
Abstract
Background and Purpose:
The refinement in the localization of prostate cancer tumor foci through transperineal template-mapping biopsies and MRI has led to an increased interest in lesion-directed focal prostatic cryoablation. Data are lacking, however, that compare the outcomes of whole-gland (WG) to focal ablation therapy (FT). The aim of our study was to assess both oncologic and functional outcomes between WG and FT cryoablation of the prostate after having matched patients for preoperative characteristics.
Patients and Methods:
We matched with a 1:1 ratio 317 men who underwent FT with 317 who underwent WG treatment in the Cryo Online Data (COLD) registry between 2007 and 2013. All patients were low-risk according to the D'Amico risk groups and were matched according to age at surgery. We only included preoperatively potent men. Oncologic outcomes were biochemical recurrence (BCR) free-survival defined according to the American Society for Radiation Oncology (ASTRO) and Phoenix criteria and assessed by Kaplan-Meier curves. Only patients with prostate-specific antigen (PSA) nadir data were included in oncologic outcome analysis. Functional outcomes were assessed at 6, 12, and 24 months after the procedure for erectile function (defined as ability to have intercourse with or without erectile aids), urinary continence, urinary retention, and rates of fistula formation.
Results:
Median age at the time of the procedure was 66.5 years (standard deviation [SD] 6.6 y), and median follow-up time was 58.3 months. After surgery, 30% (n=95) and 17% (n=55) of the men who received WG and FT, respectively, underwent biopsy, with positive biopsy rates of 11.6% and 14.5%, respectively. BCR-free survival rates at 60 months according to the Phoenix definition were 80.1% and 71.3% in the WG and FT cohorts, respectively, with a hazard ratio of 0.827; according to the ASTRO definition, they were 82.1% and 73%, respectively (all P≥0.1). Erectile function data at 24 months was available for 172 WG and 160 FT treated men. Recovery of erection was achieved in 46.8% and 68.8% of patients in the WG and FT cohorts, respectively (P=0.001). Urinary function data at 24 months was available for 307 WG and 313 FT patients. Continence rates were 98.7% and 100% for WG and FT groups, respectively (P=0.02). Urinary retention at 6, 12, and 24 months was reported in 7.3%, 1.9%, and 0.6%, respectively, in the WG arm, and in 5%, 1.3%, and 0.9%, respectively, in the FT arm. Finally, only one fistula was reported in each group.
Conclusions:
Men with low-risk prostate cancer who underwent FT cryoablation had comparable BCR-survival rates at 60 months to patients treated with WG. However, FT patients had higher erectile function preservation rates at 24 months post-procedure. Urinary continence, retention and fistula rates were similar between the two treatment groups.
Introduction
P
Active surveillance (AS) was developed with the intent of postponing or in some cases completing avoiding therapy and treatment-related complications in patients with low-risk disease. Simultaneously, AS aims to maintain rigorous surveillance of the cancer by serial biopsies to preserve quality of life as long as possible. Despite excellent outcomes and quality of life, 8 this strategy remains underutilized, both because of patient anxiety factors 9 –11 and for fear of sampling errors (undergrading/understaging) associated with conventional prostate biopsies 12,13 that might misguide risk stratification and treatment planning.
In this context, prostate cryoablation was developed as a minimally invasive method to control disease. At 5 years after whole-gland (WG) cryoablation, 75% to 90% of low-risk men are expected to be free from biochemical recurrence (BCR). 14 –16 While WG cryoablation offers excellent preservation of urinary continence, only 25% to 30% of men have been historically able to have sexual intercourse, 14,17 likely because of thermal damage to the neurovascular bundles.
Focal cryoablation therapy (FT), in contrast, by targeting just the index lesion or cancerous region of the prostate, is aimed at maintaining erectile function by preserving at least one of the nerves erigendi. The largest study to date reported erections in almost 60% of patients after focal treatment intended as nonimage-guided partial ablation of the prostate. 17
There is a lack of systematic comparison of oncologic and functional outcomes between WG and FT series. Hence, the aim of our study was to compare oncologic and functional outcomes between WG and FT in preoperatively potent men with D'Amico low-risk disease, after having matched them for age, a well-known predictor of erectile dysfunction and urinary incontinence.
