
Abstract
Purpose:
To examine the association between statin medication use and sepsis risk after percutaneous nephrolithotomy (PCNL).
Materials and Methods:
Using medical claims data, we identified working-age adults with urinary stone disease who were treated with PCNL. Among this cohort, we determined which patients had a prescription fill for a statin agent that encompassed their surgery date. We then fitted logistic regression models to examine for differences in rates of postoperative sepsis between statin users and nonusers. In addition, we evaluated the frequency of nonfebrile urinary tract infections (UTIs) and intensive care unit (ICU) services utilization and hospital length of stay (LOS) as a function of statin use.
Results:
During the study period, at total of 2046 patients underwent PCNL, 382 (18.7%) of whom had a prescription fill for a statin agent preceding their surgery. The overall rate of sepsis in this population was 3.8%. After adjusting for patient health status and sociodemographic factors, the rate of postoperative sepsis was comparable between statin users and nonusers (5.3% vs 3.5%, respectively; P=0.105). In addition, UTI and ICU utilization rates did not relate to statin use (P>0.05 for all associations). Adjusted hospital LOS was shorter among statin users, but the difference was clinically trivial (3.6 vs 4.1 days; P=0.007).
Conclusions:
Statin use is not associated with reductions in postoperative sepsis, nonfebrile UTIs, ICU utilization, or hospital LOS after PCNL. To increase the safety of PCNL, urologists will have to consider other processes of care (e.g., clinical care pathways).
Introduction
W
Emerging data suggest that the benefits of statins extend beyond their lipid-lowering effects. Specifically, empiric work shows that these medications exhibit both anti-inflammatory and antioxidant properties, as well. 7 –9 Statins have been shown to blunt the first step in the activation of the cellular cascade of the immune system in reaction to microbial infection, thereby lowering levels of cytokines, tumor necrosis factor, and C-reactive protein—drivers of the sepsis response. 10,11 To the extent that these properties can be leveraged to modulate the systemic immune response, statin use may have a role in the prevention of postoperative sepsis. 12 Among different populations, statin use has been shown to be associated with lower rates of other types of infections, including respiratory, blood, and urinary infections. 13 –16 No study yet, however, has examined the infectious prophylaxis role of statin in patients undergoing PCNL.
To address this knowledge gap, we conducted an observational study using medical claims from working-age adults. After identifying patients with nephrolithiasis who were treated with PCNL, we determined those who were prescribed a statin medication preoperatively. We then estimated the risk of postoperative sepsis, comparing rates between statin users and nonusers. Findings from our analysis serve to inform urologists who manage urinary stone disease on the utility of statin prophylaxis among PCNL patients.
Materials and Methods
Data source
For our study, we used Truven Health's MarketScan® Commercial Claims and Encounters Database (2002–2006). This database captures the healthcare utilization of an estimated 5.6 million working-age adults and their dependents with employer-sponsored benefit plans. Contained within these data are all inpatient and outpatient claims submitted on a beneficiary's behalf, including detailed prescription drug information, which was important, given our interest in statin use.
Study population
Through a previously described algorithm, we used International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9) diagnosis codes to identify adults 18 to 64 years of age with one or more claims for urinary stone disease. 17,18 We then used relevant Current Procedural Terminology codes to identify the subset of patients who underwent PCNL at some point during the study interval. For study inclusion, we required that persons have continuous enrollment in a benefit plan for a minimum of 120 days before and 30 days after the index date for their surgical procedure. We excluded those enrolled in benefit plans from which Truven Health did not receive prescription drug claims in the 30 days before the procedure.
Exposure
We then used National Drug codes for 32 proprietary and generic statin medications to distinguish between patients prescribed statin therapy before PCNL and those who were not. 19 We tracked statin use based on prescription fill dates and the number of days supplied. A patient was considered a statin user if he or she had a prescription fill for a statin agent, where the days supplied encompassed the procedure date and the 2 weeks before it. We chose a 2-week period because the anti-inflammatory of statins have been observed within 2 weeks of treatment. 20 For our primary analysis, patients who stopped their statin more than 90 days before the surgical procedure were classified as nonusers. Patients who were taking statins at some point between 90 days and 14 days of the index date were excluded from the study cohort because of possible residual effects of statin therapy.
