
Abstract
Background and Purpose:
Prolonged operative time (ORT) is often considered a drawback to minimally invasive surgery (MIS) because of increased morbidity. Limited data exist comparing long laparoscopic ORT with similar or shorter open ORT. This study aims to identify ORT when a minimally invasive procedure becomes inferior to its open counterpart.
Methods:
Minimally invasive and open total and partial nephrectomies and nephroureterectomies were identified in the National Surgical Quality Improvement Program (NSQIP) from 2005 to 2012. Procedures were split into open and minimally invasive nephrectomy and then stratified into four ORT groups: 0 to 90 minutes, 91 minutes to 3 hours, 3 to 6 hours, and ≥6 hours. Thirty-day mortality and morbidity were analyzed. Univariate analysis was performed using chi-square and Fisher exact tests. Significant univariate results were then tested using stepwise logistic regression, controlling for demographics, comorbidities, and preoperative treatments.
Results:
There were 14,813 patients identified. Both partial and total minimally invasive kidney procedures had significantly improved outcomes compared with open counterparts of similar ORT. In the total nephrectomy group, a minimally invasive approach had a lower rate of surgical site infections, sepsis, pneumonia, return to operating room, and overall length of stay when compared with open procedures of the same duration. Length of hospital stay decreased in MIS regardless of operative time, except when comparing minimally invasive cases longer than 6 hours with open cases less than 90 minutes. Transfusion rates also significantly decreased in minimally invasive total nephrectomy cases. In the partial nephrectomy group, similar outcomes were seen in terms of length of stay and infectious outcomes. Interestingly, transfusion risk was decreased in the open partial nephrectomy group when comparing cases less than 90 minutes with minimally invasive partial nephrectomies lasting 3 to 6 hours; otherwise there was no significant correlation with transfusion risk.
Conclusions:
Minimally invasive operations are less morbid than open operations of similar ORT. Longer and likely more complex laparoscopic procedures continue to provide a benefit to patients when compared with shorter and possibly less complex open procedures. These data should be considered during a surgeon's preoperative and operative decision-making.
Introduction
K
With the increasing use of minimally invasive techniques for the management of RCC, the complications and outcomes of laparoscopic and open procedures for RCC have been extensively studied. Prolonged operative time (ORT) is often deemed a shortcoming of laparoscopy, given the pervasive notion that prolonged surgical time is associated with increased complications. 6 The goal of this study is to determine the ORT when laparoscopic procedures become more morbid than similar open procedures.
Methods
A retrospective analysis of the National Surgical Quality Improvement Program (NSQIP) database was completed using International Classification of Diseases-9 codes to identify patients undergoing nephrectomies (partial, total, nephroureterectomies) between 2005 and 2012. NSQIP is a nationally validated, risk-adjusted, outcomes-based program that records morbidity and mortality outcomes in the 30-day perioperative period. The data are collected by surgical clinical reviewers who review medical charts and contact patients, yielding a 95% success rate in capturing all outcomes within 30 days in all the cases in the database.
NSQIP has 435 hospitals that participate in collecting data, including tertiary care and academic centers, Kaiser hospitals, military hospitals, as well as a healthy representation of community and rural hospitals. Operations were divided into two categories to account for differences in operative outcomes: Total nephrectomies and partial nephrectomies. They were also divided by operative approach: Laparoscopic and open. Outcomes examined included mortality, sepsis, renal complications, cardiac complications, length of stay longer than 7 days, pulmonary embolism, deep vein thrombosis, surgical site infection (SSI), pneumonia, reintubation, peripheral neuropathy, return to the operating room, and transfusion. Patients were excluded from multivariate analysis if any of the demographic or comorbidity variables were unavailable or if they were coded as both partial and total nephrectomy.
Cases were stratified into four groups based on ORT: Less than 90 minutes, 91 minutes to 3 hours, 3 to 6 hours, and greater than 6 hours. Morbidity and mortality outcomes were analyzed comparing each minimally invasive ORT group with equal or shorter open procedures. Ordinal time groups were used instead of a continuous variable to look at associations between treatment groups and outcomes by comparing combinations of time groups for laparoscopic vs open treatment. In addition, this allows examination of the possibility that the association of treatment with outcome may not have a linear association with time. The time groups were chosen in a manner to allow an approximately normal distribution in number of cases around the four time groupings.
