
Abstract
The purpose is to present the first report and describe our novel technique for intracorporeal continent cutaneous diversion after robotic cystectomy. After completion of robot-assisted cystectomy using a standard six-port transperitoneal technique, three additional ports are placed, and the robot is redocked laterally over the patient's right side in the modified lateral position. Our technique replicates step-by-step the principles of the open approach. Ileocolonic anastomosis, ureteroenteral anastomoses, and construction of a hand-sewn right colonic pouch are all performed intracorporeally. Tapering of efferent ileal limb and reinforcement of the ileocecal valve are performed via the extraction site, while the stoma is matured through a prospective port site. Successful robotic intracorporeal creation of a modified Indiana pouch was achieved. Operative time for diversion was 3 hours, with negligible blood loss, and without any intraoperative complications. No major (Clavien III–V) 90-day complications were observed. At a follow-up of 1 year, the patient continues to catheterize without difficulty. We demonstrate the first description of robotic intracorporeal continent cutaneous urinary diversion after robot-assisted cystectomy. We present a systematic minimally invasive approach, replicating the principles of open surgery, which is technically feasible and safe with a good functional result.
Introduction
R
Technique
Patient positioning and port placement
At the completion of robot-assisted cystectomy, using a standard six-port transperitoneal configuration, 9 the patient is taken out of the steep Trendelenburg and dorsal lithotomy positions. The port setup used for cystectomy is modified to allow access to the right side of the abdomen to facilitate large bowel mobilization/segmentation and pouch creation. Of note, only three additional port sites (one at the site of the future stoma) are added from the cystectomy