Patients and Methods
Patient population and treatment modality
From the Cryo Online Data (COLD) registry, we extracted data on men who underwent primary prostate cryoablation between 1999 and 2013 for histologically diagnosed prostate cancer. The COLD registry is a web-based database aimed at collecting data on patients treated with prostate cryoablation. Clinicians enter data, and the database is maintained and audited by Watermark Research Partner, Inc. (Watermark, Indianapolis, IN), an independent research company.
A separate physician board supervises the database and is responsible for all research queries and publications. The registry is funded by Endo Pharmaceuticals, a manufacturer of cryoablation equipment. The database is approved by a central Institutional Review Board and by the Institutional Review Boards of local participating institutions.
We queried data on 7403 patients who underwent primary cryoablation between 2007 and 2013. Treatment data in the COLD registry are classified either as “whole-gland” or “partial-gland.” There are no guidelines produced from the advisory board of the registry on either patient selection or ablation template. Therefore, data from the COLD registry represent treatment as practiced in the community and prevailing selection criteria at the time of enrollment, as well as heterogeneity of focal-therapy approaches (i.e., hemi-ablation, ablation of a quarter of the prostate, or index lesion ablation).
We excluded patients who underwent WG ablation using a “nerve-warming” technique whereby a probe was placed adjacent to the nerve(s) to try to maintain a warm temperature during the cryoablation process. Of the whole population, we selected 785 men who met low-risk criteria according to the D'Amico 18 definition—that is, biopsy Gleason score ≤6, PSA level at diagnosis <10 ng/mL, and clinical stage ≤T2a. Furthermore, we included only men with preoperative erectile function sufficient for penetration during sexual intercourse. It is indeterminate if this definition was patient or provider-reported given the limitations of the database.
Lastly, because age has an important impact on both urinary and erectile function, 19,20 we performed a 1:1 match based on age at time of surgery between patients undergoing WG and FT. The final study cohort consisted of 634 men, 317 of whom underwent WG treatment and 317 of whom underwent FT.
Outcomes and statistical analysis
The oncologic outcome of our study was biochemical recurrence (BCR), defined according to both the American Society for Radiation Oncology (ASTRO) (three consecutive rises in PSA level >6 months after therapy) 21 and the Phoenix definitions (PSA nadir +2 ng/mL) 22 and positive biopsy rate (biopsy of treated area). Functional outcomes were: Erectile function, defined as the ability to have penetration during sexual intercourse, with or without erectile aids; urinary continence (no pad use); urinary retention; and the development of a rectourethral fistula. Functional outcomes in the COLD registry are commonly recorded at 6, 12, and 24 months after the procedure as categorical variables. Additional data are not routinely collected after the 24 months because potency and continence have often stabilized by this point. Post-treatment biopsies were performed for cause—because of a rising PSA level meeting BCR definitions.
Kaplan-Meier curves were used to assess BCR-free survival rates in the two groups, and the log-rank test was used to compare them. Comparison between the functional outcomes at 6, 12, and 24 months after the procedure was assessed with the Fisher exact test. All statistical tests were two-sided, and significance was set as a P value <0.05. Statistical analysis was conducted using commercial statistical software (MedCalc, Mariakerke, Belgium).
Results
Median age at surgery was 66.5 years. All patients selected were low risk according to the D'Amico definition, having a serum PSA level at diagnosis ≤10 ng/mL, biopsy Gleason ≤6, and clinical stage ≤T2a (see Table 1 for full demographic details). Figures 1a and 1b show Kaplan-Meier curves predicting BCR-free survival according to ASTRO and Phoenix criteria, respectively. Median follow-up time was 58.3 months.