Statistical analysis
For each outcome, prevalence rates were compared between laparoscopic and open treatment at each ORT category using chi square and Fisher exact tests. To correct for any possible confounding variables, a stepwise logistic regression model was used with a cut-point of P<0.20 to enter or exit from the prediction model for each outcome.
Along with the treatment variable of laparoscopic or open approach, other covariates that were permitted to enter the equations included: Sex, age, race, smoking, alcohol consumption, American Society of Anesthesiologists score 4 or 5, surgery in the past month, sepsis, nonindependent functional status, dyspnea, diabetes, ventilator dependence, history of chronic obstructive pulmonary disease, congestive heart failure, myocardial infarction, angina, hypertension, peripheral vascular disease, rest pain or gangrene, pneumonia, previous percutaneous cardiac intervention, previous cardiac surgery, ascites, esophageal varices, acute kidney injury, dialysis, impaired sensorium, coma, cerebral vascular accident, central nervous system tumor, paraplegia or quadriplegia, disseminated cancer, SSI, chronic use of steroids, weight loss of greater than 10% of body mass in 6 months, bleeding disorder, transfusion, use of chemotherapy or radiotherapy, weight, body mass index.
Laboratory results were also accounted for including: Levels of bilirubin, albumin, sodium, blood urea nitrogen, creatinine, serum glutamic oxaloacetic transaminase, alkaline phosphate, white blood cell count, platelet count, partial thromboplastin time, and international normalized ratio, with missing laboratory values set at the mean. Statistical significance for univariate tests was defined as a P value less than 0.05. Because a large number of multivariate tests were performed, a Bonferroni correction was used in the multivariate tests to correct for multiple testing and reduce the overall false-positive rate.
Results
Between 2005 and 2012, 14,813 nephrectomies were completed including 9591 total nephrectomies and 5222 partial nephrectomies. A minimally invasive approach was used in 52% of total nephrectomies and 53% of partial nephrectomies. Eighty-five percent of nephrectomies were completed in 91 minutes to 6 hours, including 81% of total nephrectomies and 90% of partial nephrectomies (Table 1).
Percentages reflect the percentage of cases in the time grouping for each approach for total and partial nephrectomy; for example, the percentage of laparoscopic total nephrectomy occurring in less than 90 minutes in the total nephrectomy group.
Lap=laparoscopic; N=total number of cases.
Total nephrectomy
Laparoscopic and open total nephrectomies of similar ORTs were compared. In all periods, the laparoscopic approach was found to be equivalent or superior to the open approach. Mortality was equivalent in laparoscopic and open total nephrectomies, with no variation based on ORT. The laparoscopic approach was significantly associated with decreased hospital length of stay for all cases lasting more than 90 minutes. Open cases greater than 90 minutes had a significantly longer hospital stay, even when compared with laparoscopic cases that were more than 3 hours. Transfusion requirement was also significantly increased for open cases lasting 90 minutes to 3 hours. In operations lasting 3 to 6 hours, events of sepsis, pneumonia, and SSI decreased with the laparoscopic approach. The frequency of return to the operating room was significantly decreased in laparoscopic cases lasting 91 minutes to 3 hours when compared with open cases of the same length (Table 2).
Test: Multivariate regression.
Statistically significant Bonferroni P=0.00042.
ORT=operative time; NA=odds ratio cannot be calculated because of no events in one treatment group; DVT=deep vein thrombosis.
When compared with shorter open operations, longer laparoscopic operations were found to have adverse outcomes only when open total nephrectomy was completed in 90 minutes or less. Both transfusion requirements and prolonged hospital length of stay were decreased with the open approach for cases completed in less than 90 minutes compared with the laparoscopic operations longer than 6 hours. All other outcomes were equivalent or superior with the laparoscopic approach. Transfusion requirements and hospital length of stay were both decreased by the laparoscopic approach in cases lasting more than 3 hours when compared with shorter open operations (Table 2). The net outcomes of all laparoscopic and total nephrectomies are depicted in Figure 1.