configuration (Fig. 1). Using the tilt of the operating table, the patient is placed in a modified lateral position, and the robot is docked over the patient's right side in preparation for the bowel work. For continent cutaneous urinary diversion using the right colon, the patient receives a mechanical bowel preparation with polyethylene glycol and is placed on a clear liquid diet 24 hours before surgery.
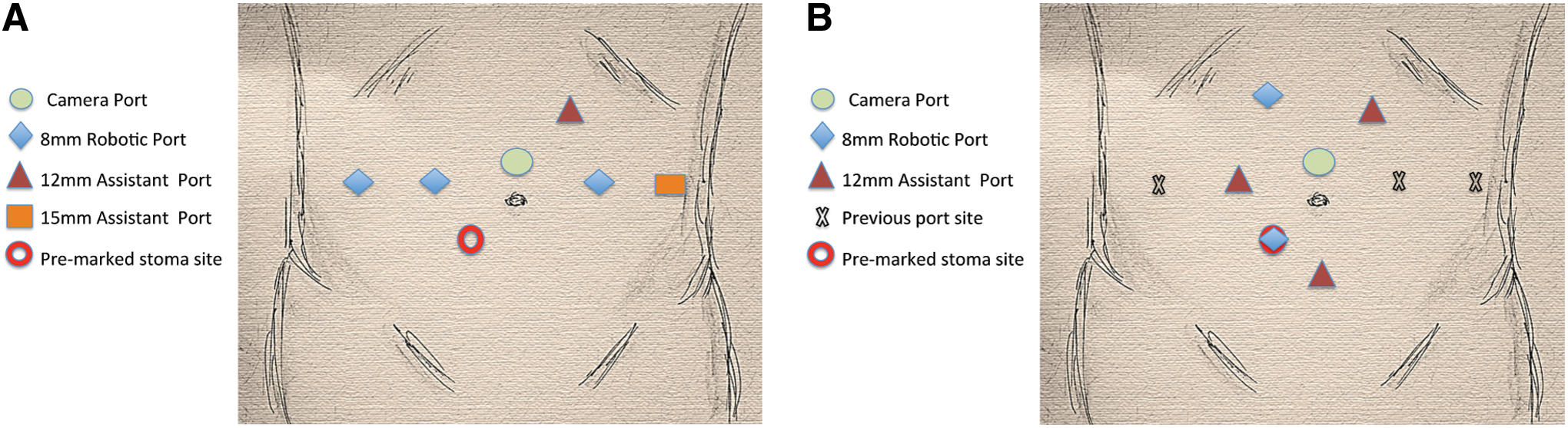
Transition from radical cystectomy port configuration (
Mobilization and segmentation of bowel segments
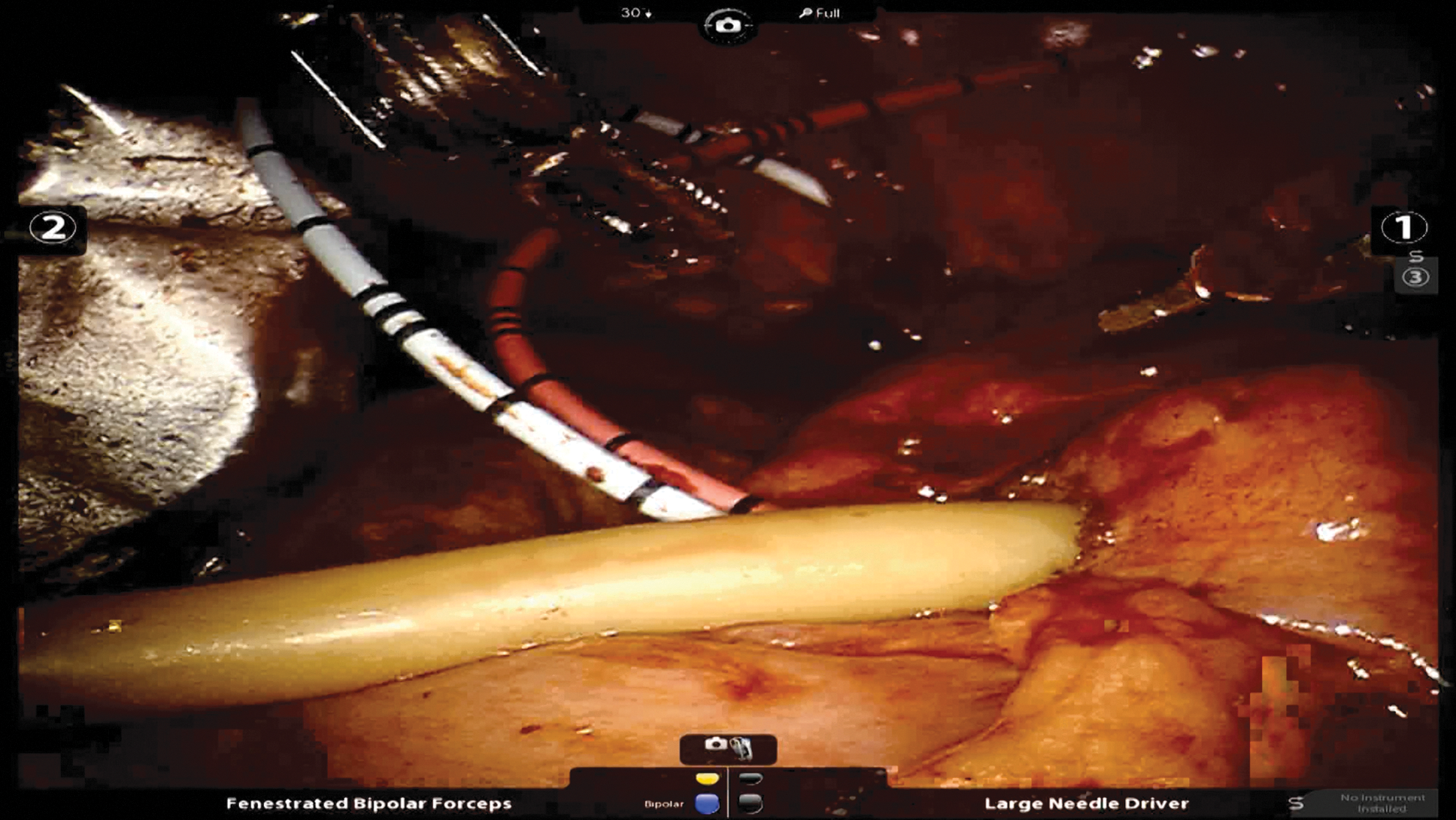
The ileocecal junction is first identified. The cecum and ascending colon are then mobilized. The colon is fully mobilized beyond the hepatic flexure to the midtransverse colon. A 30-cm segment of ascending colon is measured using a pr-marked latex drain (Penrose drain, Cardinal Health, Dublin, OH). Bowel manipulation is carefully performed using atraumatic double-fenestrated bowel