Outcomes
Our primary outcome of interest for this study was the occurrence of sepsis after PCNL. We defined sepsis events using an ICD-9 code-based algorithm. Within the 30-day period after the procedure date, we said that a sepsis event occurred if a patient had a claim filed on his behalf with one or more of the following ICD-9 codes: 020.0x (septicemic), 038.xx (septicemia and its subtypes), 785.52 (septic shock), 790.7x (bacteremia), 995.91 (sepsis), 995.92 (severe sepsis), and 780.6 (fever of unknown origin).
In addition to the occurrence of sepsis, we measured a variety of secondary outcomes, including the occurrence of a nonfebrile urinary tract infection (UTI), the use of intensive care unit (ICU) services postoperatively, and hospital length of stay (LOS). UTIs were identified in the 30-day period after the surgery date using a previously described ICD-9 code-based algorithm. 21 Hospital LOS was defined using patient admission and discharge status. ICU services use was determined through standard revenue codes from the facility claims filed within the 30-day surgical episode.
Statistical analysis
For our initial analytic step, we used t tests and chi-square tests, where appropriate, to compare statin users and nonusers across a variety of sociodemographic and clinical factors. Specifically, we made comparisons based on patient age, sex, surgery setting (inpatient vs outpatient), employee classification (salaried vs nonsalaried), employment status (full- vs part-time), benefit plan type (comprehensive, preferred provider organization, health maintenance organization, point-of-service, or other noncapitated plan), residence within a metropolitan statistical area, and geographic region of residence based on the United States Census regions (Northeast, Midwest, South, or West).
Because a patient's baseline health may contribute to his or her sepsis risk, we assessed comorbidity using a modification of the Charlson index. 22 In addition, we identified all the patients who had a medical claim filed for sepsis or a nonfebrile UTI within the 90-day window before the surgery date using the ICD-9 codes mentioned above. Further, we determined those patients who were prescribed antimicrobial therapy within 5 days of their procedure (but not including the day of the procedure, which reflects standard antibiotic prophylaxis).
After adjusting for the patient factors described above, we then used multiple logistic regression to evaluate the association between statin use and the occurrence of postoperative sepsis. We fitted similar models to assess the relationship between statin use and UTI and ICU utilization rates. Finally, we used multivariable Poisson regression to evaluate the relationship between hospital LOS and the use of statin therapy. We conducted all analyses using SAS® (version 9.3) statistical software. All tests were two-tailed with the probability of type I error at 0.05. Our Institutional Review Board deemed this study to be exempt from its oversight.
Results
In total, we identified 2046 patients who met our inclusion criteria. Among these patients, 382 (18.7%) were statin users. When compared with nonusers, patients on statin therapy were more likely to be older (P<0.001) and men (P<0.001) (Table 1). With regard to socioeconomic status, statin users were more likely to have full-time employment (P<0.001), be salaried (P=0.005), and have a more generous benefit plan (P<0.005). They were also more likely to reside in the Midwest and Northeast (P<0.005). Perhaps more important, a greater proportion of statin users had higher levels of comorbid illness and preoperative sepsis and UTI than nonusers (P<0.001).
SD=standard deviation; PPO=preferred provider organization; HMO=health maintenance organization; POS=point of service; UTI=urinary tract infection.
Postoperative sepsis was uncommon in our cohort, occurring in only 78 (3.8%) of patients. In 10% of these patients, sepsis was severe enough to warrant ICU admission, but no deaths occurred in our cohort. More than 40% of sepsis events occurred in the first 3 days after PCNL (Fig. 1). Only 13% of patients with sepsis had a drainage tube (either a ureteral stent or nephrostomy tube) inserted before the procedure. Patient factors that were independently associated with the odds of sepsis included the level of comorbid illness and whether or not the procedure was performed on an outpatient or inpatient basis (Table 2). On multivariable analysis, the occurrence of an uncomplicated UTI or sepsis before surgery increased the odds of postoperative sepsis by 71% (odds ratio [OR], 1.71; 95% confidence interval [CI], 1.06 to 2.76; P=0.028).
