
Abstract
Purpose:
This prospective single-arm multicenter clinical trial was conducted to evaluate the safety and efficacy of the Sun's tip-flexible semirigid ureterorenoscope (tf-URS) when used for managing upper urinary tract stones.
Patients and Methods:
Data from patients who underwent ureteroscopy using the tf-URS for proximal and renal stone removal were prospectively collected from seven Chinese clinical centers. The primary study end point was the stone clearance at the 2-week follow-up. Other data associated with the procedure were also collected.
Results:
Between October and December of 2014, this study enrolled a total of 254 patients; among which, 235 patients were eligible for ureteroscopy, 216 of whom were treated using the tf-URS. Among all treated patients, 135 had proximal ureteral stones (group 1) while 81 had renal stones (group 2). The overall success rate of endoscope advancement was 91.9% (216/235). The mean fragmentation times were 17.5±12.6 minutes and 23.3±15.1 minutes for groups 1 and 2, respectively, and corresponded to an experience-dependent increase in fragmentation speed in both groups. The mean operative times were 31.9±15.5 minutes and 39.5±2 0.3 minutes for groups 1 and 2, respectively. The access rate to renal stones in group 2 was 96% (76/81). All treated patients were assessed during a 2-week follow-up period. The stone-free rates at the 2-week follow-up for groups 1 and 2 were 98.7% (133/135) and 91.3% (74/81), respectively. Adverse events were observed in 7.3% (16/216) of the patients; however, all were classified as Grade I or Grade II complications.
Conclusions:
Based on our initial experience in the current study, the tf-URS can be safely and effectively used to manage proximal ureteral and renal stones with a low rate of complications. Future studies are needed to focus on a transverse comparison between the tf-URS and conventional ureteroscopes.
Introduction
B
Ureteroscopes are commonly divided into two categories based on their structure. A semirigid ureteroscope (r-URS) is suitable for managing distal or midureteral stones. 3 Because of its straight metal shaft that cannot be deflexed, however, a r-URS is not capable of managing renal stones. A flexible ureteroscope (f-URS) a has totally flexible shaft and active deflection, thus is suitable for removing renal stones and proximal ureter stones. A f-URS still has some disadvantages, however, including its poor maneuverability and the difficulty of insertion into the ureter. 4
In 2013, we developed a novel endoscopic device that integrated the functions of both the r-URS and f-URS, and named it the Sun's tip-flexible semirigid ureterorenoscope (tf-URS). The current study was conducted to evaluate the impact of this new device on the clinical outcomes when managing UUTS.
Patients and Methods
Patients
Data from consecutive patients who underwent ureteroscopy using the tf-URS for proximal and renal stone removal were prospectively collected from seven clinical centers in China (Changhai Hospital of the Second Military Medical University; the First Affiliated Hospital of Guangzhou Medical University; Xiangya Hospital of Central South University; Ningbo First Hospital of Ningbo University; West China Hospital of Sichuan University; Tsinghua Changgung Hospital; Yantai Yuhuangding Hospital of Qingdao University). All sites obtained study approvals from their ethics committees, and the patients were counseled concerning the purpose and risks of the study and provided a signed informed consent. The main eligibility criterion was stones <2 cm. Additional details pertaining to the inclusion and exclusion criteria are listed in Table 1.
CT=computed tomography; IVU=intravenous urography.