graspers (Fig. 2). A 60-mm laparoscopic tissue load (3.5-mm thickness) stapler (Echelon Flex 60, Ethicon Inc., Cincinnati, OH) is introduced through the midline 12-mm assistant port to divide the large bowel. In a similar fashion, approximately 10 cm of distal ileum is measured for the efferent catheterizable channel and stoma. Using the left upper quadrant assistant port, the small bowel is transected again using a 60-mm bowel load stapler (3.5-mm thickness)
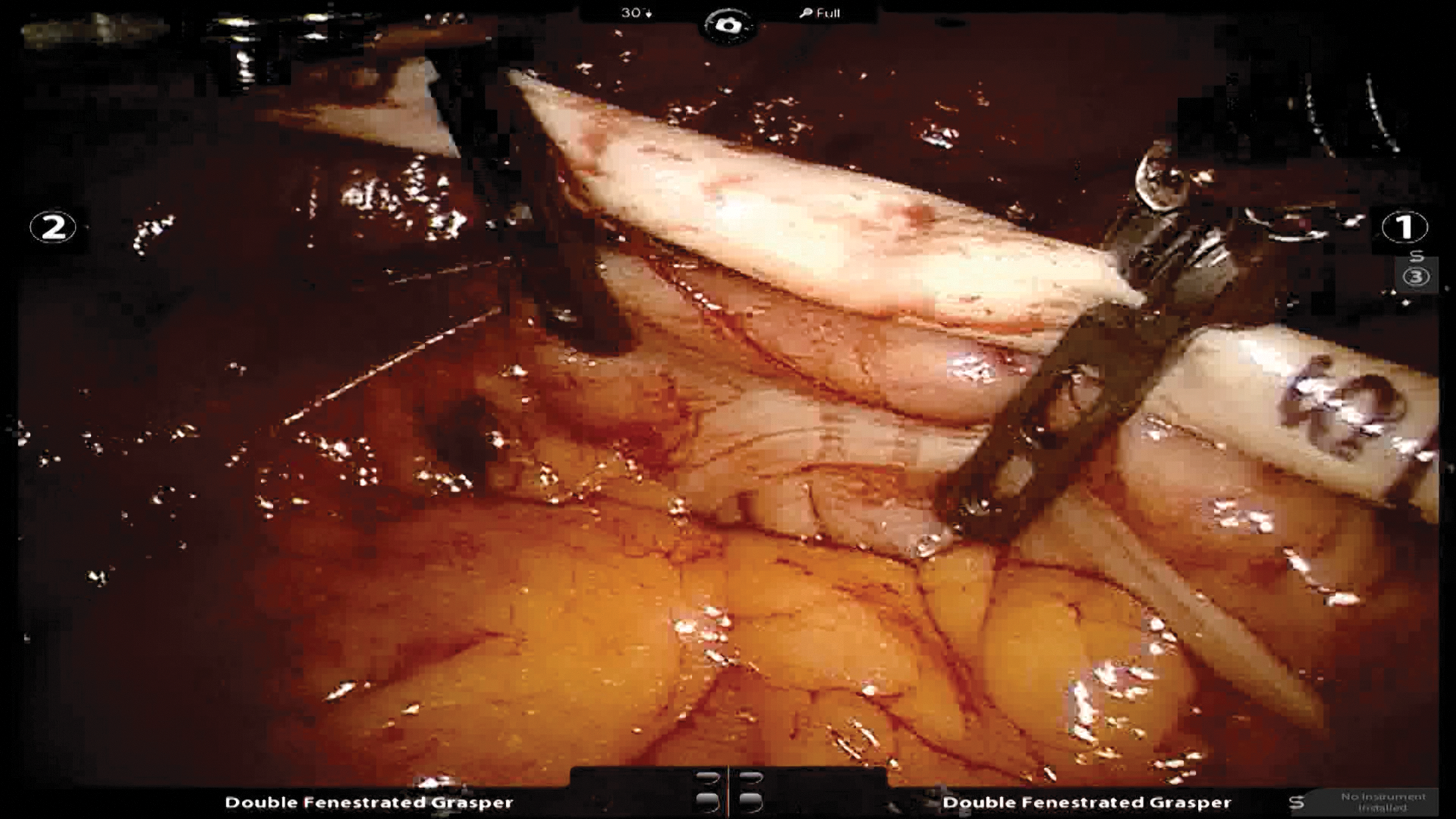
Double fenestrated graspers and a marked Penrose drain are used to measure bowel segments.
Restoration of bowel continuity
To restore continuity, a side-to-side ileal-colonic anastomosis is performed. A 60-mm laparoscopic stapler is introduced via the 12-mm right lateral assistant port and the antimesenteric surfaces of ileum and colon are joined in a side-to-side fashion (Fig. 3). The remaining open end of bowel is closed with another tissue stapler load deployed in