
Abstract
Purpose:
To compare perioperative outcomes of open (OSP) and minimally invasive (MISP) simple prostatectomy for benign prostatic hyperplasia (BPH) in a large national cohort using validated patient safety measures.
Patients and Methods:
We studied patients undergoing simple prostatectomy for BPH in the Nationwide Inpatient Sample (NIS) from 1998 to 2010 and used weighted sampling to estimate national trends. Patient safety indicators (PSI) and multivariable regression were used to generate adjusted odds ratios (ORadj) comparing OSP with MISP.
Results:
We identified 34,418 and 193 patients undergoing OSP and MISP, respectively. Although the overall frequency of simple prostatectomy cases decreased from 3157 cases in 1998 to 2227 cases in 2010, the annual frequency increased each year from 2008 to 2010. We focused on 2008 to 2010 for the comparative outcome analyses. Among all OSP cases during this period (n=6027), the transfusion prevalence was 21%. MISP patients were more likely to have higher Charlson comorbidity scores (P=0.11) and less likely to undergo transfusion (P=0.13), but these differences did not attain significance. There were no significant differences in median length of stay (LOS) (P=0.19), hospital charges (P=0.15), or unadjusted in-hospital mortality (P=0.73). PSI frequency was low, and did not differ significantly between groups (ORadj 1.59, 95% confidence interval 0.26 to 9.53, P=0.61).
Conclusions:
In this, the first national analysis of simple prostatectomy, use of both OSP and MISP rose substantially from 2008 to 2010. Although transfusion prevalence was lower and LOS shorter for MISP, these differences did not attain significance. Further comparative analyses are needed.
Introduction
T
An increased incidence of clinically advanced BPH portends increases in the number of patients needing surgical therapy. Simple prostatectomy is a robust treatment for appropriately selected men with clinically advanced BPH and large prostates (
Patients and Methods
NIS
The NIS is the largest publicly available all-payer inpatient care database in the United States. It contains data from 5 to 8 million hospital stays per year and consists of all discharges from a stratified random 20% sample of community hospitals (
Prostatectomy case identification
We identified all discharges from January 1998 to December 2010 using principal or secondary procedure International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9CM) codes for suprapubic prostatectomy or transvesical prostatectomy (60.3) and retropubic prostatectomy (60.5). We excluded patients with an admission type other than elective, a diagnosis of prostate cancer, and with procedure codes for local excision of lesion of prostate (60.61) and radical prostatectomy (60.5). We then divided the remaining cases into “laparoscopic” (concurrent ICD-9CM codes 54.51, 54.21, or 17.42) or “open” (without concurrent laparoscopy codes). Because of the low number of MISPs performed before 2008, we focused on 2008 to 2010 for the comparative outcomes analyses.
Outcome variables
Outcome variables included hospital LOS, hospital charges, transfusion prevalence, and in-hospital mortality.
Patient safety indicators
The Agency for Healthcare Research and Quality (AHRQ) has developed a set of outcomes measures called patient safety indicators (PSIs) that provide information on preventable in-hospital adverse events identified in administrative data (
Statistical analysis
All estimates were weighted using the discharge level sampling weights to provide nationally representative estimates. Variance estimates and P values were computed using Stata v 11.1 (StataCorp, College Station, TX). 20 Statistical significance was assessed at the two-sided 5% level. We computed weighted estimates of the total number of OSPs and MISPs occurring in the United States in each year. Differences in proportion were assessed using chi-square tests (Rao & Scott second order correction).
We used weighted logistic regression to compare the incidence of any PSI between surgery types (OSP vs MISP). Variables were retained at 20% significance level or if deemed to be clinically significant. The final models included age, Charlson Comorbidity Index, 26 number of eligible PSIs, and year.
Results
Frequency of simple prostatectomy
We identified a total of 34,418 and 193 patients undergoing OSP and MISP, respectively. Although the overall frequency of simple prostatectomy procedures decreased from 3157 cases in 1998 to 2227 cases in 2010, the annual frequency increased each year from 2008 to 2010—the longest sustained, year-to-year increase during the study period (Fig. 1). The majority of MISP cases (n=182) occurred from 2008 to 2010.
