
Abstract
Purpose:
This study evaluated face, content, construct validity, and reliability of Thiel embalmed cadavers (TEC) as a training tool for transperitoneal laparoscopic nephrectomy (TLN).
Materials and Methods:
The study participants were prospectively recruited through an advanced laparoscopic renal resection teaching skill course. The participants were grouped into: nonexperts (performed fewer than 50 TLNs) and experts (performed more than 50 TLNs). All the participants performed TLN on TEC, which was video recorded. All participants rated their overall experience of performing TLN on TEC with emphasis on realism (face validity). The participants were asked to rate the appropriateness of TEC for training in TLN (content training). Two experienced laparoscopic surgeons, using validated modified Objective Structured Assessment of Technical Skills, assessed the individual videos. The parameters studied were: Respect for tissues, time and motion, and instrument handling for each step of laparoscopic nephrectomy (LN) (construct validity). Test-retest and interrater reliability was also evaluated.
Results:
Twenty-four participants (4 experts and 20 nonexperts) took part in this study. The mean overall rating for the experience of TLN on TEC was 4.5 (Face Validity). The mean score for the appropriateness of TEC as a training tool for TLN was 4.6 (content validity) when evaluated by the four experts. The mean scores for the nonexperts and experts using video recordings for various variables were: Respect for tissue—1.74 (standard deviation [SD]–0.62) vs 3.63 (SD–1.06), (P<0.01), time and motion—1.74 (SD–0.58) vs 4 (SD–0.76), (P<0.01), and instrument handling—1.84 (SD–0.61) vs 4.25 (SD–0.71), (P<0.01) (construct validity). The study also suggested test-retest and interrater reliability.
Conclusions:
This study suggests face, content, and constructs validity and reliability of the TEC as a training tool for TLN.
Introduction
T
A recent European survey reported only more than a third of the residents to be satisfied with their laparoscopic exposure and experience. 4 This has been reflected in the “European Basic Laparoscopic Urological Skills 2011–2012 examination” results, reporting a pass rate of 4.2% when final year urology residents were assessed for time and quality of laparoscopic skills. 5 Achieving competence is, however, crucial for urology trainees before receiving certification for independent clinical practice.
Currently, trainees in the United Kingdom (UK) have an aspirational expectation by the Joint Committee of Surgical Training (JCST) to perform a nephrectomy with minimal supervision to achieve Certificate of Completion of Training. 6 Interestingly, a recent pan-European survey suggested that two-thirds of trainee urologists in final stages of their training did not complete laparoscopic nephrectomy (LN) as a first operator suggesting that the JCST's expectation is potentially unrealistic. 4 There is, therefore, an urgent need to review training methods and develop tools to facilitate minimally invasive training.
There is a commonly held perception that the traditional apprenticeship style of surgical training is obsolete, and there is a need for the incorporation of Simulation based Training (SBT) into the urology training curricula. A recent survey of the opinions of urology Training Programme Directors (TPD, n=16) in the UK reported that laparoscopic simulators improve laparoscopic training and should be integrated into urologic training curricula. 7 SBT has been shown to improve laparoscopic skills and potentially reduce learning curves. 8 –10 A recent randomized controlled trial concluded that a portable Integrated Laparoscopic Simulator improved core laparoscopic skills in medical students with no previous experience of surgery. 11 Furthermore, the feasibility of a centralized simulation program is currently being explored. 12
Operating on live patients by relatively inexperienced trainees is challenging because of concerns of compromise in patient care quality and safety. To maintain progressive surgical education, it is paramount that tools for surgical skills acquisition are continually developed. Inanimate objects or devices are often used for initiation and progressive honing of basic and advanced surgical skills before operating on live patients. Inanimate objects, however, lack fidelity.
Traditionally, human cadaveric models have been an invaluable resource for anatomic and surgical training, with an ability to achieve a high level of fidelity without subjecting patients to inherent risks of surgery. Human models should and can form an intermediate training tool before a novice's progression to operating on live patients, particularly in the setting of a teaching course. 2
Laparoscopic training using human cadaveric models was previously limited because of their inability in creating satisfactory pneumoperitoneum and lack of normal tissue texture. Recent advancements in embalming techniques such as the Thiel embalming method have addressed these issues, reproducing a real-life operating experience for LN.
