
Abstract
Purpose:
To compare outcomes in patients treated with radiofrequency ablation (RFA) and partial nephrectomy (PN) for clinical T1a renal-cell carcinoma (RCC) in a propensity-score matched cohort.
Methods:
We conducted a retrospective review of the records of all patients who underwent RFA or nephrectomy between February 2005 and December 2009 in our institution. The Kaplan-Meier method was used to generate the survival curves that were compared with the log-rank test. Univariable and multivariable regression analyses were performed to determine predictors of survival.
Results:
A total of 90 patients were included in the final study after being matched by propensity scores (RFA 45; PN 45). The 5-year overall survival (95% confidence interval [CI]) was 90.2% (78.6–98.8) vs 93.2% (85.8–98.9); 5-year cancer-specific survival (95% CI) was 95.6% (89.5–98.1) vs 97.7% (93.4–99.3); 5-year disease-free survival (95% CI) was 86.7% (89.5–96.7) and 88.5% (79.1–97.9); 5-year recurrence-free survival (95% CI) was 95.4% (89.3–98.1) vs 97.7% (93.3–99.2); and 5-year metastasis-free survival (95% CI) was 95.5% (89.4–98.0) vs 95.5% (89.4–98.0). Age was the only factor that could predict the disease-free survival (P=0.044). The percentage decrease in the glomerular filtration rate was significantly lower in the RFA group at the time of last follow-up (P=0.001).
Conclusions:
In the propensity-score matched cohort of patients with clinical T1a RCC, we observed that RFA was an effective treatment option that provided comparable 5-year oncologic outcomes and better preservation of renal function than PN.
Introduction
W
For the sake of minimally invasive therapy and maximally preserved renal function, ablative therapy in the form of cryoablation, radiofrequency ablation (RFA), microwave ablation, and irreversible electroporation have been proposed in selected candidates. As ablative technologies continue to be increasingly proposed as a standard treatment modality, the role of histopathologic and immunohistochemical analysis through renal biopsy will be beneficial in determining the accurate diagnosis and the possible best definitive treatment approach (e.g., an ablative, nonextirpative procedure or surveillance). 3
Ablative procedures are recommended in the management of small renal-cell carcinomas (RCC) for patients with an advanced age, those with significant comorbidities who are poor surgical candidates, or those who are not willing to undergo extirpative surgery. 4 RFA has been increasingly accepted as an alternative effective nephron-sparing technique in the management of small RCCs. Currently, the American Urological Association guidelines have recommended RFA as an option for patients with stage T1 RCCs, especially those with clinical T1a RCCs. 5
Several retrospective studies have concluded that RFA has a relatively high local control rate and similar cancer-specific and disease-free survival rates compared with those of nephrectomy in the management of clinical T1a RCCs. 6,7 It is difficult to draw conclusions, however, according to the retrospective and unmatched cohort comparisons because treatment groups differed significantly by age, sex, American Society of Anesthesiologists (ASA) score, and so on.
We have therefore performed a propensity score matching comparison to mimic a randomized trial between RFA and PN for clinical T1a RCCs to provide more reliable information on perioperative and long-term oncologic outcomes.
Materials and Methods
Patients
Institutional Review Board approval was obtained to review retrospectively the medical records of the patients who underwent either RFA or PN for small renal masses between February 2005 and December 2009 at our hospital. Only patients with a localized tumor measuring no more than 4.0 cm (clinical T1a) in maximum diameter that was pathologically confirmed to be RCC and a minimum postoperative follow-up of 5 years were included in our study. Patients with multiple ipsilateral, metachronous, synchronous bilateral tumors or distant metastatic diseases were excluded from the present study. In addition, those who had a familial history of RCC or a history of hereditary RCC syndromes were also excluded.
Patients with significant comorbidities, a solitary kidney, or tumors in unresectable locations were recommended treatment with RFA. Those who were not willing to take the risk of PN were also included in the RFA treatment cohort of their own accord. Informed consent to perform either of the treatment modalities (RFA or PN) was obtained from each patient.