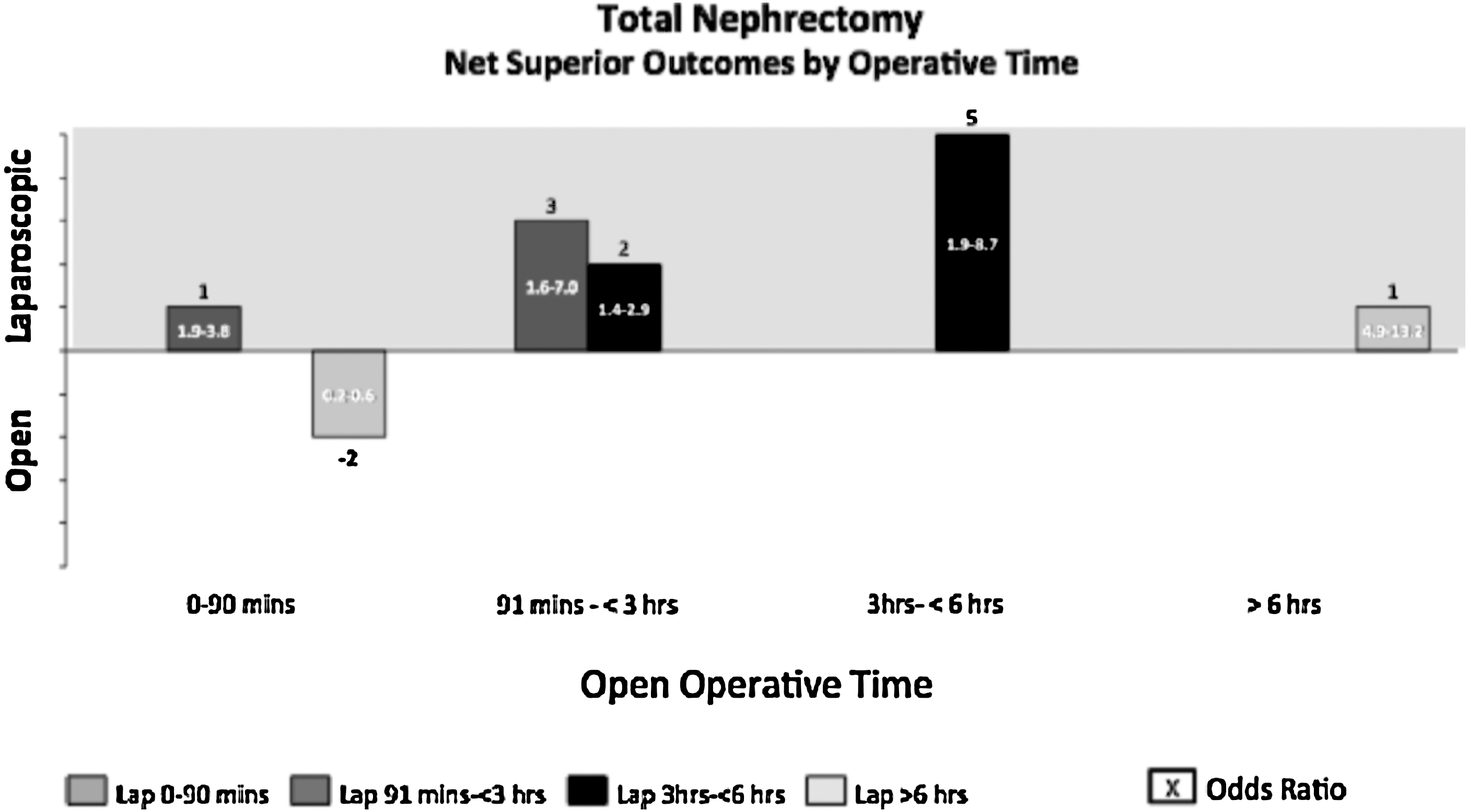
Total nephrectomy: Net superior outcomes by operative time. Lap=laparoscopic.
When all outcomes were evaluated, only six outcomes (SSI, sepsis, pneumonia, transfusions, return to the operating room, and length of stay) were affected by length of procedure. Mortality, deep venous thrombosis, pulmonary embolism, reintubation, renal and cardiac complications were all unaffected by ORT in the context of the open vs laparoscopic approach (Table 2).
