
Abstract
Purpose:
To assess whether our ureteroscopic real-time navigation system has the possibility to reduce radiation exposure and improve performance of ureteroscopic maneuvers in surgeons of various ages and experience levels.
Materials and Methods:
Our novel ureteroscopic navigation system used a magnetic tracking device to detect the position of the ureteroscope and display it on a three-dimensional image. We recruited 31 urologists from five institutions to perform two tasks. Task 1 consisted of finding three internal markings on the phantom calices. Task 2 consisted of identifying all calices by ureteroscopy. In both tasks, participants performed with simulated fluoroscopy first, followed by our navigation system. Accuracy rates (AR) for identification, required time (T) for completing the task, migration length (ML), and time exposed to simulated fluoroscopy were recorded.
Results:
The AR, T, and ML for both tasks were significantly better with the navigation system than without it (Task 1 with simulated fluoroscopy vs with navigation: AR 87.1 % vs 98.9%, P=0.003; T 355 s vs 191 s, P<0.0001; ML 4627 mm vs 2701 mm, P<0.0001. Task 2: AR 88.2% vs 96.7%, P=0.011; T 394 s vs 333 s, P=0.027; ML 5966 mm vs 5299 mm, P=0.0006). In both tasks, the participants used the simulated fluoroscopy about 20% of the total task time.
Conclusions:
Our navigation system, while still under development, could help surgeons of all levels to achieve better performances for ureteroscopic maneuvers compared with using fluoroscopic guidance. It also has the potential to reduce radiation exposure during fluoroscopy.
Introduction
I
With advances in engineering technology, the use of retrograde intrarenal surgery (RIRS) using high-performance flexible ureteroscopes has been increasing. With the expanding use of flexible ureteroscopy, the use of fluoroscopy is also increasing. Urologists should make an effort to reduce radiation exposure of both patients and urology staff. Although an effective radiation protocol for ureteroscopy has been reported, 2 –5 there are no reports on the use of a novel navigation system as a method to reduce the need for fluoroscopy.