a transverse direction via the 12-mm midline assistant port. The side-to-side anastomosis is reinforced using 3-0 polyglactin suture (Vicryl; Ethicon Inc.; Cincinnati, OH).
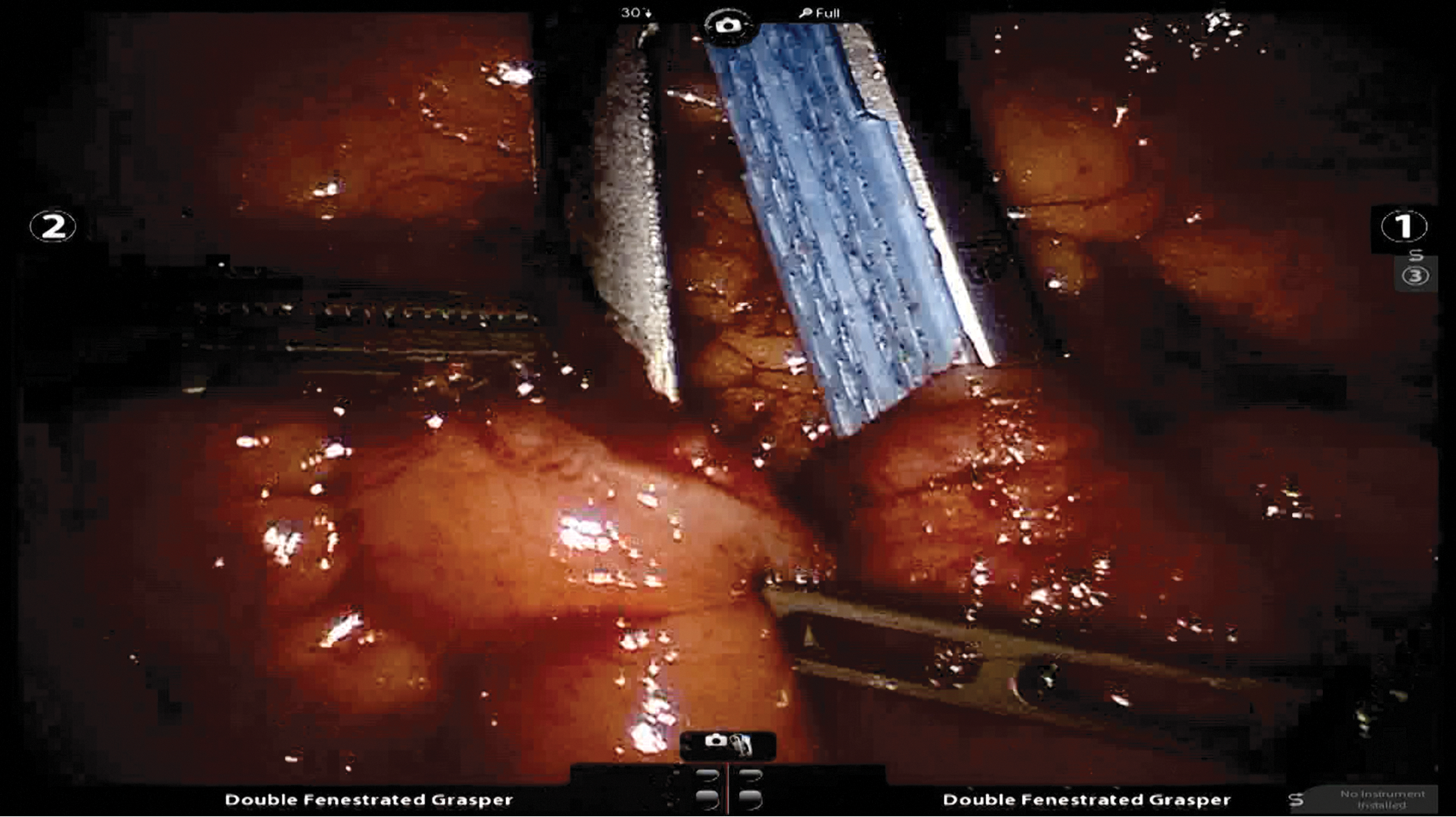
A 60-mm laparoscopic stapler is used to restore bowel continuity via the 12-mm right lateral assistant port.
Detubularization
Pouch construction begins with detubularization of the isolated colonic segment. The staple line is first removed off the transected end of the colon, and the entire antimesenteric length of colon is detubularized along the edge of the taenia using monopolar scissors (Fig. 4). When opening the large bowel, minilaparotomy pads are used to control the contents and then placed in an Endo Catch™ (Covidien) bag.
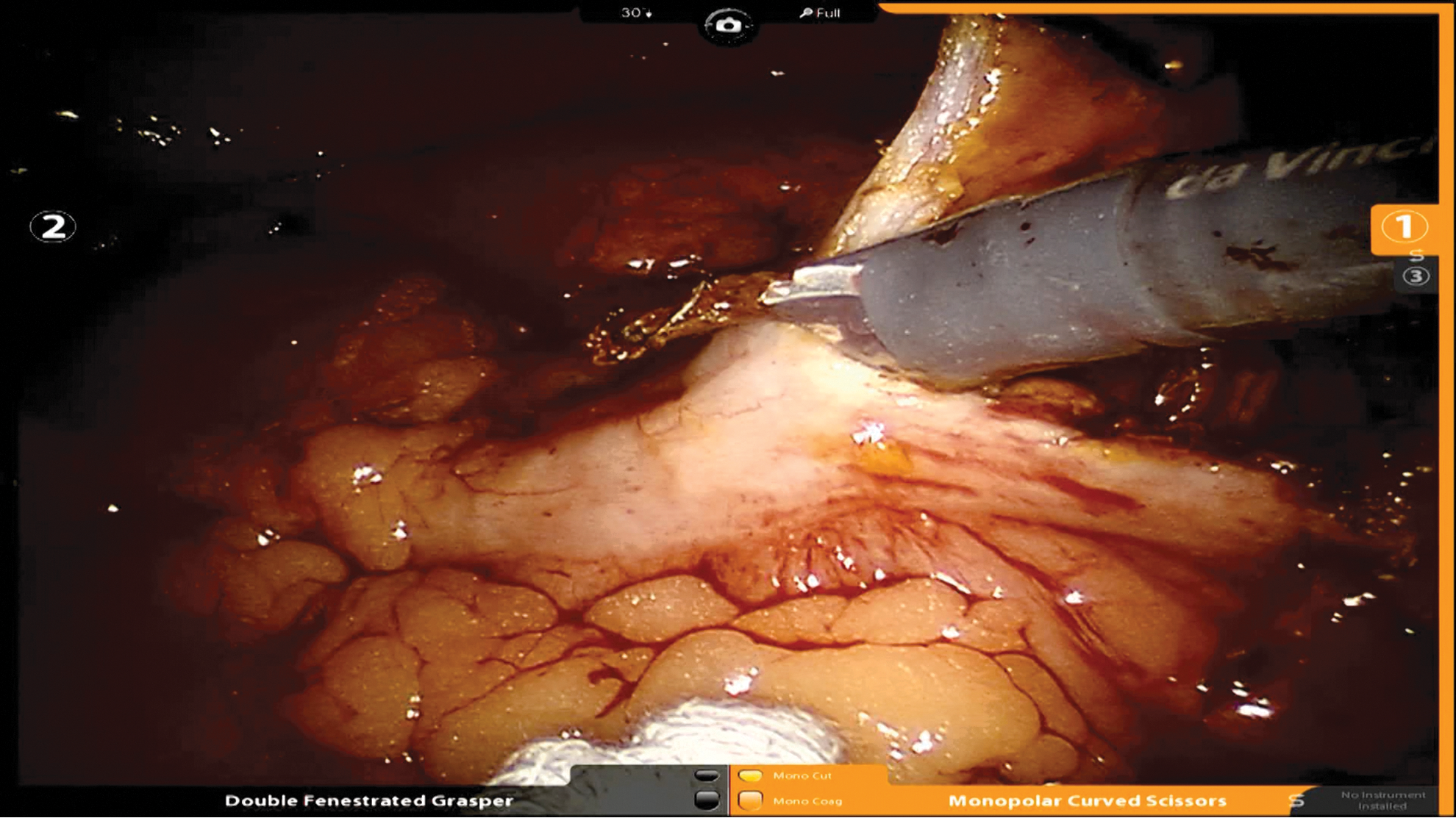
The entire length of isolated colon is detubularized along the antimesenteric taenia.
Ureterocolonic anastomosis
At the beginning of the cystoprostatectomy, the ureters are previously identified, clipped with ligation clips (Weck Hem-o-lok; Teleflex; Limerick, PA), and tagged with suture. The left ureter is transposed under the sigmoid mesentery to the right side. A 1-cm colonic hiatus is created on the posterior plate of the detubularized colon for each ureter. Sites are chosen on the posterior portion of the pouch to ensure a tension-free anastomosis without angulation of the ureters after folding. The ureters are passed from outside the colonic wall through the previously created openings. With adequate spatulation, the ureterocolonic anastomosis is performed in a Bricker fashion using two running 4-0 polyglactin sutures (PS-2 needle). Once the anastomoses are completed, a 2-mm port (Autosuture MiniPort 2 mm; Covidien, New Haven, CT) is used for percutaneous stent placement. Two 7.0F single J stents (Bander Ureteral Diversion Stent Set, Cook Medical, Spencer, IN) are positioned in each collecting system and secured in place with absorbable suture.