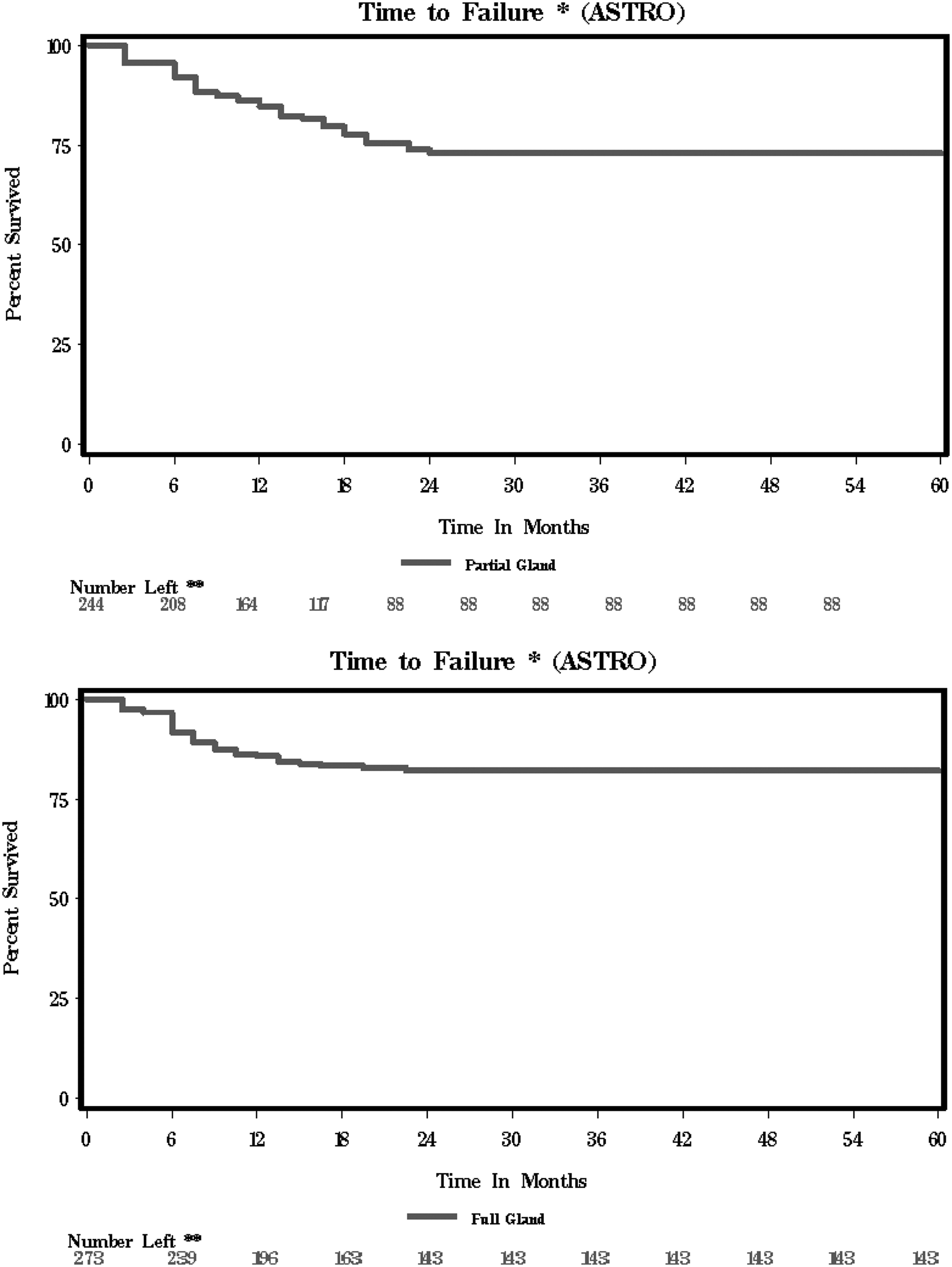
Time to failure, whole gland and partial gland (American Society for Radiation Oncology [ASTRO] definition). Percent surviving are calculated from Kaplan-Meier product limit estimates. Deaths are censored at the last recorded visit.