Study design
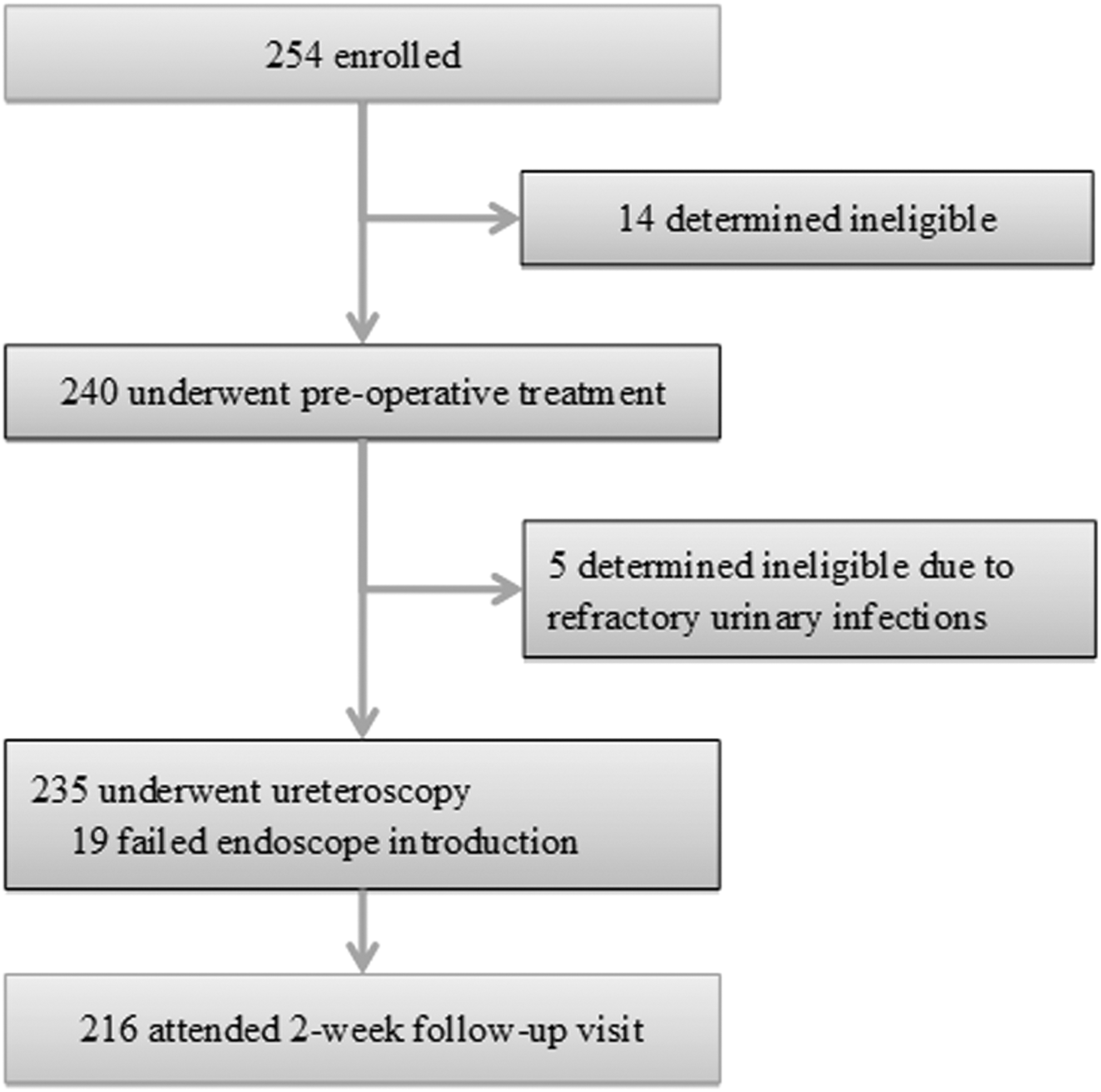
This study was an open-label, prospective, multicenter, single-arm trial that enrolled patients from seven clinical centers in China. Figure 1 shows a flowchart for the study, including its treatment and follow-up phases. The primary study end point was the stone clearance at a 2-week follow up visit. For purposes of this study, “stone free” was defined as the patient having gravel particles <0.2 cm.
Study design.
Data were also collected for the following parameters: (1) The stone clearance on the first postoperative day; (2) endoscope advancement results; (3) the time associated with the surgery, including the full operative time, endoscope advancement time, the total time needed to inspect the collecting system of the renal stone patients, and the fragmentation time; (4) the requirement for stone relocation to facilitate fragmentation of renal stones; (5) adverse events and their classifications according to the modified Clavien-Dindo grading system; 5 (6) postoperative treatments including the postoperative stay, any secondary treatments, and the need for readmission within two weeks after surgery; (7) endoscope damage and endoscope repair frequency.