Our group previously introduced the utility of Thiel embalmed cadavers (TEC) for training in LN. 2 TEC along with other simulators have a significant role to fill voids in contemporary surgical skills training. A critical evaluation of this novel cadaveric preparation method as a training tool, however, has not been reported. In the present study, we have systematically assessed the reliability and validity of TEC for laparoscopic renal resection.
Ahmed and associates 13 reported a three-point approach to evaluating novel training tools including initial design (face and content validity), validation (construct validity, reliability and concurrent validity) and implementation (feasibility, acceptability, educational impact, cost-effectiveness, predictive validity. This study aims to perform a preliminary validation process of TEC as a training model for LN training with emphasis on face, content and construct validity, and reliability.
Materials and Methods
Design
This is a prospective, observational single center study. Human cadavers embalmed by the Thiel method were used in the study, which were processed in the Centre for Anatomy and Human Identification at the University of Dundee, United Kingdom.
Thiel embalming technique
Thiel and colleagues 14 first described this method of embalming cadavers. The embalming fluids used are water based containing 4-chloro-3-methylenphenol for mold prevention; boric acid and various salts for disinfection and fixation; ethylene glycol for tissue plasticity conservation; 0.8% formalin in the submersion fluid; and alcohol with morpholine in the intravascular fluid for tissue consistency and color preservation. 2,14 Thiel's method uses intravascular perfusion embalming followed by at least 2 to 3 months of submersion.
Participants
Participants were recruited from a 2-day training course run for consecutive years since 2011. All the participants were involved (assistants, performing parts of the procedure, and primary surgeon) with a minimum of 10 cases of transperitoneal laparoscopic nephrectomy (TLN). They were grouped into: (1) Nonexperts—performed fewer than 50 cases of LN as primary surgeon; and (2) experts—experience of performing more than 50 cases independently as primary surgeon. The figure of 50 was chosen to differentiate between nonexperts and experts because this was defined as the number required to be a mentor by the British Association of Urological Surgeons (BAUS). 15
The layout of the course was divided into two sessions: (1) Didactic lecture and short video session on the principles of TLN in TEC.
16
(2) Skills session: Each nonexpert performing a TLN under the supervision of two experts. The experts also performed TLN on the cadavers. The procedures were video-recorded. The Delphi process was used to achieve agreement between the experts in scoring tasks and skills needed for TLN (Fig. 1).

Delphi process consensus for steps of laparoscopic nephrectomy.
On conclusion of the Delphi process, the following 10 steps were finalized: a. Setup and positioning of the body for TLN. b. Location of landmarks and ease of trocar entry. c. Pneumoperitoneum creation. d. Orientation and identification of anatomic landmarks. e. Mobilize and elevate the ureter to allow dissection and elevation of the lower pole. f. Continue dissection to allow identification of the hilum (Fig. 2). g. Identification and skeletization of the renal vein and artery (Fig. 2). h. Clip and divided the artery and vein. i. Mobilize the upper pole and lateral aspect of the kidney. j. Entrap and deliver the specimen.