Surgical techniques
A laparoscopic or percutaneous approach was applied in the RFA cohort and PN was performed under an open or laparoscopic condition. Tumor location, tumor size, history of previous abdominal surgery, surgeon judgment, and patient preference were taken into consideration when choosing the surgical approach.
Our techniques for laparoscopic RFA and percutaneous RFA have been described previously. 8,9 Ultrasonography was used intraoperatively to determine the tumor location and guide the placement of the electrodes. To reveal the preoperative outline of the tumor, contrast-enhanced ultrasonography (CEUS, B/K, Denmark) was performed before RFA. After biopsy (TruCore, 22G), several cycles of RFA procedures were performed with the help of a Cool-tip system (Radionics, Burlington, MA). Another intraoperative CEUS was given to evaluate whether the previous ablation was efficient right after the previous ablation. Extra cycles of ablation were adopted at the surgeon's discretion if the previous ablation was considered incomplete on visual inspection or the image of CEUS.
When it came to PN, perirenal fat was dissected off the kidney, and only the fat overlying the tumor was left. The renal artery and vein were also dissected for the possibility of hilum clamping at the surgeon's discretion. During laparoscopic PN, laparoscopic ultrasonography was used to locate the tumor and simultaneously reveal the outline and depth of the tumor. After tumor excision with cold scissor, the tumor bed was coagulated with bipolar forceps and closed using 3-0 polyglactin sutures, and then the renal defect was closed using 2-0 polyglactin sutures.
Follow-up
The patient follow-up after RFA included history review, physical examination, chest radiography, contrast-enhanced CT, or enhanced MRI, serum chemistries, serum creatinine determination, liver function tests, and emission CT for bone scanning if necessary. Contrast-enhanced CT assessment was made at 7 days, 3 months, 6 months, and every 6 months sequentially after RFA. Enhanced MRI was applied in patients who had renal insufficiency or contrast agent allergy. The ablation was considered successful when the lesion showed less than 10 Hounsfield units (HU) of contrast medium enhancement on CT or no qualitative evidence of enhancement on enhanced MRI. Any new enhancement (>10 HU) found during a nonenhanced scan was defined as recurrence. 10
The follow-up protocol of PN was similar to that of RFA, except that the interval was every 6 months in the initial 3 years and annually thereafter. Preoperative glomerular filtration rate (GFR) was compared with the GFR at the last follow-up. Estimated GFR was calculated using the modified Modification of Diet in Renal Disease equation. 11
Statistical analysis
Demographics as well as perioperative data were analyzed using the Student t test for continuous and ordinal variables, and the chi-square test for categorical variables. The propensity score was built by way of a multivariable logistic regression model considering the following variables: Age, sex, ASA score, tumor size, tumor side, tumor histology, R.E.N.A.L. (radius; exophytic/endophytic; nearness; anterior/posterior; location) nephrometry score, and preoperative GFR.
The overall survival (OS), cancer-specific survival (CSS), disease-free survival (DFS), recurrence-free survival (RFS) and metastasis-free survival (MFS) were respectively defined as the proportion of patients who did not die from any cause, the proportion of patients who did not die from any cancer including RCC, the proportion of patients free from any disease, and the proportion of patients free from local recurrence or metastatic recurrence.
The Kaplan-Meier method was used to generate the survival curves, which were compared with the log-rank test. Univariable and multivariable regression analyses were performed to determine predictors of survival. All statistical analyses were performed using IBM SPSS vol. 19.0 (Chicago, IL) with a P value<0.05 considered statistically significant.
Results
Table 1 shows patient demographics and tumor characteristics of the initial study cohort of 268 patients before and after they were matched according to their propensity to undergo RFA. A total of 134 patients in each group underwent RFA or PN. Before propensity-score matching, there were more male patients in the RFA group than those in the PN group (P=0.027). The patients in the RFA group had a relatively higher mean ASA score than those in the PN group (P<0.001). The mean preoperative tumor diameter was significantly larger in the PN cohort (P=0.004). All the other patient demographics and tumor characteristics showed no significant differences in Table 1 between the two groups before the propensity-score matching.