Endoscopic device
The tf-URS (SN-V, Hawk Endoscopes, China) has been approved for clinical applications by the China Food and Drug Administration. The design of the tf-URS is unique in that it consists of a retractable rigid sheath and a r-URS with a 9-cm flexible part on the tip (Fig. 2). The rigid/flexible working modes can be switched by releasing the flexible tip. Duel 250-degree/270-degree deflection can be manipulated by the lever on the handle. The tf-URS is 8.2/8.7F in diameter at the tip of the inner-shaft/outer-sheath, and 9.8F in diameter at the bottom of the sheath. It also has a 3.6F working channel for auxiliary instruments. In addition, the tf-URS contains an independent outflow channel along the interspace between the shaft and the sheath that enables continuous outflow.
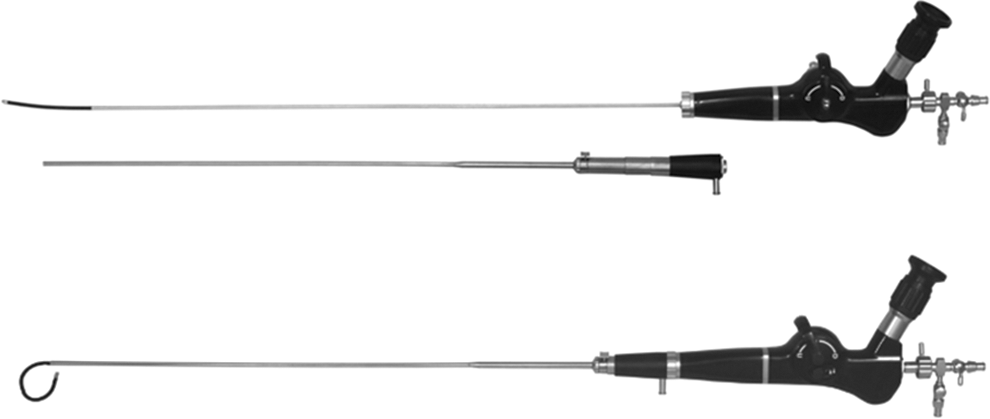
Separate and assembled structures of the Sun's tip-flexible semirigid ureterorenoscope.
Preoperative treatments
Several examinations were performed before each surgery, and the subjects were restricted to those with mild or moderate hydronephrosis (<3 cm) based on their ultrasonography results. Stone burden was calculated as the sum of the sizes of all stones size (length×width×0.25×3.14159) as seen on radiography and intravenous urography. CT was also performed to evaluate stone burden and location when a subject had radiopaque stones or faint radiography results.
All patients received a single dose of antibiotic (ciprofloxacin) if their urine culture showed negative results; otherwise, they were continued on a sensible antibiotic regimen until their culture results were negative. Patients who had ipsilateral prestent placement or a previous ureteroscopy within the previous 6 months were excluded from the study.
Surgical procedures
Each clinical site had one fixed surgeon and two assistants. All surgeons were skilled in semirigid and flexible ureteroscopy and had previously treated >500 patients.
Retrograde ureteroscopy was performed in a supine lithotomy position under general anesthesia, and irrigation was provided by one assistant using a syringe. The tf-URS was advanced through the ureter along the guidewire under visual and fluoroscopic guidance. For subjects with proximal ureteral stones, the 200 μm laser fiber was introduced to proceed with stone disintegration after the safety wire was in place. Pulse settings began at 0.6 J and a frequency of 15 Hz and were increased to 1.0 J at 15 Hz if the stone was hard. The tf-URS was maintained in “rigid mode” during the procedure within the ureter.
For patients who had renal stones or in whom proximal ureteral stone retropulsion was encountered, the tf-URS was further advanced into the renal pelvis. The endoscope was then switched to “flexible mode” by extending the tip of the inner flexible shaft. After fully inspecting the collecting system and determining stone location, disintegration was performed using the 200 μm laser fiber at settings of low energy and high frequency. Stone dusting was considered to be satisfactory when each piece of gravel was <0.2 cm. Subsequently, fluoroscopy was used to detect the presence of any residual fragments. After extracting a single fragment for component analysis, the tf-URS was withdrawn along the guidewire, and a 6 F Double-J stent was placed routinely.