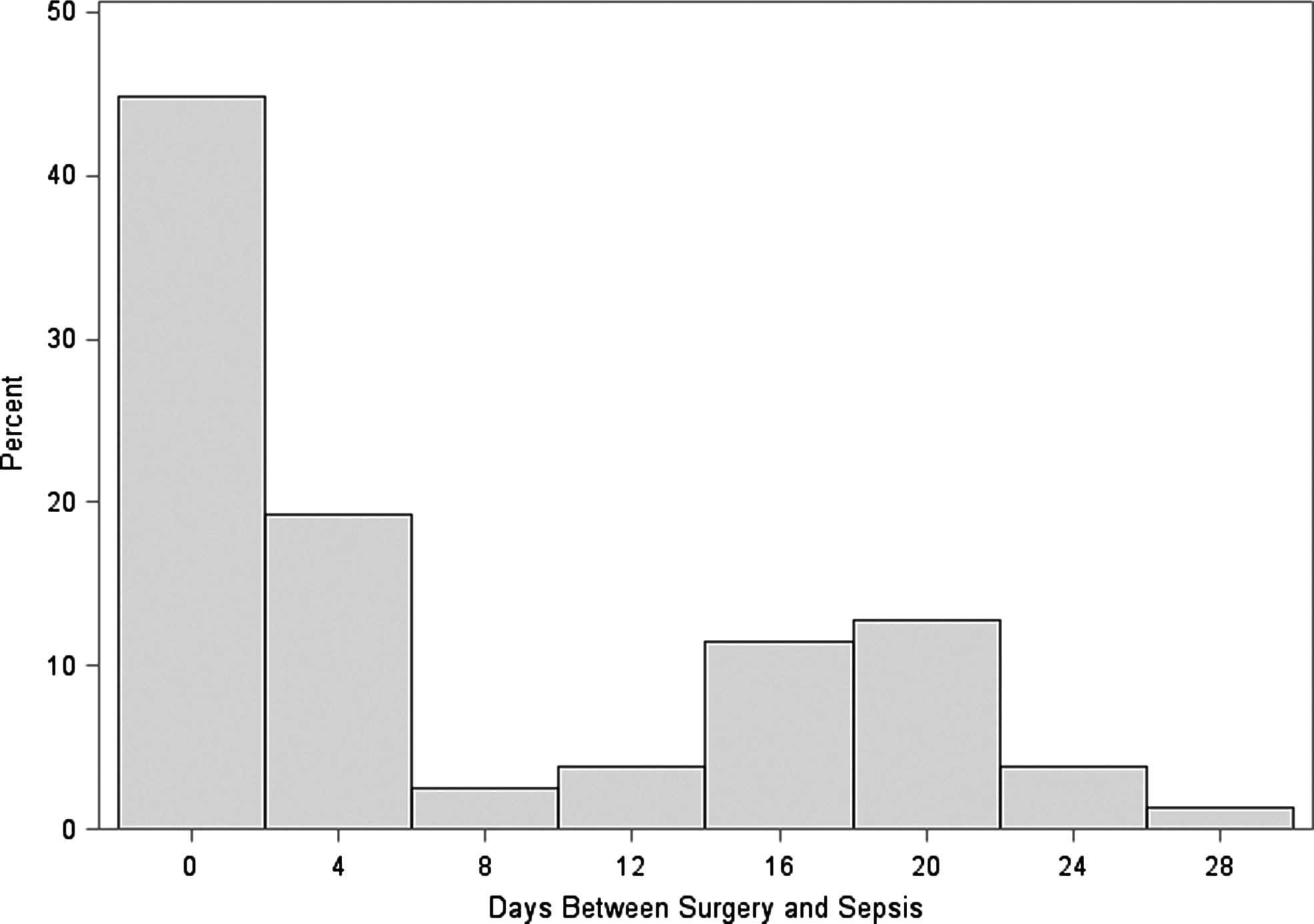
The interval between surgery and a sepsis diagnosis.