RFA=radiofrequency ablation; PN=partial nephrectomy; ASA=American Society of Anesthesiologists; GFR=glomerular filtration rate; MDRD=Modification of Diet in Renal Disease.
As to perioperative outcomes shown in Table 2, patients in the PN cohort had larger estimated blood loss (P<0.001), longer operative time (P<0.001), and larger percentage change in GFR in the last follow-up (P=0.005). Even though the PN group seemed to have a longer hospital stay and more major complications (Clavien system: ≥IIIa), there were no significant differences between the two groups (P=0.110 and 0.776, respectively).
PS=propensity score; PN=partial nephrectomy; EBL=estimated blood loss; OT=operative time; PCG=percentage change in glomerular filtration rate; HS=hospital stay; MC=major complications.
After being matched by propensity scores (Fig. 1), 45 patients for each group met the matched criteria and were included in the final study (Fig. 2). Within the propensity-score matched cohort, all the patient demographics and tumor characteristics between the two groups had no significant differences (P>0.05). The RFA group was associated with significantly lower estimated blood loss (74.8±50.8 mL vs 243.3±284.8 mL, P<0.001) and shorter operative time (132.6±24.9 min vs 171.5±32.4 min, P<0.001). No patients in the PN group underwent renal ischemia during the procedure.
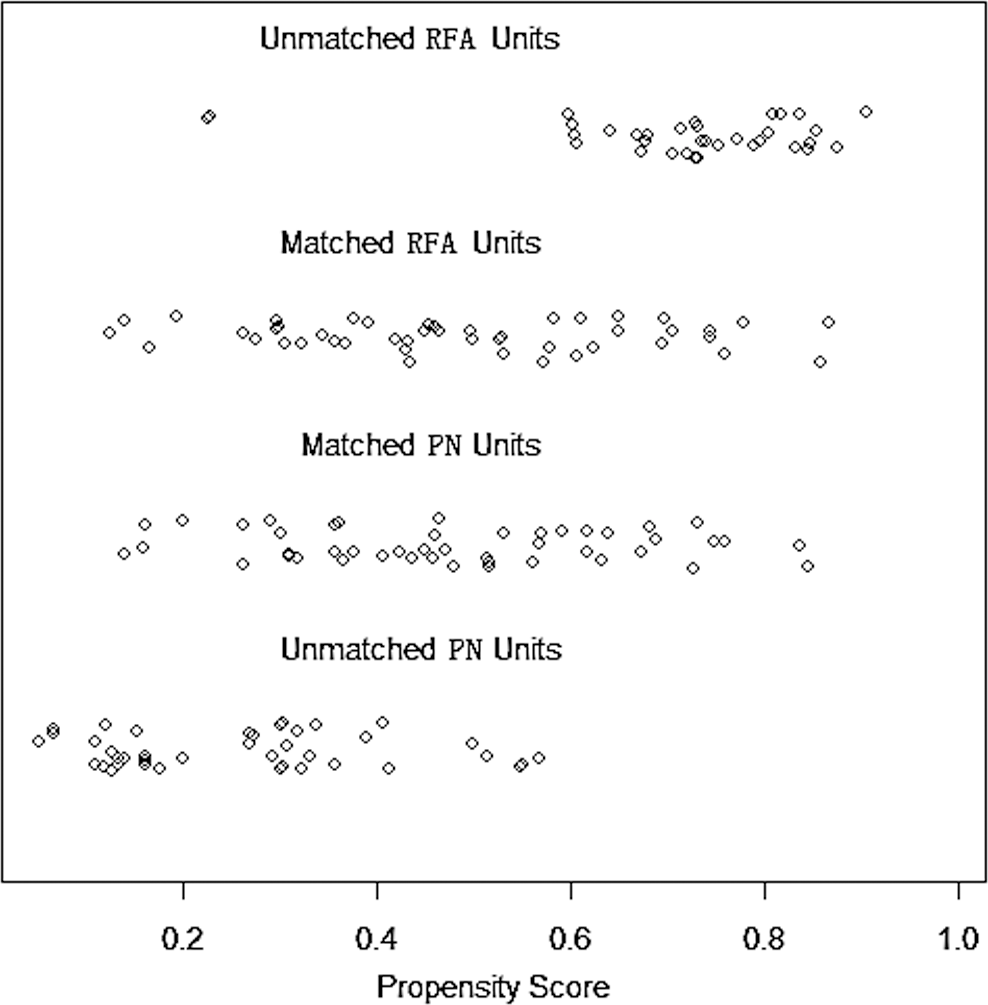
Distribution of propensity scores. RFA=radiofrequency ablation; PN=partial nephrectomy.