Postoperative treatments and follow-up
All subjects underwent antibiotic therapy after surgery, and radiography was performed on the following day. At the 2-week follow-up visit, the Double-J stent was removed by cystoscopy, and the final stone-free rate (SFR) was assessed by radiography.
Results
Study population
Between October and December, 2014, a total of 254 subjects were recruited, of whom 14 were excluded based on exclusion criteria. The remaining 240 patients underwent preoperative preparation; however, 5 patients were deemed ineligible because of refractory urinary infections. Finally, a total of 235 eligible patients underwent ureteroscopy, of whom 216 were treated using the tf-URS. All treated patients were available for the 2-week follow-up visit and completed the study. Basic characteristics of the treated patients are summarized in Table 2.
Data are mean±standard error of the mean.
Features of the stones
Among the 216 treated patients, 135 had proximal ureteral stones (group 1), and the remaining 81 patients had renal stones (group 2). The average number of stones per patient was 1.4±0.8 (range 1–4), and the mean stone size was 1.4±0.5 cm (range 0.4–2.0 cm). Among subjects with renal stones, the stone locations included upper calix (9.8%, 8/81), middle calix (8.6%, 7/81), lower calix (13.6%, 11/81), renal pelvis (40.7%, 33/81), and multiple sites (32.1%, 26/81). Among all stones, 81% were composed of oxalate, while the others were composed of phosphate (8%), uric acid (8%), or were mixed stones (3%). Details of the stone features are listed in Table 2.
End points
When including all treated subjects (except 19 who failed endoscope introduction), the immediate SFR on the first postoperative day was 94.0% (203/216), and the final SFR at the 2-week follow-up visit was 95.8% (207/216). Data pertaining to these outcomes are shown in Table 3.
Data are mean±standard error of the mean.
Perioperative results
The overall success rate for endoscope advancement was 91.9% (216/235). The mean time for endoscope advancement in group 1 was 2.9±1.5 minutes (range 1.0–8.0 min, from insertion into the ureter to arrival at the ureteral stone) and 3.0±1.6 minutes in group 2 (range 1.0–5.5 min, from insertion into the ureter to arrival at the renal pelvis). The mean time needed to inspect the collecting system for group 2 subjects was 2.3±0.7 minutes (range 1.5–8.0 min), and the stone access rate for group 2 subjects was 96.0% (78/81).
The mean fragmentation times were 17.5±12.6 minutes (range 2.0–75 min) and 23.3±15.1 minute (range, 12.0–60.0 min, including stone relocation using the basket) for groups 1 and 2, respectively; which corresponded to mean fragmentation speeds of 8.1±3.0 mm2/min and 7.3±1.7 mm2/min, respectively. The mean operative times (including placement of the Double-J stents) in groups 1 and 2 were 31.9±15.5 minutes (range 10.0–96.0 min) and 39.5±20.3 minutes (range 15–92 min), respectively.
Stone retropulsion during the lithotripsy was encountered in 21.5% (29/135) of all group 1 patients and necessitated further advancement of the tf-URS into the renal pelvis to continue surgery. Among all group 2 patients, 33.3% (8/24) had stones located at the lower calix that could not be reentered when the laser fiber was introduced, and these patients necessitated stone relocation using a basket. Stones access was not completed in three patients in whom the renal stones were located at the lower calices. These three patients had small infundibulopelvic angles (<5 degrees) and long lengths of the caliceal infundibulum (>3.5 cm). For the three patients, we changed our procedures and used conventional f-URS; however, this conversion did not permit stone access either.
The mean length of the postoperative stay for all patients was 1.9±1.1 days (range 1–8 days), and 1.4% (3/216) of patients needed a second procedure.
Data pertaining to the perioperative results are presented in Table 3.