Partial nephrectomy
Partial nephrectomies of equivalent ORTs were compared. The minimally invasive approach had superior or equivalent outcomes at all ORTs. Hospital length of stay was the most significantly impacted by the minimally invasive approach with improved outcomes for all cases lasting greater than 90 minutes. The minimally invasive approach also significantly improved sepsis rates and SSIs for cases lasting 3 to 6 hours. Mortality was not affected by the operative approach regardless of operative time (Table 3).
Test: Multivariate regression.
Statistically significant Bonferroni P=0.00058.
The minimally invasive approach is associated with decreased hospital length of stay compared with shorter open partial nephrectomies. Minimally invasive operations lasting 91 minutes to 3 hours have decreased length of stay compared with shorter open operations. Hospital length of stay was also decreased in minimally invasive operations lasting 3 to 6 hours when compared with open operations 91 minutes to 3 hours. The only outcome found to be improved by the open approach was transfusion requirement. Minimally invasive partial nephrectomies lasting 3 to 6 hours have a greater transfusion requirement compared with open partial nephrectomies less than 90 minutes (Table 3).
Figure 2 depicts the net outcomes of all minimally invasive and open partial nephrectomies. The benefits of minimally invasive surgery (MIS) are significant across all open ORTs. Only one outcome (transfusion requirement) was improved in the open approach lasting less than 90 minutes compared with a longer minimally invasive approach.

Partial nephrectomy: Net superior outcomes by operative time.
ORT and approach had a significant impact on transfusion requirement, hospital length of stay, sepsis, and SSIs. Venous thromboembolism, return to the operating room, pulmonary, renal, and cardiac complications were all unaffected by ORT and approach.
Discussion
Approximately 50% of kidney operations between 2005 and 2012 were performed in a minimally invasive fashion. Over the past several years, advances in MIS, including the availability of new tools to aid in intracorporeal suturing, hemostatic agents, and the more prevalent use of robotics, have increased the acceptance and practice of minimally invasive techniques for kidney surgery including nephron-sparing surgery. 7,8 The increasing use of minimally invasive techniques for partial nephrectomies was approximated at 50% in 2011. 9 This speaks to the growing popularity of minimally invasive techniques for the performance of kidney procedures. The use of partial nephrectomy in our article was approximately 35%, which is similar to reports of population-based studies in 2010. 10
Laparoscopic radical nephrectomy became the standard of care for treatment of patients with RCC after studies found equivalent oncologic outcomes to the open approach. 11 With the emergence of partial nephrectomy as the standard of care for small renal masses and the availability of radiofrequency ablation and cryoablation, laparoscopic nephrectomy has recently been used more in the removal of larger tumors. 12 Historically, documented advantages of laparoscopic radical nephrectomy included decreased blood loss, less pain, better cosmesis and convalescence, and shorter hospital stays. 11,13 After thorough review of the surgical literature, the effect of prolonged ORTs on these previously reported benefits has not been addressed.
Our study suggests that the laparoscopic approach to total nephrectomy has superior or equivalent outcomes to the open approach regardless of ORT, with the exception of transfusion requirement and length of stay in open cases lasting less than 90 minutes. These “extreme operative time” cases (less than 90 minutes or more than 6 hours) constitute less than 20% of total nephrectomies performed. In laparoscopic operations longer than 6 hours, only one outcome was inferior when compared with the open approach completed in less than 90 minutes, and all other outcomes were equivocal.
The benefits of the laparoscopic approach are greatest in operations lasting 91 minutes to 6 hours. This is of significant clinical importance given that the vast majority of all total nephrectomies performed fall into this group. When open and laparoscopic operations of equal times were compared, the laparoscopic approach was superior in all operations lasting longer than 90 minutes (Fig. 1).
