
Abstract
Background and Purpose:
Three-dimensional (3D) laparoscopy has been developed in an attempt to address one of the main limitations of laparoscopic surgery, which is two-dimensional (2D) vision. Still, data on the learning curve during adaptation of such technology in clinical practice are scarce. In this study, perioperative data from the initial operations performed by an experienced laparoscopic surgeon in a 3D laparoscopic setup are presented, aiming to document any difficulties faced during the integration of 3D vision to laparoscopy.
Patients and Methods:
In total, 15 consecutive, unselected cases were operated using 3D laparoscopy within a 30-day period. The cases included five laparoscopic extraperitoneal radical prostatectomies, three nephrectomies, three partial nephrectomies, one nephrouretectomy, one adrenalectomy, one ureterolithotomy, and one radical cystectomy with ureterocutaneostomies. Perioperative data were prospectively collected and analyzed.
Results:
The transition from 2D to 3D laparoscopy for the expert surgeon seemed to be very rapid without compromising the efficacy of the operation or patient safety. Perioperative outcomes and complications resembled the outcomes of our 2D experience.
Conclusions:
Our preliminary experience with 3D laparoscopy was favorable, and we definitely opt for 3D vision in future operations. Nevertheless, current systems are related to several technical limitations that should be addressed to make even more appealing the further development of this technology. Whether the visual comfort offered by 3D vision during laparoscopy can be translated into an improvement in clinical outcomes offered to patients remains to be addressed in the future.
Introduction
S
Three-dimensional (3D) laparoscopy has been developed in an attempt to address one of the main limitations of laparoscopic surgery, which is 2D vision. The latter is associated with an impaired perception of depth and disturbed eye-hand target axis. 3 Current 3D laparoscopic technology offers a high-definition 3D image and aims to restore stereoscopic vision during conventional laparoscopic surgical procedures, providing a similar optical experience with open surgery. Still, data on the learning curve during adaptation of such technology in clinical practice are scarce.
In this study, perioperative data from the initial operations performed by an experienced laparoscopic surgeon in a 3D laparoscopic setup are presented, aiming to document any difficulties faced during the integration of 3D vision to laparoscopy.
Patients and Methods
During the first month of 3D laparoscopic system acquisition from our department, 15 unselected, consecutive patients underwent a 3D laparoscopic surgical procedure by a single expert laparoscopic surgeon (EL). Perioperative data including patient age and sex, type of operation, operative time (skin incision to skin closure), estimated blood loss (EBL), pre- and postoperative hemoglobin count, hospital stay, intra- and postoperative complications were prospectively collected. The Clavien-Dindo grading system was used for the classification of surgical complications. 4
A 0°-degree and a 30-degree 10-mm 3D-TIPCAM® laparoscopes (Karl Storz, Tuttlingen, Germany) equipped with “chip on the tip” technology were used. The cameras were connected to a 3D camera control unit, and the image was displayed on a medical-grade 32″ HD monitor capable of displaying 2D and 3D images (Karl Storz). Polarized glasses were used by all theater personnel to achieve stereoscopic imaging.
Results
Five women and 10 men were operated on using 3D laparoscopy within a 30-day period. Mean patient age was 69 years (range 57–91 years). The cases included five laparoscopic extraperitoneal radical prostatectomies (LERP), three nephrectomies, three partial nephrectomies (PN), one nephrouretectomy (NU), one adrenalectomy, one ureterolithotomy, and one radical cystectomy with ureterocutaneostomies.
All LERPs were nerve sparing, and none included pelvic lymph node dissection. Mean operative time for LERP was 80 minutes (range 63–102 min). Blood loss was minimal, and none of the patients needed blood transfusion. No intraoperative complications were observed. Urinary retention from clot occlusion of the indwelling catheter that caused anastomotic urinary leakage was observed in one patient postoperatively (Clavien-Dindo grade I). This caused a prolonged hospitalization of up to 5days without necessitating additional intervention.