Complications
All adverse events classified by the modified Clavien-Dindo grading system are presented in Table 4. Complications were observed in 7.3% (16/216) of all patients. Grade I complications were observed in 11 (5.1%) patients and included moderate pain, hematuria, and other types of discomfort. Grade II complications were observed in five (0.5%) patients and included fever, severe pain, and postoperative obstruction. One patient was readmitted for acute obstruction after Double-J stent removal at the 2-week follow-up, but later expelled the stones after medical expulsive therapy. No Grade III or Grade IV complications were observed in the current study.
Data are mean±standard error of the mean.
Endoscope damage
There were three endoscope failures in the study. One endoscope lost one-way deflection when managing the lower pole stone after six usage times. Leakage of the working channel was observed in another endoscope caused by the improper operation of the surgeon (laser fiber accidental injury) after 21 usage times. One other endoscope generated more than five black dots on endoscopic images; however, this issue had no significant effects on procedures.
Discussion
During the past several decades, the management of UUTS has been significantly impacted by substantial improvements in the surgical treatment armamentarium. In 2003, we developed a first generation tf-URS for use in retrograde ureteral and intrarenal surgeries and demonstrated its efficacy by achieving an 83% SFR at 1 month postsurgery. 6 To the best of our knowledge, this ureterorenoscope was the first to integrate advantages associated with the use of both rigid and f-URS.
In 2013, we presented a new version of the tf-URS and named it the Sun's tip-flexible semirigid ureterorenoscope. We conducted the current study to evaluate the ureteroscopic outcomes achieved when using this novel device for treating patients with UUTS. Because management of larger stones necessitated a prolonged operative time and involved an increased risk for tissue damage, the American Urological Association/EAU suggested that ureteral and renal stones managed using an endoscopic approach should be limited to 2 cm, 1,7 and thus stone size was restricted to 2 cm in the current study.
Whether or not stone fragments should be retrieved remains controversial. 8 The tf-URS must be withdrawn back into the bladder and subsequently readvanced to extract stone fragments. This process could be time consuming and increase the risk for tissue damage. 9 We therefore preferred stone dusting rather than stone extraction.
Because of its straight metal shaft, the r-URS is considered to be maneuverable. When the tf-URS is maintained in the “rigid mode” with the flexible tip withdrawn in the sheath, it can be manipulated in a manner identical to a conventional r-URS and is capable of passing either the orifice or the physiologic tortuosity of the ureter with ease like a r-URS.
The tf-URS is 8.2/8.7F in diameter for the inner-shaft/outer-sheath at the tip and is 9.8F at the bottom of the sheath, which is larger than the commercially latest available f-URS and even smaller r-URS. According to the EAU guidelines, 1 however, a ureter access sheath (UAS) is recommended in flexible ureteroscopy. When compared with the most commonly used UAS (12/14F), the tf-URS is smaller, which indicates that retrograde intrarenal surgery using the tf-URS does not need a larger caliber of the ureter than a common flexible ureteroscopy.
Although the smallest r-URS is only 4.5F in diameter, the most commonly used r-URS in China is the 8/9.8F endoscope (8703.534, Wolf, Germany) that is similar to the tf-URS in endoscopic caliber.
In our study, the success rate of endoscope advancment was 91.9% and the SFR for proximal stones was 98.7%. These results were comparable to common ureteroscopic outcomes that have been reported, 10 which indicated that the caliber of the tf-URS did not significantly influence the outcomes for the management of UUTS.
The Clinical Research Office of the Endourological Society recently reported that the overall SFR for proximal ureteral stones managed with ureteroscopy was 84.5%, 11 but decreased to 63.4% when only a r-URS was available. This result is thought to be attributable to potential retropulsion. 7,12 In the current study, stone retropulsion was observed in 21.5% (29/135) of the patients with a proximal ureteral stone. In these cases, the tf-URS could be further advanced up to the renal pelvis without assistance from the UAS, and then switched to the “flexible mode” to complete the disintegration of migrated stones. Surgeons only needed to make a simple thumb motion to control the duel deflection of the flexible tip.