Flowchart of included study population. RCC=renal-cell carcinoma; PS=propensity score.
Regarding the renal functional outcomes, there was no significant difference in preoperative GFR or late GFR between the two groups (P=0.341, 0.057, respectively); however, the mean percentage change in GFR was −12.0±25.8 and −26.9±17.6 with a significant difference (P=0.001) for the RFA and PN groups, respectively. There was no new-onset chronic kidney disease or progression to dialysis postoperatively in both cohorts. No significant differences concerning hospital stay (P=0.311) and major complications (P=0.557) were found between the RFA and PN groups.
The mean follow-up period for RFA vs PN was 67.6 months±6.0 (median: 66 months) vs 69.0 months±12.9 (median: 72 months) in the matched cohort. No significant difference was found in the oncologic outcomes between the two study cohorts. The 5-year OS (95% CI) (Fig. 3a) was 90.2% (78.6–98.8) vs 93.2% (85.8–98.9) and 5-year CSS (95% CI) (Fig. 3b) was 95.6% (89.5–98.1) vs 97.7% (93.4–99.3) for RFA vs PN, respectively.

During the follow-up, three patients died in the RFA cohort. One of them was found to have disease progression (lung metastasis) 24 months after initial RFA and died 3 months later after refusing any therapy. The other two patients died of old age and colon cancer, respectively. Among the three patients in the PN cohort who died, one had multiple metastases and died 7 months later in spite of the administration of sorafenib. The other two died of either acute coronary syndrome or stroke.
Two patients in the RFA group and one patient in the PN group had local recurrence, which contributed to 5-year RFS (95% CI) (Fig. 3d) of 95.4% (89.3–98.1) vs 97.7% (93.3–99.2) for RFA and PN. The patient in the PN group who underwent open radical nephrectomy is alive without any disease at last follow-up. Both patients in the RFA group who underwent salvage laparoscopic radical nephrectomy after refusing salvage RFA remain without evidence of recurrence after the salvage surgery. All the local recurrence was confirmed by pathologic outcomes.
The 5-year MFS (95% CI) (Fig. 3e) was 95.5% (89.4–98.0) vs 95.5% (89.4–98.0) for the RFA and PN groups. Two cases of distant metastasis occurred in both groups, and one patient in each group died for the reasons mentioned above. The other two patients who had small lesions of liver metastases received salvage RFA, and the diseases remain stable during regular examinations.
Fig. 3c shows that the respective 5-year DFS (95% CI) for RFA vs PN was 86.7% (89.5–96.7) and 88.5% (79.1–97.9). Univariable and multivariate regression analyses demonstrated that sex, tumor size, surgical approach (RFA vs PN), and nephrometry score could not predict the DFS in propensity-score matched cohort significantly (Table 3). Age seemed to be the only factor that could predict the DFS in both univariable and multivariate regression analyses (P=0.032 and 0.044).
OR=odds ratio; CI=confidence interval.
Discussion
Surgical excision remains the gold standard for the treatment of patients with clinical T1a RCC. More and more articles in the recent literature reported that long-term oncologic outcomes for RFA mirror those for extirpative surgery. 12 Retrospective studies show that RFA is an effective minimally invasive therapy for the management of cT1a RCC, yielding comparable long-term oncologic outcomes to those of nephron-sparing surgery. 6 In the present study, we compared RFA with PN in cT1a RCCs regarding perioperative and oncologic outcomes based on a propensity-score matched analysis.