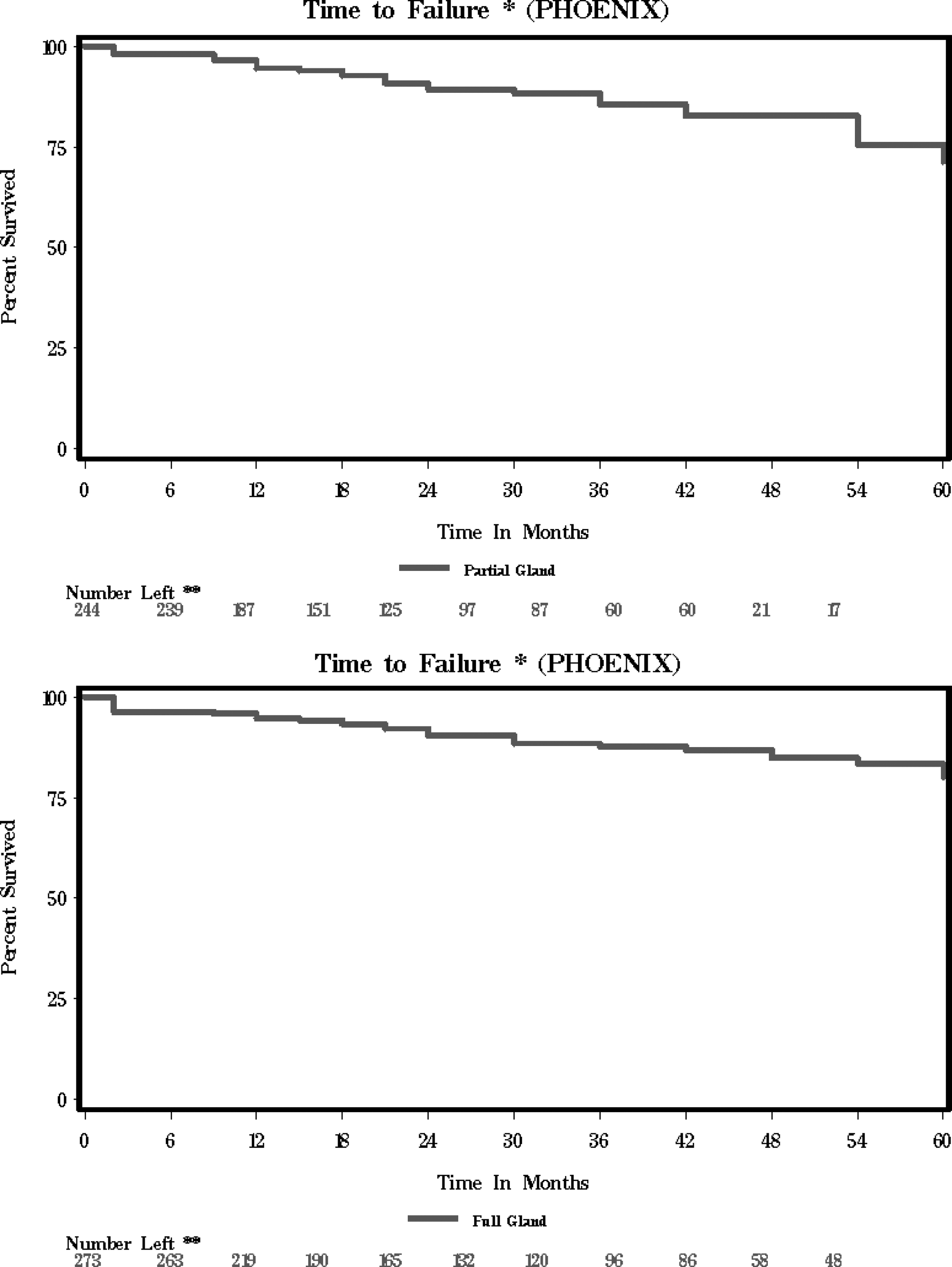
Time to failure, whole gland and partial gland (Phoenix definition). Percent surviving is calculated from Kaplan-Meier product limit estimates. Deaths are censored at the last recorded visit.
All percentages are based on the number of subjects identified by (n=) at the top of the column.
All patients low risk: PSA <10, Gleason <7, and Stage <T2b.
Std. Dev.=standard deviation; PSA=prostate-specific antigen.
Using the ASTRO definition, 60 months after ablation, BCR-free survival rates were 82.1% and 73% for the WG and FT groups, respectively (P=0.1). On the other hand, according to the Phoenix definition, BCR-free survival rates 60 months after ablation were 80.1% for men who received WG therapy and 71.3% for those who received FT (P=0.5) with a hazard ratio of 0.827.
After ablation, prostate biopsy was performed for cause with an increase in PSA level in 95 (30%) of men who received WG treatment with 11 (11.6%) positive results, while it was conducted in 55 (17%) patients treated with FT, with 8 (14.5%) having positive results.
Urinary continence data for all time intervals were available for 307 (97%) patients who were treated with WG ablation and 313 (99%) who were treated with focal ablation. Rates of urinary continence recovery at 6, 12, and 24 months were 98%, 98%, and 98.7%, respectively, in the WG arm, and 99.4%, 100%, and 100%, respectively, in the focal arm (P=0.02).
