrent hysterectomy rates just among the RASC patients (71% Northeast, 51% Midwest, 51% South, 46% West; P<0.001).
P values reflect Pearson chi-square test, Mann-Whitney test, and Student t test.
Only complication categories with significant number of events are displayed.
Cost is presented for 2009–2011 patients and is missing for 10% of patients.
RASC=robot-assisted laparoscopic sacral colpopexy; IQR=interquartile range.
The overall incidence of in-hospital postoperative complications developing was 7% for non-RASC and 8% for RASC (P=0.360). Median LOS was 1 day longer for non-RASC. Both total charges to the primary payer and hospital costs were significantly higher for RASC, however.
There was an overall increase in the number and proportion of patients undergoing RASC throughout the study period, with a 58% increase in the odds of a RASC for each year of the study (P trend<0.001). This increase in RASC was most pronounced in the Midwest and South, with 73% and 122% increases in the odds of RASC per year, respectively (Fig. 1). On multivariable logistic regression, patients undergoing concurrent hysterectomy were at 1.28 times the odds of RASC (P=0.014) (Table 3). In addition, compared with patients with Medicaid, patients with private insurance or Medicare as their primary payer were at significantly increased odds of undergoing RASC.
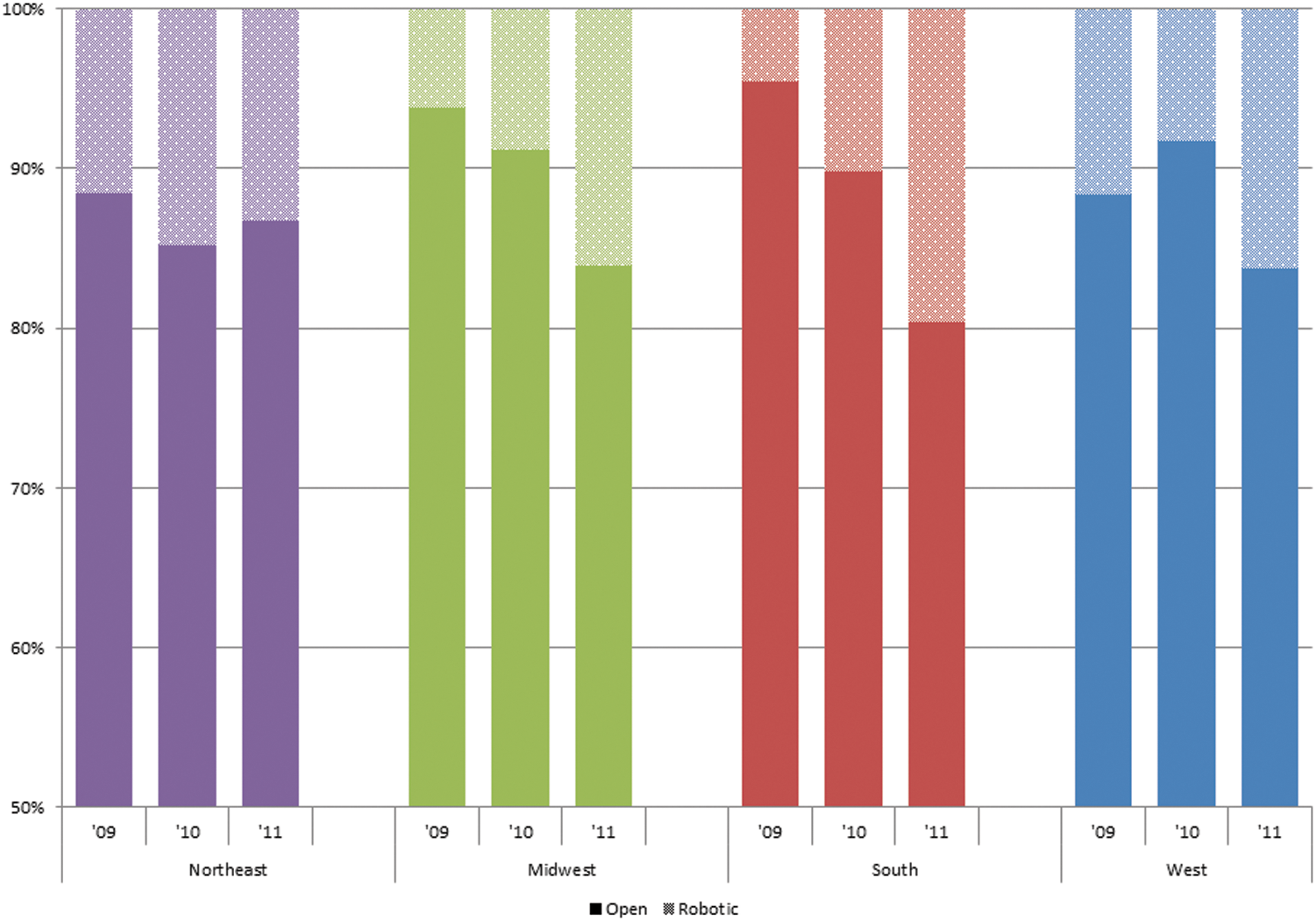
The Midwest and South had the greatest increases in the proportion of patients undergoing robot-assisted laparoscopic sacral colpopexy during the study period (annual change from univariate logistic regression: Northeast odds ratio (OR) 1.08, 95% confidence interval (CI) 0.58–2.02, P trend=0.803; Midwest OR 1.73, 95% CI 1.15–2.59, P=0.008; South OR 2.22, 95% CI 1.57–3.15, P<0.001; West OR 1.28, 95% CI 0.86–1.91, P=0.224).