Three laparoscopic (one simple and two radical) nephrectomies took place. One was performed for a nonfunctioning kidney and the rest for pT2 renal-cell carcinoma (RCC). Mean operative time for nephrectomy procedures was 56 minutes, (range 45–78 min), and blood loss was negligible. The patients did not have any intraoperative or postoperative complications. One NU was performed because of a pT2 RCC and a concomitant ureteral stone near the ureterovesical junction. The procedure was completed in 149 minutes with an EBL of 300 mL because of bleeding from an adrenal vessel during operation. This resulted in a hemoglobin drop of 0.9 g/dL without the need for blood transfusion. The postoperative course was uneventful.
All three PNs were performed in a clampless fashion without ischemia. Tumors were enucleated with a concomitant use of harmonic scalpel and bipolar coagulation. Despite the absence of bleeding from the tumor bed after tumor excision, a sliding clip renoraphy was performed in all cases in accordance with our standard protocol. Mean operative time was 107 minutes (range 93–124 min), and blood loss was minimal in all cases. No intra- or postoperative complications were observed. No alteration in creatinine levels was observed postoperatively. All three patients had negative surgical margins.
Cystectomy was performed for muscle invasive bladder cancer. The comorbidities and the advanced age of the patient (90 years old) led to the selection of ureterocutaneostomies as the most appropriate urinary diversion. The procedure lasted 220 minutes, and EBL was 300 mL. Postoperative ileus was encountered (Clavien-Dindo grade II) and resided with conservative management. After normalization of bowel motility, the patient was discharged on postoperative day 7.
A laparoscopic adrenalectomy was performed on a 76-year old woman for a 6 cm adrenal tumor. The procedure necessitated 98 minutes without any complications. EBL was 150 mL. The patient was discharged on postoperative day 2.
A ureterolithotomy was performed on a male patient with a large midureteral stone of 4 cm in diameter. The operation was uneventful, and needed 62 minutes with negligible blood loss. The patient was discharged on postoperative day 1. A pigtail catheter was left in place and removed after 1 month. Perioperative data of patients included in this cohort are summarized in Table 1. In addition, comparative data from our 2D experience including the last 10 2D LERP, the last 10 2D laparoscopic PN, and the last 10 2D nephrectomies are demonstrated in Table 2 as a surrogate marker of competiveness between the two approaches. Relative data from our 2D experience in adrenalectomy, NU, and cystectomy were not added, given that only one case was performed for each kind of operation and direct comparison would be biased.
Pts=patients; OT=operative time; EBL=estimated blood loss; TRF=transfusion; Hosp=hospitalization; CD=Clavien-Dindo classification; LERP=laparoscopic extraperitoneal radical prostatectomy; N=nephrectomy; PN=partial nephrectomy; NU=nephrouretectomy; Cyst=radical cystectomy; A=adrenalectomy; U=ureterolithotomy.
Data drawn from the last 10 patients operated on in a 2D system before 3D experience.
2D=two-dimensional; 3D=three-dimensional.
Discussion
Although the first 3D laparoscopy systems were introduced three decades ago, their adaptation by laparoscopic surgeons was restricted by side effects associated with their use. These side effects included early onset of fatigue, induction of headache, and blurring of the eyes. 5 –7 Boosted by the wide experience gained by 3D vision during robot-assisted surgical procedures, a newer generation of 3D laparoscopic systems became available that entails superior image quality. Our department gained early access to one of these systems, and we herein document our initial experience.
Overall, our practice with the 3D vision during laparoscopy was favorable. Spatial perception was combined with excellent image resolution and fidelity. Within the first 30 minutes of the first operation, the expert surgeon and his assistants felt comfortable operating in the 3D setting. The surgeon became more familiar with the 3D vision as our experience progressed. The latter observation is evident on the operative time of LERP where a plateau of approximately 60 minutes, which is similar to our operative times on 2D LERP, was achieved after the fourth procedure (Fig. 1). Overall, surgeon comfort was not compromised at any stage of adaptation in 3D technology. Motion sickness was not experienced by surgical staff and, after the first cases, no real difference between our 2D or 3D experience was evident apart from a superior image and depth perception associated with 3D vision.