Erectile function data were available at 6, 12, and 24 months for 225 (71%), 217 (68%), and 172 (54%) men, respectively, in the WG group, and for 172 (54%), 200 (63%), and 160 (50%) men, respectively, in the FT group. Among patients who received WG cryoablation, 29.3%, 41%, and 46.8% reported to be able to have intercourse at 6, 12, and 24 months after treatment, respectively, while among patients who received focal cryoablation, 54.1%, 59.5%, and 68.8%, reported to have a satisfactory erection at 6, 12, and 24 months, respectively (P=0.001).
Urinary retention was reported at 6, 12, and 24 months in 7.3%, 1.9%, and 0.6%, respectively, in the WG arm, and in 5%, 1.3%, and 0.9%, respectively, in the focal arm. Finally, only one episode of rectourethral fistula was reported in each treatment group.
Discussion
The foremost goal of cancer therapy should be to control disease by preventing progression and recurrence. For this reason, before FT is widely implemented, it should have a similar efficacy to radical treatment. In the context of a lack of prospective randomized data, our study demonstrated equivalent BCR-free survival rates at 5 years between WG cryoablation and FT among men with preoperative low-risk disease. Indeed, we report BCR-free rates in the range of 70% to 80%, similar to contemporary data in the literature. 17,23
It may be argued that radical prostatectomy in low-risk patients warrants higher BCR-free survival rates, in the range of 80% to 90% at 5 years after surgery. 24,25 Several aspects need to be considered, however. First, comparing BCR rates between radical surgery and cryoablation can be troublesome. Indeed, radical prostatectomy aims at removing all prostatic tissue; therefore, any increase in PSA level is from persistent prostatic tissue/cancer in situ or to distant spread of tumor cells.
In the case of cryoablation, healthy prostatic cells might still be viable after the procedure and therefore still produce low levels of PSA, particularly around the urethra that is purposely preserved with a urethral warming catheter. For this reason, cryotherapists have adopted BCR definitions from radiotherapy studies, such as the ASTRO and Phoenix ones.
Despite being developed for another form of treatment, the Phoenix definition has been shown to be the most sensitive and specific definition to identify men with an increase in PSA level and actual disease recurrence at biopsy after cryoablation. 26 The area under the curve of the Phoenix criteria, however, is only 0.64, suggesting that the best way to determine the efficacy of cryoablation would be with mortality data. Comparison of mortality data could be challenging, because many cryoablation patients are older and suffer from more comorbidities compared with men who undergo radical surgery. 27
Second, level 1 evidence seems to suggest that in men with low-risk features, radical therapy might do more harm than good, causing functional sequelae without improving long-term survival, especially in older men. 5,6 Therefore, radical therapy is being considered an overtreatment with quality-of-life altering consequences, such as erectile dysfunction and urinary incontinence, especially in men who most likely will die of other causes rather than of prostate cancer.
Having demonstrated that focal and WG cryoablation perform equally in terms of cancer control at the 5-year mark, we then tested whether partial prostate ablation assures better erectile function recovery. In our series of preoperatively potent patients, 68.8% of men treated with FT recovered erectile function sufficient for intercourse with or without erectile aids 2 years after the procedure, compared with 46.8% of men who were treated with WG ablation (P=0.001). In addition, urinary continence was recovered in all patients by 1 year after treatment, despite ablation template.
Potency recovery rates for FT patients in the literature range from 58% to 86%, with or without the need of proerectile therapies, 16,17,23,28,29 comparable to our findings. We report higher than usual recovery rates for WG ablation, however, because previously published data report recovery of erections sufficient for intercourse in 5% to 47% of men. 14,30 –35 In addition, the potency rates at 2 years from FT in our study are also consistent with those reported for men undergoing minimal minimally invasive radical prostatectomy at 2 years (from 63% to 94%). 36
These optimistic results are most likely because of different factors. First, unlike FT series that recruit men who are interested in preservation of erections, WG studies usually attract an older population with comorbidities, including erectile dysfunction, who want to avoid radical surgery. 27 Potency recovery is indeed strongly related to preoperative erectile status, comorbidities, and age at surgery, 37 and hence erectile outcomes in previously published WG cryoablation studies might have been influenced by the poor overall health of the patients.