In this study, the SFR for proximal ureteral stones managed using the tf-URS was 98.7% (133/135), which was significantly higher than the SFR achieved using a conventional r-URS as other investigators reported, 12 indicating that the tf-URS is suitable for managing proximal ureteral stones.
Wendt-Nordahl and colleagues 13 demonstrated that the 270-degree f-URS provided increased access to lower calices and a higher SFR compared with that achieved using a 180-degree f-URS, suggesting that high deflection is essential for better results. 14 When working in the “flexible mode,” the tf-URS has a dual active deflection of 250 degrees/270 degrees (up and down) at the tip, and this is similar to the majority of commercially available f-URSs. 15 Therefore, the tf-URS is capable of managing renal stones in various calices.
In the current study, the stone access rate was 96.0% (78/81). Consistent with results from previous studies, 13,14,16 the tf-URS also showed some deflection loss when an auxiliary instrument was introduced; nevertheless, a high deflection was still retained. Relocation of lower pole stones with a 1.7F basket could still be achieved in all patients with stones located at the lower pole calices that could not be accessed when the laser fiber was inserted. Although the treatment procedures for three patients were changed to use a flexible ureteroscope when the tf-URS could not access the lower pole calices, the conversion did not allow us to complete these procedures because of the complicated location. The final SFR for renal stones was 91.3% (74/81), which is similar to that reported for flexible ureteroscopy 17 and suggests that the tf-URS can achieve good renal stone clearance.
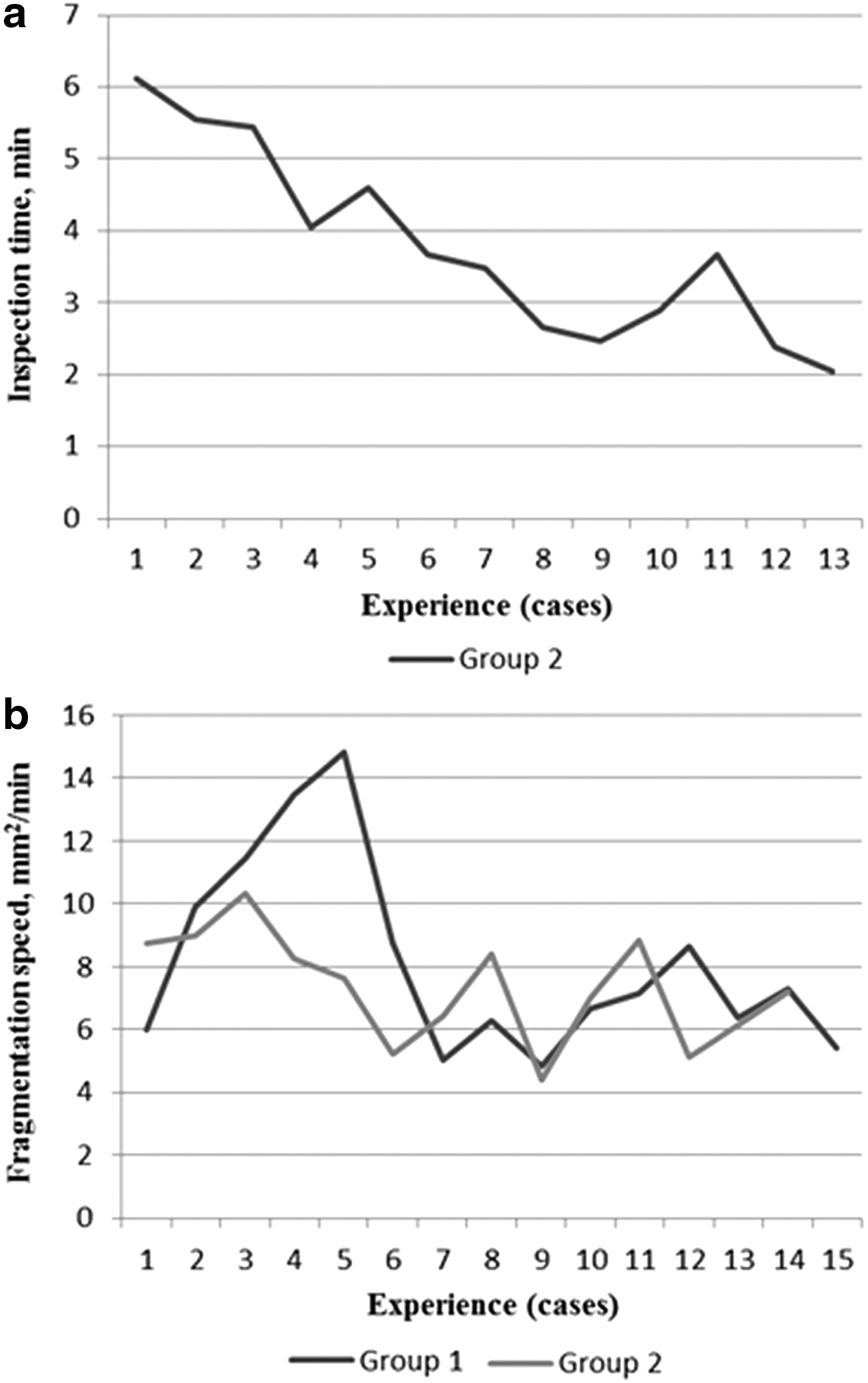
It may be argued that the full inspection and the disintegration times in our study were still quite long when compared with those achieved using conventional ureteroscopes; however, these times were reduced as the experience of the surgeons increased (Fig. 3a). In addition, the mean fragmentation speeds for proximal ureteral stones and renal stones were 8.1±3.0 mm2/min and 7.3±1.7 mm2/min, respectively, and showed obvious improvements with increased operative experience (Fig. 3b). These results may reflect a rather short tf-URS learning curve for surgeons with previous f-URS experience.
Similar to conventional URS, ureteroscopy using the tf-URS was initiated in a natural orifice suitable for performing transluminal endoscopic surgery and thus had a very low rate of complications. 18 Adverse events were observed in 7.3% (16/216) of all patients, and were classified as either Grade I or Grade II complications. Unlike other investigator reports regarding use of the f-URS, 9 there were no perforations or severe ureteral wall injuries in any of the patients in the current study. This is likely attributable to our use of “vision-guided endoscope advancement,” which allowed the surgeons to obtain clear images and avoid perforations.