In the present study, we developed simulated fluoroscopy and compared its ability to maintain spatial orientation of the ureteroscope with that of our novel navigation system. This study was performed in multiple centers with surgeons of various experience levels and ages. We evaluated the potential for reduced radiation exposure using our navigation system.
Materials and Methods
Ureteroscopic navigation system
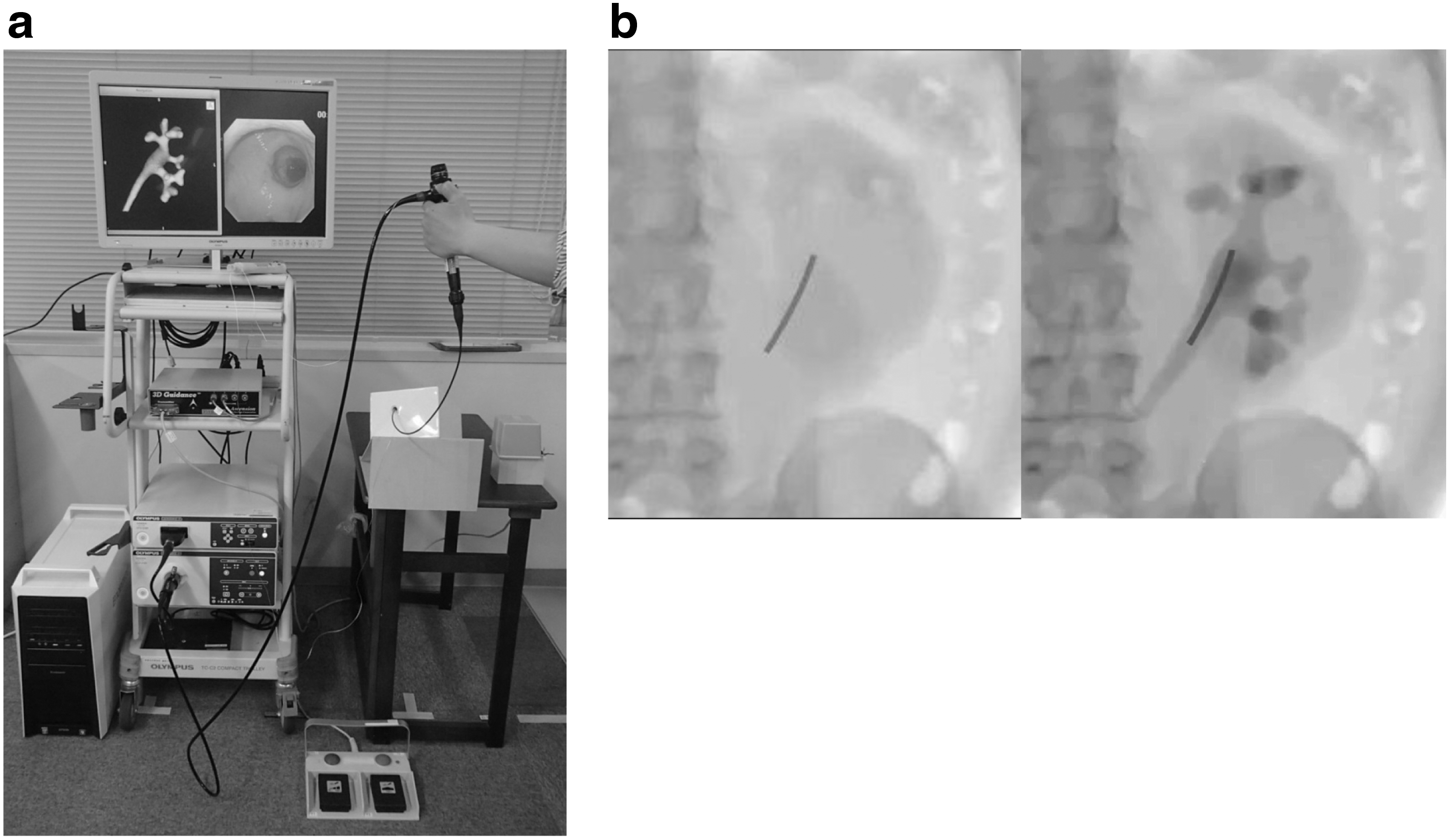
Our ureteroscopic navigation system (Fig. 1a) uses a magnetic tracking system (3D-Guidance medSAFE; Ascension Technology Corp., Milton, VT) and an ureteroscope (URF Type-V; Olympus, Tokyo, Japan). A magnetic field measurement device was used to track the positions of two sensors on the ureteroscope. A cord with sensors was passed through the channel of the ureteroscope to track the position of the ureteroscope in the magnetic field. A pyelocaliceal phantom was created using the modified Digital Imaging and Communications in Medicine (DICOM) CT data (slice thickness, 1 mm) obtained from a patient. We obtained informed consent from a patient to make the phantom model. The pyelocaliceal phantom has an inner cavity for endoscopy and internally marked calices. On the main monitor, a three-dimensional (3D) image and the endoscopic image are displayed. The tracked positions of the tip of the ureteroscope were displayed in real time on the navigation image. Using a foot pedal with two buttons, the operator could rotate the 3D navigation image to view the depth and current position of the tip of the ureteroscope.
Simulated fluoroscopy
To evaluate fluoroscopy exposure time, a system of simulated fluoroscopy (Fig. 1b) was developed. DICOM CT data were used to make a simulated fluoroscopic image. This image included a vertebral body, rib bone, iliac bone, and kidney, as a C-arm image would. The two-dimensional simulated fluoroscopic image was used to confirm the position of the ureteroscope on a secondary monitor. The surgeons were able to rotate the image to maintain depth perception and inject contrast medium into the urinary tract to confirm its shape. The contrast image was set to disappear automatically after 60 seconds. The elapsed time of simulated fluoroscopy was measured.
Participants and tasks
Thirty-one urologists were recruited from five institutions. For subgroup analysis, they were divided into two groups: 15 junior residents (14 male and 1 female, postgraduate years [PGY]<10, Group A) and 16 senior residents (all male, PGY ≥10, Group B).