In one study by Kimura and colleagues, 35 77% of men undergoing primary WG cryotherapy presented with severe erectile dysfunction at the time of the procedure. In our study, we only included men who were capable of intercourse at the time of the procedure, rendering our series the largest one yet. A second bias might be that our functional data, because of the nature of the COLD registry, is reported in binary format—i.e., potent or not—and the source of this information is not identified in the registry.
Our study is not devoid of limitations. First, the majority of patients with low-risk disease would be offered AS today, and the study population would more likely focus on intermediate-risk disease instead. During this study, however, men with low-risk disease were believed to be candidates for FT, and even whole gland radical therapies; thus, the low-risk population reflects the prevailing attitude for treatment at the time.
The COLD registry includes data from a multitude of institutions, and from different levels of practices, therefore rendering it very heterogeneous. The differences are not only limited to the ablation template for FT, but also apply to patient selection criteria, follow-up protocols, and cryoablation technologies. The registry aims at prospectively collecting outcomes data and does not issue any centralized operative guidelines. The registry, apart from clinical stage, biopsy Gleason grade, and PSA level at diagnosis, does not have data on more specific selection criteria for FT versus WG, such as number and percentage of positive cores at biopsy or physician methodology for treatment selection.
The shortcomings regarding the oncologic outcomes are the midterm (5-year) follow-up and the lack of BCR definitions specific to cryoablation and FT. An alternative outcome could have been the presence of cancer at biopsy in the case of BCR. We only have postprocedure biopsy data, however, on a small proportion of patients because of biopsies being performed for cause. Also, because of the nature of the registry, we are not able to locate the time of the biopsy in relation to BCR.
An ideal study would assess cancer-specific mortality rates, but it would require a long follow-up. In addition, prostate cancer-specific mortality rates are very low in men with low-risk disease.
Another limitation is the lack of standardized functional outcome reports through validated questionnaires. There are no guidelines produced from the advisory board of the registry requiring the collection of validated questionnaires; therefore, this practice varies among individual urologists and is not a prerequisite to add functional data to the registry. Furthermore, functional data is inserted into the registry as a binary outcome (i.e., potent or not potent, or continent or incontinent); thus, it does not allow for more refined studies on variation of outcomes. Data on the use of proerectile aids after the procedure were too scarce to be reported, and data on comorbidities that could affect erectile function were missing.
These limitations need to be balanced by the strengths of the study, however. A 2-year observation period to determine outcomes of urinary and erectile function is usually sufficient time. A 100% self-reported urinary continence is excellent, particularly when using a very strict definition of “no pad” use. Although we do not know the exact template for FT used in each case, the vast majority of patients were treated with a hemi-ablation approach in which one of the neurovascular bundles on the side of the known cancer was intentionally ablated as part of the therapy. At the time of the study, hemi-ablation was the most common manner of applying focal therapy.
An overall potency rate of 69% in the FT arm is quite good given the intentional ablation of one of the nervi erigente. At present, FT has become much more targeted to the specific lesion, and the neurovascular bundle is not routinely and intentionally treated. Thus, with more focused treatments, we only expect the potency rate to improve.
Conclusions
Among potent men with low-risk prostate cancer, FT seems to deliver similar oncologic control in the midterm with improved erectile function recovery rates after the procedure. FT still remains a novel approach that needs long-term validation in prospective-randomized trials comparing it with the standard of care, such as radical prostatectomy. Furthermore, lately there has been a shift of indications for FT, with recruitment of men presenting with intermediate-risk criteria, such as PSA ≤15 ng/mL, clinical stage T2c, or biopsy Gleason 3+4. 16,38
The broadening of indications for FT has been brought about by improvement in cancer localization within the gland, with standardized three-dimensional–template mapping biopsy protocols 39 as well as the development of multiparametric MRI and MRI-transurethral ultrasonography fusion-guided biopsies. 40 In the future, FT could aim at ablating only index lesions while sparing as much healthy tissue and structures as possible, ensuring optimal preservation of quality of life.
Author Disclosure Statement
Dr. Polascik is a consultant, educator, and has investment interests in Endocare. For the remaining authors, no competing financial interests exist.
Footnotes
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.