OR=odds ratio; CI=confidence interval.
Statin use, however, was not associated with any protective effect against postoperative sepsis (OR, 1.61; 95% CI, 0.91 to 2.86; P=0.105). As shown in Figure 2, statin users had adjusted rates of postoperative sepsis comparable to those of nonusers (5.3% vs 3.5%, respectively; P=0.105). In addition, UTI and ICU utilization rates also did not differ between statin users and nonusers (P=0.113 and P=0.666, respectively). Although the mean of hospital LOS was shorter in favor of statin users, this difference was trivial clinically (3.6 vs 4.1 days; P=0.007).
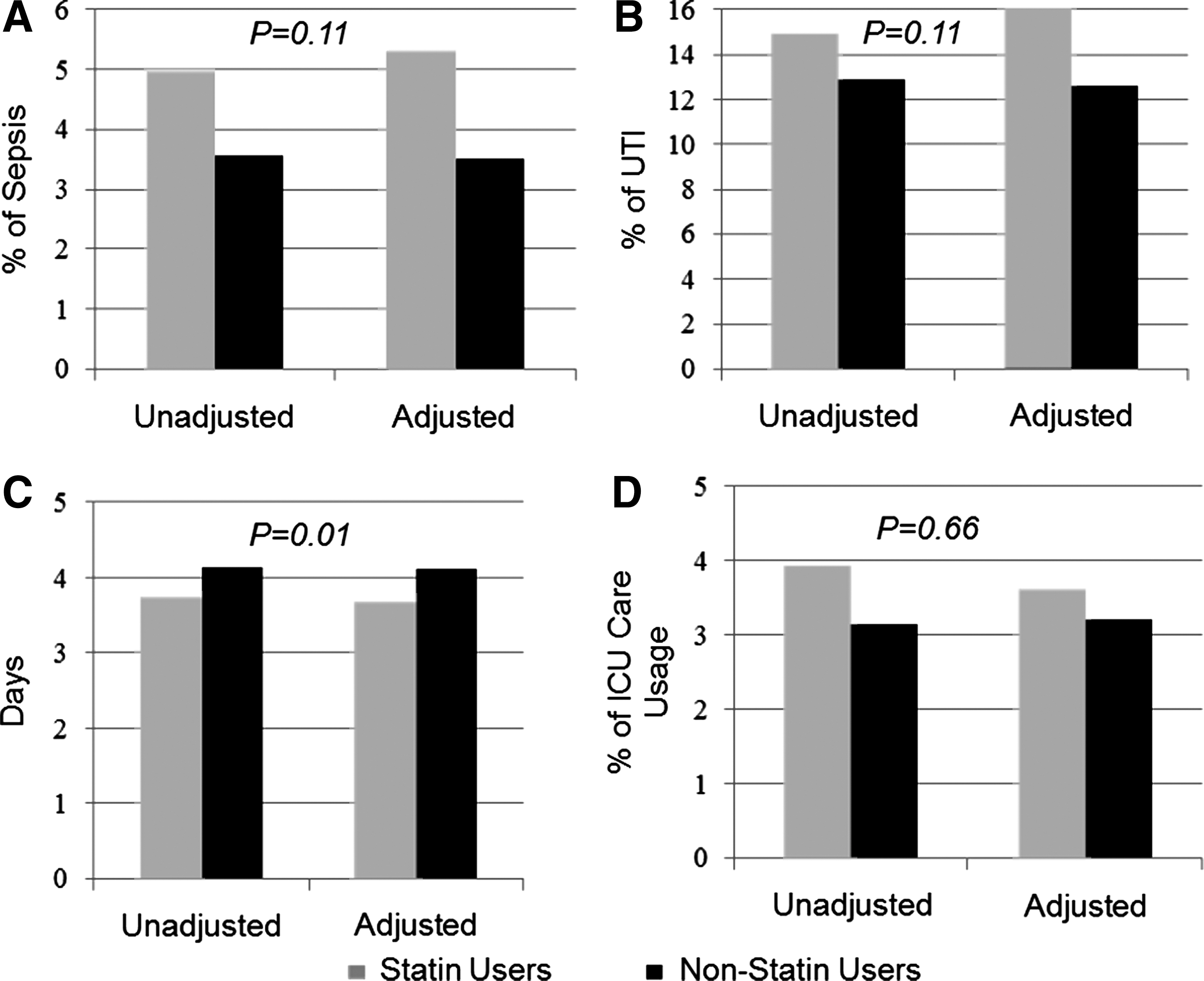
Statin outcomes. (
Discussion
We found that the use of a statin medication was not associated with reduced rates of sepsis after PCNL. UTI and ICU utilization rates also did not vary by statins use. While this class of medications may have other salutary effects on patient health, our collective findings do not support the use of statin medications for sepsis prophylaxis among PCNL patients.