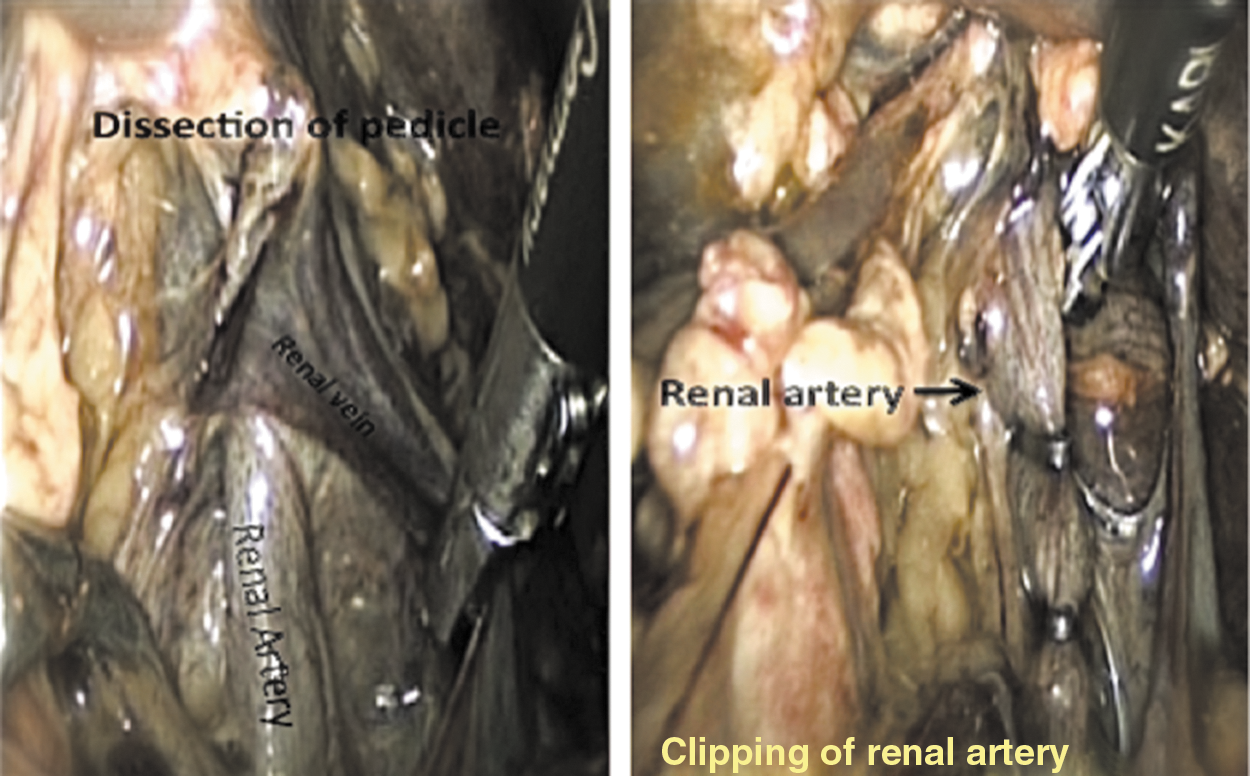
Dissection of the pedicle and clipping of the renal artery.
This breakdown facilitated learning and comprehension of the entire procedure by the participants and assessment of procedural skills by the reviewers.
Outcome parameters
Face/content validity
All the participants were asked to rate their overall experience of performing a TLN on TEC and rate individual steps of TLN using the five-point Likert score with an emphasis on realism (face validity). In addition, the participants were asked to rate their experience for the following domains: (a) Quality of the tissue and organ color; (b) tissue consistency; (c) tissue tactility during dissection; (d) fluid content of the tissue; and (e) odor of the cadavers with an emphasis on realism (face validity). The experts were asked to rate the appropriateness of TEC for training in TLN (content training) using the five-point Likert score.
Construct validity
Video recordings of LN performed by the participants were edited to include the stepwise procedure of TLN. Videos were randomized and assessed blindly by two experienced laparoscopic surgeons (BS, CS) not originally involved with the laparoscopic surgical courses using three domains of the validated and reliable Objective Structured Assessment of Technical Skills tool/Global Rating Scale, as shown in Table 1. 17 The following domains were assessed and each assigned a score ranging from 1 to 5, giving an overall total of 15 maximum points:
a. Respect for tissues (excessive force/traction).
b. Instrument handling (instruments collisions, instruments missing the target, correct application of energy).
c. Time and motion (procedural time, unintended movements of instruments).
The authors used only three domains of this form, and the remaining four were excluded. The objective of this exercise was to evaluate construct validity of TEC. The domains including communications skills use of assistants, knowledge of procedure, and flow of procedure (planning and forward planning) could not be evaluated on blinded videos and were therefore excluded.
Reliability
The mean scores of each step of LN on TEC filled by participants using the Likert score were calculated for years 2011, 2012, and 2013. Test-retest reliability was calculated by comparing the mean scores for each step of TLN for the years 2011, 2012, and 2013. Interrater reliability was also calculated.