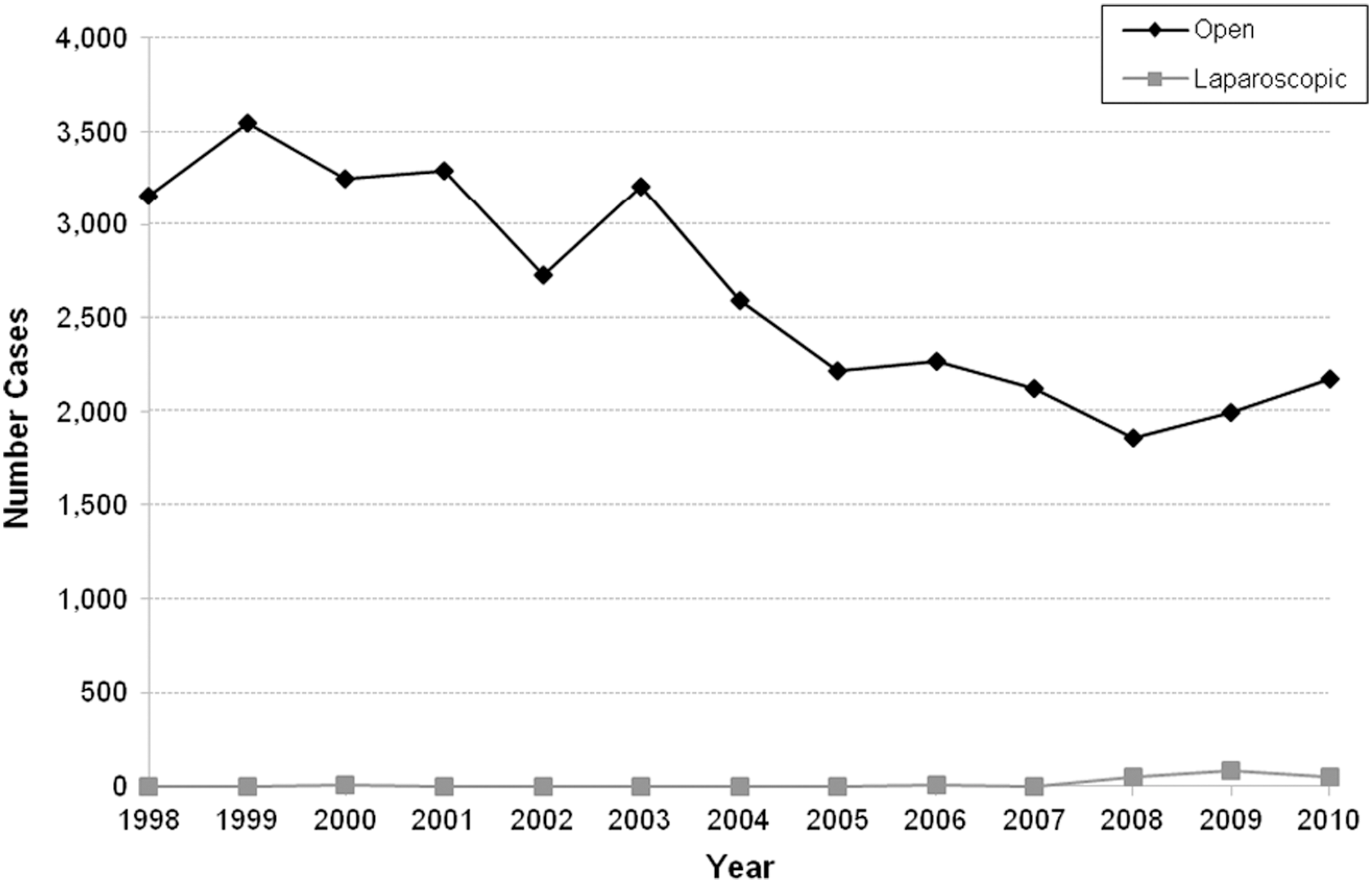
National estimated frequencies of open simple prostatectomy and minimally invasive simple prostatectomy by year, estimated from a 20% sample of the Nationwide Inpatient Sample with applied weighting with 95% confidence intervals provided for estimate.
Demographic characteristics
MISP patients were more likely to have higher Charlson Comorbidity scores, but this difference did not attain significance. There were no significant differences in age, race, income zip code, insurance status, or hospital type (Table 1).
National estimates for demographic characteristics, hospital length of stay, hospital charges, and unadjusted mortality prevalence associated with patients undergoing simple prostatectomy for localized prostate cancer in the Nationwide Inpatient Sample, 2008 to 2010.
The Agency for Healthcare Research and Quality prohibits the reporting of values ≤0.10 to protect patient privacy.
SD=standard deviation; IQR=interquartile range.
Perioperative outcomes: Transfusion, LOS, hospital charges, and mortality
MISP patients were 50% less likely to undergo transfusion and had a shorter median LOS, but these differences did not attain significance (Table 1). Multivariable regression analysis comparing the risk of transfusion for MISP to OSP confirmed a 53% decreased risk for MISP that did not attain significance (adjusted odds ratio [ORadj] 0.47, 95% confidence interval [CI] 0.18 to 1.26, P=0.13). There were no significant differences in hospital charges or unadjusted in-hospital mortality (Table 1).
PSI
Overall PSI frequency was low, occurring among <5% of OSP and MISP patients combined and did not differ significantly between groups (Table 2). On multivariate analysis, there was no significant difference in the adjusted probability of any PSI between groups (ORadj 1.59, 95% CI 0.26 to 9.53, P=0.61).
National estimates for frequency of patient safety indicators for patients undergoing simple prostatectomy in the Nationwide Inpatient Sample, 2008 to 2010.
All patients were ineligible to experience the PSI.
The Agency for Healthcare Research and Quality prohibits the reporting of values ≤0.10 to protect patient privacy.
OSP=open simple prostatectomy; MISP=minimally invasive simple prostatectomy; PSI=patient safety indicator; DRG=diagnosis related group; PE=pulmonary embolism; DVT=deep venous thrombosis.