The regression model is adjusted for all covariates presented within this table.
CI=confidence interval; CCI=Charlson Comorbidity Index.
On multiple linear regression, after adjusting for comorbidities, concurrent procedures, experiencing an in-hospital complication, region, and year, RASC was associated with a $4825 increase in hospital costs compared with other vaginal suspension procedures (P<0.001) (Table 4). The presence of an in-hospital complication contributed $4299 to the cost of hospitalization, independent of additional procedures and comorbidities. Concurrent sling and hysterectomy were each associated with approximately $1000 in increased costs. The West had the highest associated costs for vaginal suspension procedures. Hospital costs increased over time, with an overall increase of $1152 in 2011 compared with 2009 (Table 4).
The regression model is adjusted for all covariates presented within this table.
CI=confidence interval; CCI=Charlson Comorbidity Index.
As shown in Table 5, the median cost of RASC and non-RASC varied by payer type, with the highest reimbursement for RASC being paid by private insurance and the largest reimbursement for non-RASC paid by Medicare. RASC was consistently more costly than non-RASC, regardless of payer type.
The regression model is adjusted for all covariates presented within this table.
RASC=robot-assisted laparoscopic sacral colpopexy; IQR, interquartile range.
Discussion
We report no significant difference between US regions in the percentage of patients undergoing RASC vs non-RASC. Analysis of available data did indicate that between 2009 and 2011, the South experienced the greatest increase in the proportion of patients undergoing RASC. Delayed surgical robot acquisition in the South could have led to the late upswing observed in this region. Despite the reported regional delay, recent data support that the South is now similar to the rest of the country with regard to utilization of RASC. We were also able to identify a number of factors that significantly impact hospital costs associated with vaginal suspension. Use of the robotic approach as well as experiencing an in-hospital complication both were major contributors to increased costs, and there was significant variation in cost based on US region. Interestingly, although private insurance was associated with increased reimbursement, we report that regardless of primary payer, RASC was consistently more costly by up to $5500.
Interestingly, we identified significant regional differences in patients undergoing concurrent hysterectomy. We found that patients in the Northeast and West were the most likely to undergo concurrent hysterectomy in the setting of vaginal suspension, and this difference is particularly striking when only comparing among RASC patients. This is in contrast to studies reporting regional rates of primary hysterectomy, which are highest in the South and lowest in the Northeast. They also report average age to undergo hysterectomy is lowest in the South and highest in the Northeast. 12
There are many potential reasons for this distinction, including regional differences in training. Because fewer subjects in the Northeast undergo hysterectomy in general, it is possible that more have a uterus present when receiving a diagnosis of apical prolapse, accounting for the need for concurrent hysterectomy. It is also possible that regional culture may influence patient motivation to undergo hysterectomy.
In a study of patients required to seek a second opinion after a first surgeon recommended hysterectomy, Finkel and coworkers 13 surveyed patients who were subsequently recommended against surgery. They found that a higher percentage of women in the South and North Central regions of the United States chose to undergo hysterectomy despite the second opinion advising against it and suggest that this population was more likely to have the operation regardless of medical necessity. In regions, such as the South, in which hysterectomy is performed more commonly and at a younger age, it stands to reason that these women would not be candidates for concurrent hysterectomy. Further exploration of this is not possible with NIS. Much would be gained, however, from additional studies that explore motivations for undergoing hysterectomy.
Cost analyses of RASC compared with non-RASC vaginal suspension procedures report mixed results. Patel and colleagues 14 reported in a comparison of open, laparoscopic, and robotic sacral colpopexy that operating room and material costs were significantly more expensive for minimally invasive approaches vs open, but other direct costs related to anesthesia and hospital stay were not significantly different. Their study population was small, however, and lacked sufficient power to detect a significant difference in either operating room times or hospital stay, both of which have been commonly reported in the literature. 14 –16 Judd and associates 17 found that even after discounting the cost of robotic equipment purchase, RASC was still the most expensive approach. They attributed this increased cost to longer operating room times and increased use of disposables.