Statistical analysis
Two independent variables were compared using the Mann-Whitney test. Multiple independent variables were compared using the Kruskal-Wallis analysis of variance. A two-tailed significance level of P<0.05 was considered to indicate significance. Box/Whisker plots were graphically used to compare the performances between the two groups with box representing the interquartile range, bar representing mean, and whisker representing range. Interrater reliability was calculated using the Spearman and Pearson correlation coefficient test. Statistical analysis was performed using the software StatPlus (version 2).
Results
Demographics
Twenty-four participants were categorized as nonexperts (20) and experts (4) based on the levels of previously defined clinical laparoscopic experience.
Face, content validity
The mean overall rating of overall experience of performing TLN on TEC with emphasis on realism was 4.5 (face validity). The mean score for the quality of tissue and organ color, tissue consistency, tissue tactility, and tissue fluid content was higher than 4 (face validity). The mean rating of the various steps of LN is displayed in Table 2. The mean scores of all the participants, experts and nonexperts, for each step of the LN was higher than 4 (face validity). Experts rated the TEC at least 4 on for “Appropriateness of TEC as a training tool for TLN” with a mean score of 4.6 (content validity).
n=19.
n=15.
SD=standard deviation.
Construct validity
The mean scores for the nonexperts and the experts, respectively, were:
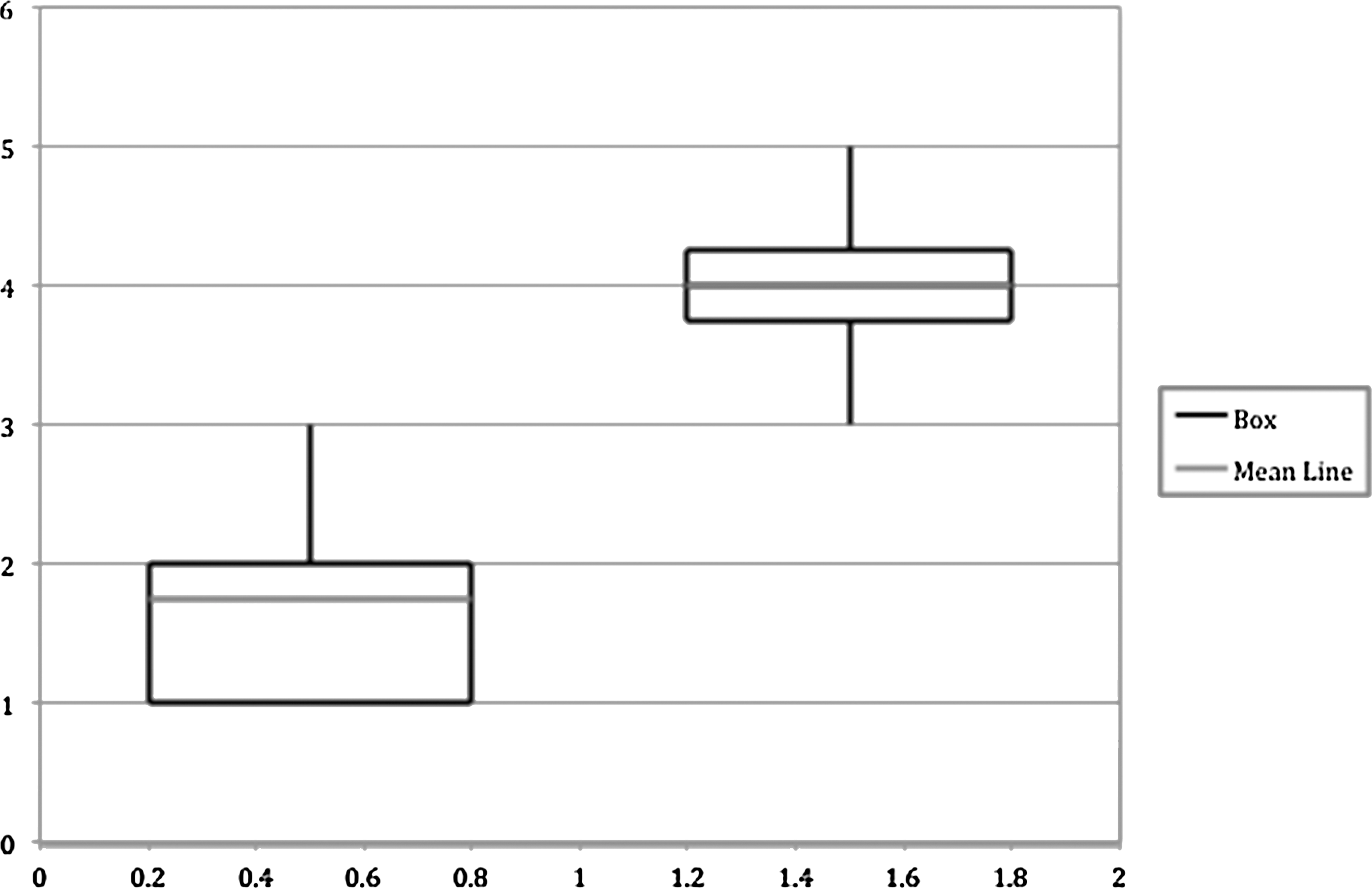
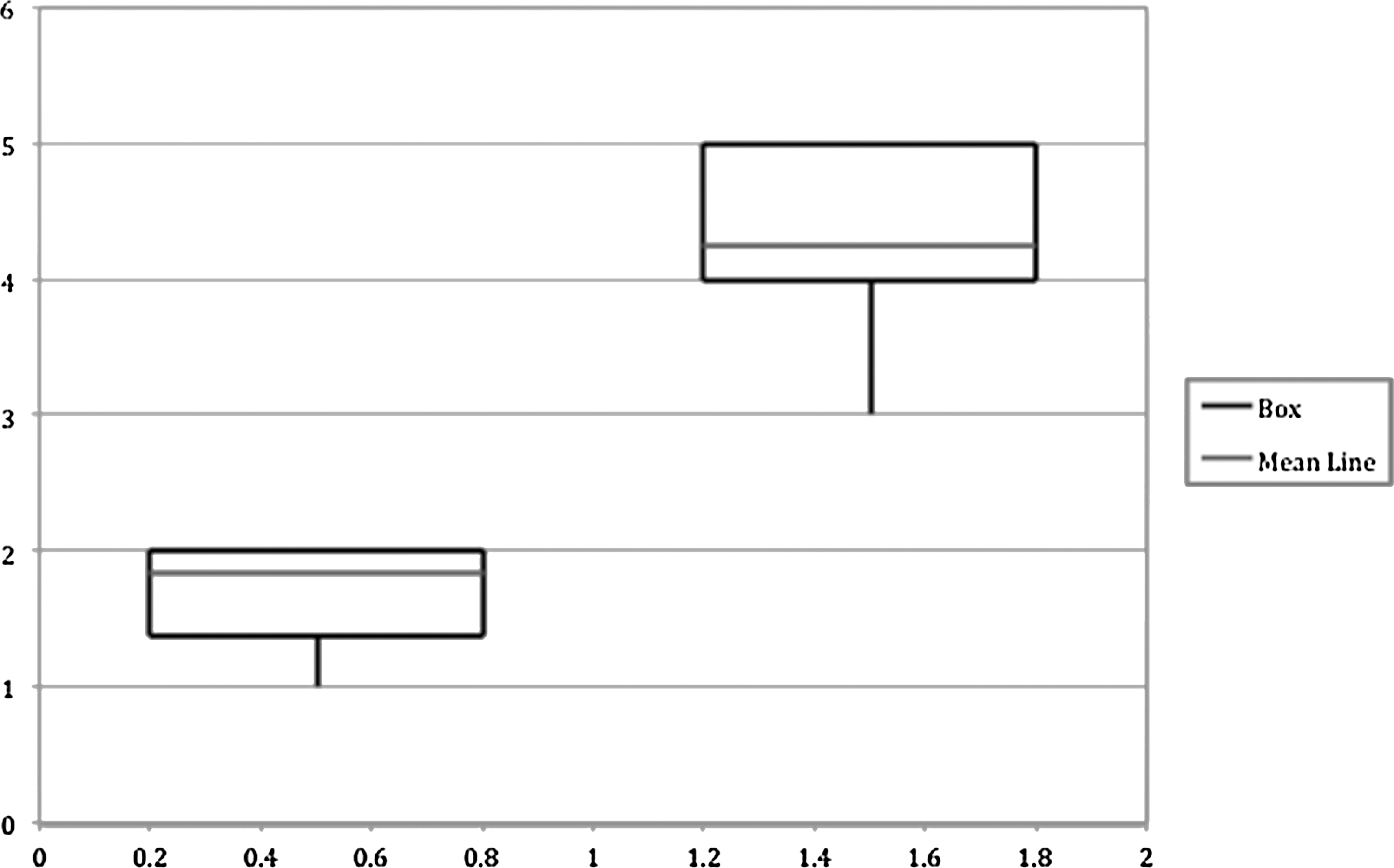
Overall score—5.16 (SD [standard deviation]–1.53) vs 11.88 (SD–2.3) (P<0.01) (Fig. 3); respect for tissue—1.74 (SD–0.62) vs 3.63 (SD–1.06), (P<0.01) (Fig. 4); time and motion—1.74 (SD–0.58) vs 4 (SD–0.76), (P<0.01) (Fig. 5); and instrument handling—1.84 (SD–0.61) vs 4.25 (SD–0.71) (P<0.01) (Fig. 6).