We compared 5-year DFS, CSS, RFS, MFS, and OS among patients treated with PN or RFA for sporadic and localized solid renal masses. We observed that local control was similar between the two treatment modalities. No significant differences were found of the five survival parameters between the two matched cohorts.
In a recent long-term series, Psutka and associates 10 reported that 5-year RFS, 5-year MFS, 5-year CSS, 5-year DFS, and 5-year OS for RFA in the treatment of T1a RCC was 96.1%, 100%, 100%, 91.5%, and 74%, respectively. Another more recent study from the Surveillance, Epidemiology and End Results-Medicare database reported their findings of 5-year OS and CSS for patients undergoing PN was 83.1% and 96.7%. 13
Direct comparison RFA with PN for patients with T1a RCC in terms of long-term oncologic outcomes is limited. Olweny and colleagues 6 reported their comparative 5-year oncologic outcomes for RFA vs PN in patients with clinical T1a RCC. They concluded that the respective 5-year OS was 97.2% vs 100% (P=0.31), CSS was 97.2% vs 100% (P=0.31), DFS was 89.2% vs 89.2% (P=0.78), local RFS was 91.7% vs 94.6% (P=0.96), and MFS was 97.2% vs 91.8% (P=0.35). Our long-term outcomes are favorable and comparable to the results of existing reports in the literature. Propensity-score matched analysis confirmed that there was no significant difference in the survival rates between RFA and PN cohorts.
Increasing numbers of studies have shown that renal function can be better preserved in patients undergoing RFA than in those undergoing PN with small renal masses. 6,14 Recent data indicate that short- and long-term influence on renal function may result from each minute of hilum clamping. 15 Several novel techniques have been introduced to minimize ischemic injury during PN 16 ; however, difficulties in mastering these special techniques and a longer learning curve limit their wide use in the clinical practice.
Our present study shows that RFA is a safe and easy way to better preserve renal function. At the same time, less estimated blood loss and shorter operative time are also favorable in the RFA cohort. In our series, intraoperative CEUS was used to monitor the damage, 17 and the treatment success rate was 100% after initial RF session. The perioperative major complication rate was comparable between the two cohorts of our present study. With the help of effective monitoring techniques, the RFA-related complications can remain at a relatively low level and RFA efficacy can be maximized. 18
Multivariate regression analyses in our matched cohort showed that age was the only factor that could predict the DFS in the long run. Patel and coworkers 13 found that a greater proportion of persons aged 75 years or older compared with those younger than 75 years died of kidney cancer (13.2% vs 4.6%, P<0.01). Older patients might also have tumors of a more aggressive biology because relative immunodeficiency associated with aging facilitates progressive growth of kidney cancer. 19 Thus, the excellent 5-year survival outcomes suggest that RFA may be selectively extended to younger and healthier patients who desire minimally invasive therapy.
This study is limited by the small sample size. A larger sample study is needed to confirm the outcomes of our study in the future. In addition, a retrospective design existed in our study, even though it had been matched by the propensity score. A randomized controlled trial could be ideal and may be realized in the future. Last, despite relatively homogeneous patient cohorts, multiple approaches for RFA and PN were included in our analysis, which could potentially introduce variation in treatment efficacy.
Despite these limitations, our results from propensity-score matched analysis are in favor of the clinical usefulness of RFA in carefully selected patients with T1a RCC. Given its relatively minimal invasiveness and excellent preservation of renal function, it is safe to believe that RFA will have a better application in the treatment of patients with small renal tumors. A further prospective randomized study is needed regarding the optimal management of patients with small renal masses.
Conclusion
RFA is an effective treatment option in appropriately selected patients with clinical T1a RCC, yielding comparable 5-year oncologic outcomes to PN and better preservation of renal function than PN.
Footnotes
Disclosure Statement
No competing financial interests exist.