Discussion
This study is the first comparative analysis of perioperative outcomes for simple prostatectomy. In summary, these data demonstrate that the national frequencies of both OSP and MISP rose substantially from 2008 to 2010, suggesting an increased use of simple prostatectomy in the United States during this period. Although the prevalence of perioperative transfusion for MISP was 50% lower than that of OSP (10.8% vs 20.9%, P=0.13), and the median LOS 2 days less (2 days vs 4 days, P=0.19), these differences did not attain significance in this analysis. PSI frequency was low and did not differ significantly between groups, indicating a low probability of preventable adverse patient safety events occurring with either surgical approach. The steady decline in national utilization of simple prostatectomy from 1999 to 2008 paralleled decreases in both the use of transurethral prostate surgery 27 and the incidence of complications secondary to clinically advanced BPH during the same period. 7 The increased use of simple prostatectomy after 2008, however, corresponded to increased use of transurethral laser surgery (with steady use of transurethral resection of the prostate) in Canada, 28 as well as increased complications from clinically advanced BPH—namely, urinary retention and renal failure—in the United States. 7 These observations support the hypothesis that the population incidence of advanced BPH necessitating minimally invasive surgery or simple prostatectomy is growing. Further investigations into these population patterns are warranted.
Previous single institution series of OSP have observed substantial perioperative morbidity, including relatively high intraoperative blood loss and rates of transfusion. 11,13 –15 Our data confirm that a high proportion—at least one in five—of patients undergoing OSP receive perioperative transfusions. Since the first descriptions of laparoscopic 29 and robot-assisted laparoscopic simple prostatectomy 30 in 2002 and 2008, respectively, several noncomparative single institution series have noted that MISP substantially decreases the risk of transfusion, with the majority of robotic series observing a transfusion prevalence of 0%. 16 While the decreased transfusion risk for MISP in our analysis did not attain significance, even after adjustment for age and morbidity, it is possible that our study was underpowered in this regard, raising the potential for Type II error. Only 182 MISP surgeries were available nationally for analysis from 2008 to 2010. Another possible explanation, which may at least in part account for the 10-fold increased transfusion prevalence observed nationally compared with individual institutions, is progression of MISP surgical teams through an initial learning curve before achieving lower amounts of intraoperative blood loss and rates of transfusion. Additional comparative analyses incorporating larger numbers of MISP surgical procedures over a longer period would potentially clarify these associations.
Our data also demonstrate that both OSP and MISP are reasonably safe procedures with a relatively low incidence of preventable adverse safety events. PSIs are quality measures designed by the AHRQ to identify flaws in the processes of care. They include complications of anesthesia, postoperative respiratory failure, and pulmonary embolus. Both the Institute of Medicine (IOM) and the AHRQ have identified preventable medical injuries as a source of substantial morbidity and increased health care costs. The IOM has challenged healthcare providers to implement safer processes to protect patients against preventable complications. 21,24,25,31
Despite the overall low frequency of PSIs for simple prostatectomy, there remains room for improvement. PSIs are preventable injuries. Measurement and identification of PSIs thus informs clinical care aimed at improving patient safety.
32,33
The most common preventable event for OSP, occurring in nearly 10% of cases, was failure to rescue (AHRQ prohibits the publication of values ≤10 to insure patient privacy, but the proportion of failure to rescue events for MISP did not differ significantly from OSP). Failure to rescue is defined as failure to prevent a clinically important deterioration, such as death or permanent disability, from a complication of an underlying illness (e.g., cardiac arrest in a patient with acute myocardial infarction) or a complication of medical care (e.g., major hemorrhage after elective surgery). Failure to rescue thus provides a measure of the degree to which providers respond to adverse occurrences during hospitalization. It may reflect the quality of monitoring, the effectiveness of actions taken once complications are recognized, or both (
A strength of this study is its use of validated quality assurance measures computed from a large national cohort. One potential limitation is that variations in coding practices over the study period may have influenced the analyses. There is no evidence, however, that such variations would have differentially biased the outcomes. A second potential limitation is that we could only assess outcomes during hospitalization after surgery. It is possible that adverse events occurring after discharge, but still within the 30-day perioperative period, were not assessed. A third limitation is that, because of the relatively small number of MISP surgeries performed, we were unable to distinguish laparoscopic from robot-assisted laparoscopic procedures in the analyses. Finally, we were unable to assess procedure-specific outcomes such as urinary continence, potency, adenoma weight, International Prostate Symptom Score, and postoperative urinary flow.
Conclusions
In this, the first national comparative analysis of simple prostatectomy, use of both OSP and MISP rose substantially from 2008 to 2010. The transfusion prevalence for OSP was 21%. Although transfusion prevalence was lower and LOS shorter for MISP, these differences did not attain significance. Further comparative analyses are needed.
Footnotes
Disclosure Statement
Dr. Parsons is a speaker for American Medical Systems and an investigator for Actavis (Watson Pharmaceuticals). For the remaining authors, no competing financial interests exist.