One explanation for the lack of effect is because of insufficient statistical power. Therefore, we performed a post hoc power calculation to determine the minimum detectable effect size in our study. With 2046 patients in our cohort (382 statin users) and a 5% type I error, we had 80% power to detect a 50% reduction in rate of sepsis between our treatment and comparison groups. We observed, however, in both unadjusted and adjusted models, a higher rate of sepsis in our statin user group. Therefore, we are not worried about insufficient power to detect a clinically meaningful reduction in sepsis rate.
Our study is not the first one to call into question the statin utility for decreasing the infectious complications in medical or surgical patients, however. 23 –25 In a recent meta-analysis, pooled data from 11 trials reporting on the incidence of infection among statin users found that statin use had no effect on infection risk. 26 Moreover, among patients who underwent cardiac surgery, Trezzi and associates 27 found no significant difference in the rate of postoperative infection in patients who were receiving statins (4.3%) compared with patients who were not receiving statins (3.8%).
Data from our study highlighted some patient-specific factors that were associated with sepsis: The level of comorbidity, a history of previous sepsis or UTI, and the ambulatory status of the procedure. Clinicians could use this information when counseling patients on their sepsis risk. We did not find any statistically significant association between sepsis and age, sex, preoperative antibiotic use, or insertion of a drainage tube before the surgical procedure.
There are several limitations to our study. First, because of the observational nature of our study, the potential for residual confounding exists. Second, while we accounted for many patient-level variables associated with sepsis as well as validated measures of comorbidities (the Charlson index), certain factors, such as obesity, stone type, and procedure duration, may impact a patient's sepsis risk and are not measurable using sources of administrative data. Third, our patient cohort was limited to working-age adults with insurance. While this population may limit the external validity of our results, it is important to note that this subgroup represents the one most commonly affected by urinary stone disease. 28
Finally, one limitation of working with claims data is that we know whether or not the patients filled the prescription but do not know if the patient actually took the medication as prescribed. It is possible that issues related to a patient's noncompliance with prescribed therapy could affect our results. That being said, drug information from MarketScan database is widely used. 29
Notwithstanding these limitations, our study has clinical implications for the treatment of patients undergoing PCNL. While statin therapy may not be beneficial, there are compelling data on the utility of intraoperative renal pelvis urine cultures and stone cultures for predicting postoperative sepsis. 30 Given our findings, urologists who perform PCNL would be better served by directing their attention to tests like these, specifically for the patients with high comorbidities and previous history of UTIs. Moreover, there may be a role for clinical care pathways, which may aid in the early recognition and management of sepsis, thereby lowering its associated morbidity and mortality.
Conclusions
Our study does not support the use of statins for decreasing the risk of sepsis in patients undergoing PCNL. Urologists who care for patients with urinary stone disease should focus their attention on other processes of care to prevent sepsis in this population.
Footnotes
Acknowledgment
Supported by the Agency for Healthcare Research and Quality Grant 1K08HS020927 01A1 (JMH).
This article was published as an abstract—Abstract # MP09-07: J Endourol 2014;28(suppl 1):P1-A316.
Author Disclosure Statement
No competing financial interests exist.