Anger and colleagues 6 examined costs and outcomes associated with RASC vs laparoscopic sacral colpopexy with standardized cost reporting measures. Physician charges and cost of any rehospitalizations were included (neither of which were available through NIS). Participating surgeons had completed a minimum of 10 required procedures using each approach, and they found that operative times from first incision to either robot undocking or last laparoscopic suspension suture were significantly shorter for the laparoscopic group. Despite this, there was no significant difference in total surgery time. They found that additional expenses associated with RASC were only significant when the cost of the robot was included in the analysis (6 week costs were robotic $20,898, laparoscopic $12,170, P<0.001). It is important to note that their cohort was limited to two institutions.
In contrast to the above-mentioned studies, Elliot and coworkers 16 found that RASC resulted in lower hospital costs than open sacral colpopexy (OSC), assuming sufficient hospital case volume over which to divide equipment costs and that hospital stay was sufficiently shortened. This analysis included acquisition and maintenance costs for the robot and was estimated using institutional data for operative time (found to be similar between RASC and OSC) and length of stay (1.0 days RASC vs 3.3 days OSC, P<0.001). Others agree that although RASC costs can be difficult to estimate, the procedure can be an economical choice provided that the above criteria are met. 4,15
Although all surgical procedures incur fees for operating room time, anesthesia, and hospital stay, robotic surgery also carries with it costs related to purchasing the system itself, the yearly maintenance, and disposable instruments. 16 Furthermore, some hospitals distribute these additional costs between all robotic surgeries, some between all surgical patients, and some over all hospitalized patients. For these reasons, performing cost comparison of robotic procedures to their nonrobotic counterparts has historically been quite difficult. To make worthwhile predictions given limited data, it may be of some value to examine trends in costs related to other robotic procedures.
Chang and colleagues 18 in their study of robotic prostatectomy reported a gradual decrease in costs of robotic surgery over time. Notably, they also saw a strong association of costs with operative time—as operative efficiency improves, costs tend to decrease. Their study, however, notes dramatic centralization of prostatectomies that is not yet seen in our studied population, whereby the proportion of cases performed by high-volume surgeons increased from 10% to 45% over a 7-year span. This meant that despite the overall increase in costs for prostatectomies (open and robotic), relative costs shifted over time from robotic to open approaches as comparative operative efficiency began to favor robotic technique. Given that inpatient hospitalization costs as a whole have inflated over time, 19 we would accordingly expect to see similar patterns in RASC costs as nationwide utilization increases.
There exists a disparity in access to RASC: Patients living in high-income areas are proportionately more likely to undergo RASC, and those with private insurance are nearly twice as likely as those with Medicaid to undergo RASC. Our results indicate that at a nationwide level, there is an overall increase in cost associated with RASC and that minimally invasive care is more likely to go to those who can afford it. Because differences in billing practices between hospitals appear to account for some interhospital variability, establishing cost equivalence for RASC will rely partly on implementation of a predictable, standardized, and comprehensive cost calculation strategy. Economizing these potentially costly procedures may ultimately involve further efforts to concentrate performance of these procedures at high volume “centers of excellence.” This may result in a better distribution of costs, making each procedure more affordable to the individual patient.
Because the NIS is an administrative database, there are limitations worth noting. First, we cannot account for differences in coding practices between regions or institutions that report to NIS. In addition, we are unable to identify operative or pathologic findings associated with procedures, limiting our ability to adjust for operative complexity. Furthermore, as discussed previously, fixed costs associated with acquisition and maintenance of the robot are distributed differently at each institution, and details of those policies are not available through NIS. Finally, limited data were available that would allow for a detailed analysis of complication rates.
Although NIS is not explicitly designed to capture and categorize complications, overall complication rates as indicated by ICD-9 code can be useful when performing cost comparison to assess for differences in complexity of hospitalization. Despite these limitations, this study is the first US population based study to examine national trends and hospital costs associated with RASC.
Conclusion
Rates of RASC utilization have increased nationwide, and this increase has been most prominent in the South. Despite the fact that utilization has equalized among United States regions, the data indicate that there still exists a disparity in access to RASC. This is potentially because implementation of RASC typically implies an increase in hospital costs. Although this procedure does have potential as a cost-effective minimally invasive approach, a comparison of nationwide vs institutional data suggests that this is only the case in hospitals that support enough volume, experience, and efficiency to counteract the additional expenses of upkeep. Given this disparity, it is incumbent on individual hospitals and healthcare providers to be conscientious in their choice of treatment. Although the differences in average cost between RASC and other approaches to vaginal suspension can be striking, the decision to undergo RASC is multifaceted and should primarily take into account patient health, severity of prolapse, and surgeon experience.
Author Disclosure Statement
No competing financial interests exist.