There are three notable limitations of the current study. First, this single-arm study may have produced less convincing results when compared with those that might have been shown by a controlled trial; however, our initial clinical experience indicated that the novel endoscope provided a satisfactory SFR accompanied by few complications, which is quite encouraging. A prospective randomized controlled trial is currently being planned, and will soon be conducted to provide a better comparison of the conventional and new endoscopic techniques.
A second limitation is the exclusion of patients with hydronephrosis >3 cm on ultrasonography. The presence of severe hydronephrosis would significantly increase the difficulty of surgery, even when using a f-URS with a totally flexible shaft. The length of the flexible portion of the tf-URS is 9 cm, which makes if difficult to fully inspect the collecting system in subjects with severe hydronephrosis. The clinical conditions best treated by ureteroscopy with the tf-URS are still being determined, and further studies are needed to focus on this issue.
The third limitation of this study is its relatively short follow-up period. We noticed, however, that most of the subjects had already shown rather favorable outcomes within 2 weeks after surgery. In addition, as summarized in the EAU guidelines, 1 the complication rates for ureteroscopy range from 9% to 25%, and most complications are observed during the intraoperative or early postoperative periods. The late complication rate is only 0.2%, which accounts for a very small proportion of the total complications. These two facts suggest that the follow-up duration used in our current study was sufficient to evaluate the safety and efficacy of the new device.
Conclusion
As a novel ureterorenoscope that integrates the functions and advantages of both the r-URS and f-URS, the tf-URS provides a simple means of performing retrograde ureteral and intrarenal surgery and was proven capable of safely and effectively managing proximal ureteral and renal stones with a low rate of complications. A future controlled study is needed to compare the tf-URS with conventional ureteroscopes.
Footnotes
Acknowledgment
This work was supported by the National “863” High Tech Program of China (2012AA021102).
Disclosure Statement
No competing financial interests exist.