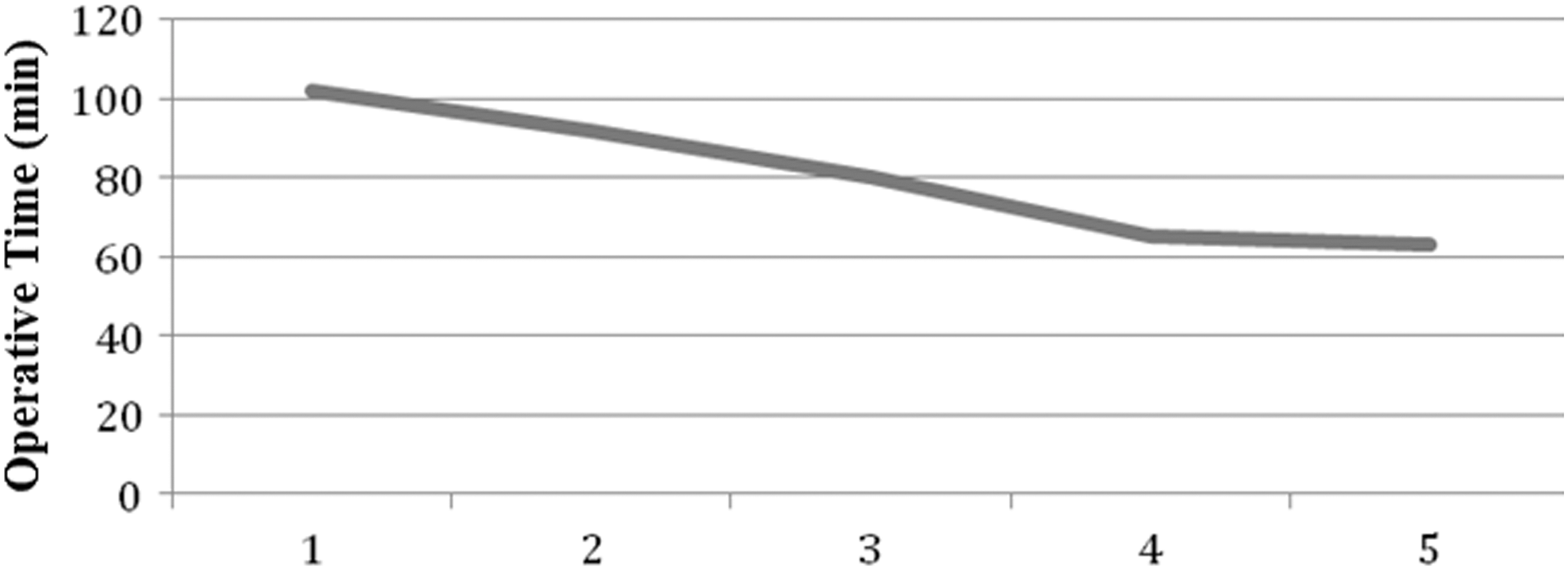
Operative times in the five patients who underwent laparoscopic extraperitoneal radical prostatectomy. Patients one to five appear in the order in which the operations occurred.
The benefits of 3D vision during laparoscopy were more evident in operations necessitating intracorporeal suturing (radical prostatectomy, PN, ureterolithotomy). Easy orientation of the needle and superior handling of the suture were noted. The learning curve for the transition from 2D to 3D did not compromise the safety of the patients, and the latter was documented by the low EBL and low complication rates regardless of the procedure. The hospital stay was similar to our experience with each of the included procedures. As a result, we could advocate that the 3D environment is safe and efficient for the performance of laparoscopic surgery in the hands of an expert surgeon even if the surgeon uses a 3D laparoscopic system for the first time.
Despite the technologic advancement of the new generation 3D systems, there are still several drawbacks associated with their use. Proper crystal clear 3D vision is achieved only by viewing the monitor within a restricted angle range and a straight axis to the monitor. As a result, the adjustment of the monitor for surgeon preferences results in nonoptimal viewing angles, blurred vision, and fatigue for the assistants and operating room personnel. Multiple monitors spread within the theater might solve this problem.