Overall score boxes (interquartile range) and whisker (range). Bar=median. Mann Whitney test, P<0.001.

Respect for tissue boxes (interquartile range) and whisker (range). Bar=median. Mann Whitney test, P<0.001.
Time and motion boxes (interquartile range) and whisker (range). Bar=median. Mann Whitney test, P<0.001.
Instrument and handling boxes (interquartile range) and whisker (range). Bar=median. Mann Whitney test, P<0.001.
Reliability
Test retest reliability
The mean score for the various steps of TLN for the respective years of 2011, 2012, and 2013 was consistently above 4 (Table 3). There was a statistically significant improvement in mean scores for the steps: (a) Mobilization and retraction of the ureters to allow dissection and elevation of the lower pole (P-0.01); (b) identification and skeletization of the renal vein and artery (P-0.005).
n=5
n=7
SD=standard deviation.
Interrater reliability
The R-value for the Spearman test was 0.8, and the Pearson correlation coefficient was 0.95 for the two ranks. The association between ranks by two blinded assessors (BS, CS) was significant (P<0.001) indicating a strong correlation (Fig. 7).

Interrater reliability.
Discussion
The present study suggests face, content, and constructs validity for TEC as a training model for TLN. In addition, this study suggests test-retest and interrater reliability. The mean scores for all the parameters measured were consistently high (minimum mean score=4) across various levels of laparoscopic experience (experts vs nonexperts). Three parameters in the study—economy of motion, handling of instruments, respect for tissues—assessed by experts using a validated instrument were able to differentiate between experts and nonexperts conclusively, thus suggesting construct validity, with experts scoring significantly higher. The mean scores for all the respective years for each step of the LN were more than 4/5 suggesting that TEC is reliable and performing consistently (test-retest reliability).
Currently available validated simulators for LN are high fidelity virtual reality simulators, which include Procedicus MIST Nephrectomy and LAP mentor (Simbionix). 18 Virtual simulators lack fidelity in comparison with cadaveric models. Brewin and colleagues 19 demonstrated high face, content, and construct validity for Procedicus MIST Nephrectomy. The performance of Procedicus MIST Nephrectomy, however, was inferior to TEC in the present study with the Likert score for similar steps between 3 and 4.
A recent prospective study comparing face validity of LAP mentor Symbionix with fresh frozen cadavers concluded that the cadaveric models were significantly better models for laparoscopic training. 20 Although not formally evaluated in this study, expert surgeons in this course with previous experience with fresh frozen cadavers commented TEC to have superior fidelity when compared with fresh frozen cadavers.
The Swiss Association of Laparoscopic and Thoracoscopic Surgery has conducted advanced laparoscopic courses using human cadavers embalmed by the Thiel method for various surgical subspecialties. 21 The responses by the participants for tissue consistency, color, and operative tactility were all rated greater than 4. These findings are in corroboration with our observation.
There are numerous simulation training tools available in urology departments and continue to be developed in the form of virtual simulators for training in laparoscopic upper tract surgery. Despite their continued refinement and evolution, however, these are nonlifelike models lacking fidelity. Moreover, they will always be anatomically inferior to the human body. Human cadavers remain a very important resource for basic anatomy teaching. They can also have a significant role in endoscopic and laparoscopic training if embalming techniques can negate compromised tissue quality from rigor mortis.