Creation of pouch
The open segment of colon is then folded over and approximated at the midpoint with an interrupted 2-0 polyglactin suture. An appendectomy is performed creating a cecostomy through which the single J stents are externalized from the pouch. Closure of the pouch is performed using barbed absorbable sutures (V-loc 2-0; Covidien Inc.; New Haven, CT) in a running fashion. With completion of the pouch, a suprapubic catheter (Malecot catheter, Cook Medical) is passed intracorporeally and inserted into the pouch through the cecostomy alongside the stents (Fig. 5). The stents and cecostomy tube are then secured with a purse-string suture. The pouch is irrigated through the Malecot catheter to confirm a watertight closure.
Malecot drain and stents are externalized through the appendiceal cecostomy.
Tapering of the efferent limb and stoma maturation
The robot is now undocked and the cystoprostatectomy specimen extracted via extension of the camera port site. Using this extraction site, the ileum is tapered over a 14F catheter using a tissue load stapler. The ileocecal valve is reinforced over the catheter using several interrupted 2-0 silk sutures. The efferent limb is then delivered through the previously marked stoma site. It is matured to the skin in standard fashion. The stents and Malecot drain are externalized via the right side assistant port. A closed suction drain is placed through the right lateral robotic port site. Figure 6 depicts the final postoperative appearance.

Final appearance at completion of the case. Indwelling 14F catheter remains in the stoma. Malecot drain and stents are externalized through the 12-mm assistant port site. Jackson-Pratt drain is placed through the previous lateral robotic port site. Color images available online at
Equipment
Role in Urologic Practice
The operative time for diversion construction was 180 minutes with negligible blood loss. There were no intraoperative complications. No major (Clavien grade ≥III) 90-day complications were observed. Our patient did need readmission at day 15 and day 26 postoperatively for education with catheterization and atrial fibrillation, respectively. At 1-year follow-up, the patient has no leakage and continues to catheterize without difficulty. He is satisfied with his functional result.
We observed no urinary fistula, bowel leak, or ureteral stricture in this intracorporeal continent cutaneous diversion. One area of concern regarding minimally invasive urinary diversion has been the rate of ureteral stenosis. We perform a Bricker anastomosis for all of our intracorporeal urinary diversions, including continent cutaneous pouch, ileal conduit, and neobladder. Our overall incidence of ureteral strictures in intracorporeal diversions necessitating surgical intervention is 2.4% (2/83), which is consistent with large open series. 11
There has been no stenosis of the catheterizable stoma. The appendix has been described as a channel for continent cutaneous diversion. In our experience and in the adult literature, however, the appendix is less reliable as a catheterizable conduit. The stenosis and wound dehiscence rate can be up to 100%. 12 In addition, the length and patency of the appendix in the adult is less predictable. Therefore, we prefer the terminal ileum along with the ileocecal valve as a more favorable efferent channel as well as continence mechanism, respectively.
We present the first description of a step-by-step technique for robotic intracorporeal continent cutaneous urinary diversion after robot-assisted cystectomy. This approach affords the patient a minimally invasive alternative for continent cutaneous diversion in conjunction with robot-assisted cystectomy. Complementing the armamentarium of previously described intracorporeal ileal conduit and neobladder with the addition of this technique, the choice of urinary diversion should not be limited by a minimally invasive approach. Continent cutaneous urinary diversion may be favorable when the urethra cannot be used because of previous radiation or oncologic involvement. In addition, patient preference may drive the need for a continent cutaneous diversion.
By performing a completely intracorporeal robot-assisted cystectomy and urinary diversion, we aim to confer the potential benefits of decreased bowel manipulation, quicker return of bowel function, reduced pain, and decreased incisional morbidity. Further investigation of these proposed benefits are currently under way.
In conclusion, we describe our technique for intracorporeal continent catheterizable urinary diversion after robot-assisted cystectomy. We demonstrate that this procedure is technically feasible and safe with good functional outcome (a supplemental video demonstrating this technique is available at
Footnotes
Author Disclosure Statement
Alvin C. Goh is a proctor for Intuitive Surgical, Inc. No competing financial interests exist for the remaining authors.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.