In addition, the 3D system has been developed to optimally focus on a particular distance away from the camera. Thus, objects in the vicinity of the camera appear blurred, and any reflection of the light is amplified causing further disturbance in the vision of the operating team. Consequently, vision of trocars during insertion, instrument shaft in close proximity with the camera, or even smoke released on the surgical field resulted in significantly impaired vision. Switching to 2D vision during trocar insertion prevented the aforementioned disturbance during trocar placement, and only when all instruments were in place was the 3D vision turned on. Finally, movement of the head while viewing the monitor causes movement of the visual objects on the screen. As a result, staying steady during monitor viewing was mandatory to avoid motion sickness. Despite the above mentioned limitations of 3D laparoscopy, the authors favored the use of the 3D laparoscopic system and it has been preferred ever since whenever it is available.
There is an ongoing debate regarding the superiority of 3D over conventional 2D laparoscopy because the evidence to support the advantages of 3D vision in the clinical setting is currently lacking. 8 Some surgeons consider that 3D laparoscopy improves perception of depth, surgical precision, and space orientation, where others do not find it to be superior to conventional 2D laparoscopy, especially when its impact on the performance of expert surgeons is considered. 9 –13 Similarly, data from this study cannot support the superiority of 3D over 2D laparoscopy given that no improvements in perioperative outcomes of each operation were noted compared with our previous 2D experience.
The latter might be explained by the fact that 3D vision appears to have a greater impact on novice rather than expert surgeons. Cicione and colleagues 13 examined the differences on the performance of novice and expert laparoscopic surgeons on 2D and 3D environment in a laboratory setting and documented that those with previous laparoscopic experience did not subjectively recognize an advantage with the use of the 3D system. In contrast, a significant improvement in performance of novice surgeons was observed. 13 Based on the above, 3D laparoscopy might ease the steep learning curve of laparoscopy and have a greater impact in the performance of novice surgeons. In the case of expert laparoscopic surgeons, the benefits of 3D vision may be limited to a more favorable surgical field vision with no effect on perioperative outcomes.
Nevertheless, 3D laparoscopy can be considered to be in its infancy, and more mature data on 3D outcomes are necessary to draw safe conclusions regarding the role of this technology in laparoscopic surgery. Still, in the era of economic burdens in healthcare systems, currently documented improved visual experience might not be enough to justify the purchase of such a system unless translation into improved clinical effectiveness is documented.
A significant limitation of the current study is that all procedures were executed by a very experienced laparoscopic surgeon. In addition, the particular surgeon had previous experience in robotic surgery and consequently he had been familiarized with 3D laparoscopic vision. As a result, it is possible that a longer learning curve might be expected in less experienced surgeons or in surgeons experiencing 3D laparoscopy for the first time. Still, the ability of the surgeon and his assistants (who had no 3D experience in the past) to feel comfortable after a few minutes in the 3D setup indicates that transition from 2D to 3D should not be expected to be steep.
An additional limitation is the small number of patients undergoing operation in the current series. Reliable conclusions can be drawn only for LERP where five patients underwent operation. The consistent homogenous performance as indicated by operative times resembling the performance of the surgeon in a 2D environment documented that transition to 3D did not compromise the outcomes of surgery (Table 2). Further investigation including the learning curve data from surgeons of varying experience performing the whole range of laparoscopic urological surgical procedures in a larger case series is deemed necessary to draw safe conclusions.
Conclusion
Current 3D systems provided excellent perception of depth and spatial resolution. The transition from 2D to 3D laparoscopy for the expert surgeon seemed to be very rapid without compromising patient safety. Our preliminary experience with 3D laparoscopy was favorable, and we definitely opt for 3D vision in future operations. Nevertheless, current systems have several technical limitations that should be addressed to make even more appealing the further development of this technology. Whether the visual comfort offered by 3D vision during laparoscopy can be translated into an improvement in clinical outcomes offered to patients remains to be addressed in the future.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.