Conventional formalin embalming, the most widely used technique for cadaver preservation, significantly compromises human tissue quality. To address this, soft-fix techniques have been described 22 comparing embalming fluids according to Graz, Dodge, and Genelyn preparations with favorable results; fresh frozen 23 and lightly embalmed 24 techniques are researched and used as alternatives to overcome the tissue changes. Despite their ability to provide a resemblance to a real-life human body, the use of conventional embalming techniques has been limited because of poor consistency, texture, odor, durability, inability to create a pneumoperitoneum, and demonstrate endoscopic anatomy. The Thiel embalming technique has the potential to counter these limitations.
In this study, the TEC achieved a score of 4.31 for creating pneumoperitoneum. The method avoids the requirement for further refrigeration or vacuum packing; instead, storage can be in the form of plastic bags or continuous submersion. 25 Furthermore, the Thiel method possesses exceptional disinfecting efficacy while releasing minimal harmful chemicals into the environment. 26
TEC is an important resource that can be integrated into current training curriculums along with the existing simulation tools in laparoscopic upper tract surgery. The authors envisage the role of TEC mainly in course settings. BAUS continues to recommend attendance at dry and wet laboratory courses to initiate laparoscopic training. 15 With the current Animal Legislation Act banning the use of live animals for training, 27 the current recommendation is often impractical for the UK based trainees. 2
The European Association of Endoscopic Surgery guidelines mandate the validation of new simulators before incorporating them into training programs or using them for assessment purposes. 28,29 Having demonstrated the required validity, it would seem sensible to use TEC as an advanced training tool for senior urology trainees/residents just before starting as a first surgeon while performing a TLN and could be incorporated as an obligatory course among trainees aspiring to become specialist laparoscopic upper tract surgeons.
Despite the obvious advantages, cadaveric training has some limitation such as cadaver unavailability and cost constraints in the maintenance of the cadavers. The basic infrastructure (cages, trays, and lifter) for maintenance is around 16,000 British pound sterling (about $25,000) for four bodies. Once institutions have available infrastructure for cadaver maintenance, the cost of chemicals for Thiel embalming is around 2500 British pound sterling (about $3900) for eight bodies. The Thiel embalming method preserves and maintains tissue quality for long periods; hence, it can be used on numerous occasions for training in different procedures. This property of TEC has advantages for skills centers in somewhat negating issues of cadaver unavailability and cost constraints.
The author's institution has now conducted the TEC course for LN annually for 4 years with an individual fee of 850-900 ($1300–$1400) British sterling. Furthermore, the same cadavers are used for student teaching, other postgraduate urology, and other subspecialties courses. This reusability and multidisciplinary adoptability for training and teaching make these models economically very viable to our institution.
The lack of vascular perfusion in TEC has limited its role as a training tool for vascular injuries in upper tract surgery. 21 Clearly models such as the “pulsating organ perfusion” are a useful tool for vascular injury training. To address this issue, the University of Dundee has developed pilot TEC models with perfusion satisfactorily demonstrated, which we will put through a validation process similar to the current study in the future.
Future research should involve work on establishing criterion validity both concurrent and predictive. How the training with TEC for TLN translates into reducing learning curves and facilitation of competence achievement is a subject of future research (predictive validity). In addition, comparison of TEC with high-fidelity virtual simulators, fresh frozen cadavers, and pulsating organ perfusion simulators in a randomized controlled setting will evaluate these simulators more accurately (concurrent). The role of TEC in training for other advanced urologic techniques (laparoscopic/robot-assisted prostatectomy and cystectomy) needs to be explored as well.
Conclusions
Given a higher rate of satisfaction and realism of the model, TEC appeared to be useful for laparoscopic training. TEC is an excellent additional resource available to upper tract laparoscopic aspirants. TEC appears to be a promising intermediary training tool in a course setting before trainee/resident progress to becoming a primary surgeon in TLN. This is clearly a model in evolution with further refinement needed to address important training issues such as vascular injury. The preliminary validation of TEC for TLN has shown satisfactory and promising outcomes.
Footnotes
Disclosure Statement
No competing financial interests exist.