To evaluate their performance during ureteroscopic maneuvers, the participants were administered two tasks to examine the inside of the phantom. They completed Task 1 first, followed by Task 2. In each task, they first performed using simulated fluoroscopy and then using the novel real-time navigation system without simulated fluoroscopy. Before performing Tasks 1 and 2, they confirmed the 3D image showing the shape of the pyelocaliceal model and three designated calices. The time limit for each task was 600 seconds.
In Task 1, the three calices (anterosuperior, anteromiddle, and anteroinferior) were internally marked with blue dots that represent tumors. First, the participants were asked to navigate using only simulated fluoroscopy and record their position using a foot pedal when they thought the tip of the ureteroscope had reached the blue markings. The recorded positions were not displayed on the 3D image. After that, the participants performed the same task using the real-time navigation system. In this navigation system, they could rotate the 3D image using the foot pedal and identify the current position of the tip of the ureteroscope. They were again asked to record the position of the tip when they reached the blue markings.
In Task 2, participants were asked to examine all 15 calices of the phantom, first with simulated fluoroscopy and then with navigation. Using each system, they marked their position when they reached each papilla.
Evaluation of ureteroscopic maneuvers
The accuracy rate (AR) of identifying the marked calices, migration length (ML) of the tip of the ureteroscope, time (T) taken to complete the task, and time exposed to simulated fluoroscopy (sFT) were recorded for Tasks 1 and 2. The AR for Tasks 1 and 2 were calculated as follows:
For measurement of ML and T, the beginning of the task was defined as the time of ureteroscope insertion into the pyelocaliceal phantom, and the end of the task was defined as the time of ureteroscope removal from the phantom. The sFT was defined as the total time the foot pedal was pressed. The percentages of sFT were calculated by dividing sFT by T to clarify the proportion of time the surgeon chose to use fluoroscopy.