Recently, several large series have compared the outcomes of open and minimally invasive partial nephrectomy. Historically, a significant number of adverse outcomes were seen with laparoscopic partial nephrectomy when compared with the open approach. More recent literature, however, has demonstrated a complication rate to be much more comparable, with hemorrhage and urine leak found to be the most frequent complications associated with laparoscopic partial nephrectomy—5% and 4.2%, respectively. 14
In more recent years, the use of the robot has become increasingly prevalent as an adjunct to laparoscopic partial nephrectomy. 14 A recent meta-analysis compared robot-assisted and open partial nephrectomies and demonstrated significantly lower rates of adverse outcomes in patients undergoing a robot-assisted partial nephrectomy despite longer ORT. Although the nature of these complications was not revealed, the length of hospital stay and rate of transfusion were significantly decreased in robot-assisted partial nephrectomies. 15 Conversely, in other reviews, a greater risk of delayed hemorrhage and increased rate of additional procedures can be attributed to the technical challenges that come with laparoscopic partial nephrectomy. 16
The outcomes seen in the partial nephrectomies evaluated in this study are similar to those in the total nephrectomy group. Sepsis and SSIs are both significantly improved for laparoscopic operations lasting 3 to 6 hours compared with the open operations. Hospital length of stay is also significantly improved with laparoscopic procedures lasting longer than 90 minutes in both partial and total nephrectomies. Although this has been seen in many studies, there is no consensus as to why this is the case. The result is likely multifactorial in nature. The placement of the open incision may increase length of hospital stay because of suboptimal pain control and pulmonary effects of a midline or flank incision. In these data, a decrease in transfusion requirement was seen in patients undergoing an open partial nephrectomy completed in less than 90 minutes when compared with a laparoscopic partial nephrectomy that is completed in 3 to 6 hours.
It has been shown in the past that tumors that are considered more complex by standard scoring systems such as the nephrometry score are significantly more likely to have major complications after partial nephrectomy, especially urine leak and hemorrhage. 17 It may be reasonable to assume that open partial nephrectomies that can be completed in less than 90 minutes are likely to have less complex tumors.
Complexity of a procedure has a significant effect on ORT regardless of approach. Prolonged ORTs in either the open or laparoscopic approach likely reflect a more tedious dissection, intraoperative complication, or complex case. Unfortunately, NSQIP does not stratify operative complexity, and ORT can be used as a surrogate. This has important implications in our data because for similar operative periods, the laparoscopic approach has equivalent or improved outcomes. Furthermore, longer laparoscopic cases and conceivably more complex procedures continue to have improved outcomes when compared with shorter and likely less complex open procedures.
Currently, no urologic studies have directly assessed the result of prolonged operative time on surgical outcomes. Our data, however, suggest that both total and partial nephrectomies have improved outcomes and no effect on mortality when completed using a minimally invasive approach compared with equal or shorter open procedures. In addition, shorter open operations do not provide beneficial results to patients in more than 80% of cases.
Surgeons should consider estimated ORT when counseling patients preoperatively and consider using an open approach if they anticipate a laparoscopic case necessitating more than 6 hours of ORT. Many factors alter the expected outcomes, including patient factors and comorbidities, tumor characteristics, previous surgeries, as well as provider factors, such as experience, use of new tools, and trainee involvement. These considerations are multifactorial and estimated ORT should be included among these factors.
Limitations
Our study carries the usual limitations of retrospective analysis and those involved in using the NSQIP database. Tumor characteristics including size, location, and indication for the procedure are not included, and this is an inherent limitation of the database. Although this is the case, other available patient characteristics that would add to surgical complexity were controlled. Outcomes only include those variables in the database of participating hospitals. In addition, outcomes are not evaluated beyond 30 days. Although this is a limitation, it has been shown that most complications of nephrectomy will occur within 30 days of surgery. 18 Moreover, these data may be more representative of practices at academic centers, which represent a high proportion of reporting NSQIP hospitals, 19 leading to conclusions that may not be generalizable.
Surgical expertise perceptibly affects postoperative complications rates as does the use of the robot. These two factors are unable to be differentiated due to limitations of the database. In recent years, the robot has become widely used in the performance of partial nephrectomies. 14 Finally, there is a lack of information about case complexity. We can deduce that longer ORTs may indicate that the case has a more complex tumor or patient factors.
Conclusion
Laparoscopic partial and total nephrectomies are associated with improved morbidity compared with the open operations of equal and shorter ORT without an effect on mortality. Longer and likely more complex laparoscopic procedures continue to provide a benefit to patients when compared with shorter and possibly less complex open procedures. Estimated ORT should be considered when planning the operative approach and in preoperative patient counseling.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.