The ML was calculated as follows:
Statistical analysis
Continuous variables are expressed as mean (range). Performance data were compared between the performances with simulated fluoroscopy and those with navigation using the Wilcoxon test. Statistical analyses were performed using Microsoft Excel for Windows and a P value of <0.05 was considered statistically significant.
Results
AR for Task 1 and Task 2
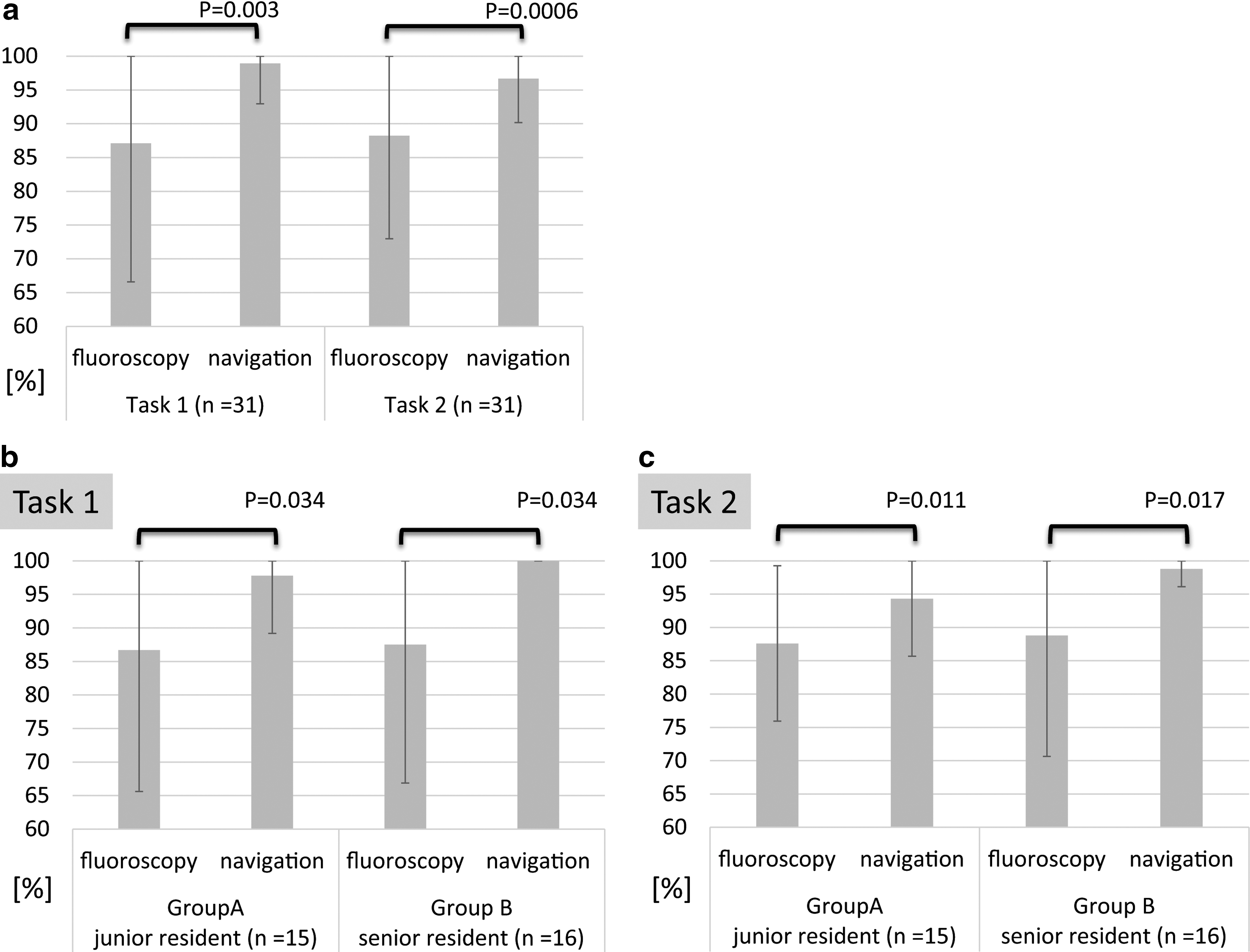
The AR for both Tasks (Fig. 2) was significantly better in both Groups A and B with the navigation system than with simulated fluoroscopy (Task 1: Overall fluoroscopy vs navigation: 87.1% [33.3%–100%] vs 98.9% [66.7%–100%], P=0.003; Group A 86.7% [33.3%–100%] vs 97.8 % [66.7%–100%], P=0.034; Group B 87.5% [33.3%–100%] vs 100%, P=0.034; Task 2: Overall 88.2% [53.3%–100%] vs 96.7% [73.3%–100%], P=0.0006; Group A 87.6% [66.7%–100%] vs 94.3% [3.3%–100%], P=0.011; Group B 88.8% [53.3%–100%] vs 98.8% [93.3%–100%], P=0.017; Wilcoxon test). These results suggest that the navigation system had advantages for both junior residents and for senior urologists.
T
T for Task 1 and Task 2 (Fig. 3) was significantly shorter with the navigation system than with simulated fluoroscopy alone (Task 1: Fluoroscopy vs navigation: 356 s [127–600 s] vs 191 s [69–600 s], P<0.0001; Task 2: 394 s [163-–600 s] vs 333 s [144–600 sec], P=0.011; Wilcoxon test). When subgroups were analyzed, both groups had improved T in Task 1 when using the navigation system (Group A: 350 s [127–600 s] vs 196 s [69–600 s], P=0.0012; Group B: 361 s [160–600 s] vs 187 s [82–537 sec], P=0.0005; Wilcoxon test), while only Group A had significantly improved T in Task 2 (Group A: 416 s [236–600 s] vs 336 s [156–600 s], P=0.041; Group B: 375 s [163–600 s] vs 331 s [144–531 s], P=0.258; Wilcoxon test).

ML
The ML (Fig. 4) was significantly shorter with the navigation system for both Task 1 and Task 2 than with simulated fluoroscopy alone (Task 1: Fluoroscopy vs navigation: 4627 mm [1835–8777 s] vs 2701 mm [1084–9980 mm], P<0.0001; Task 2: 5966 mm [3044–11040 s] vs 5299 mm [2223–9786 mm], P=0.027; Wilcoxon test).
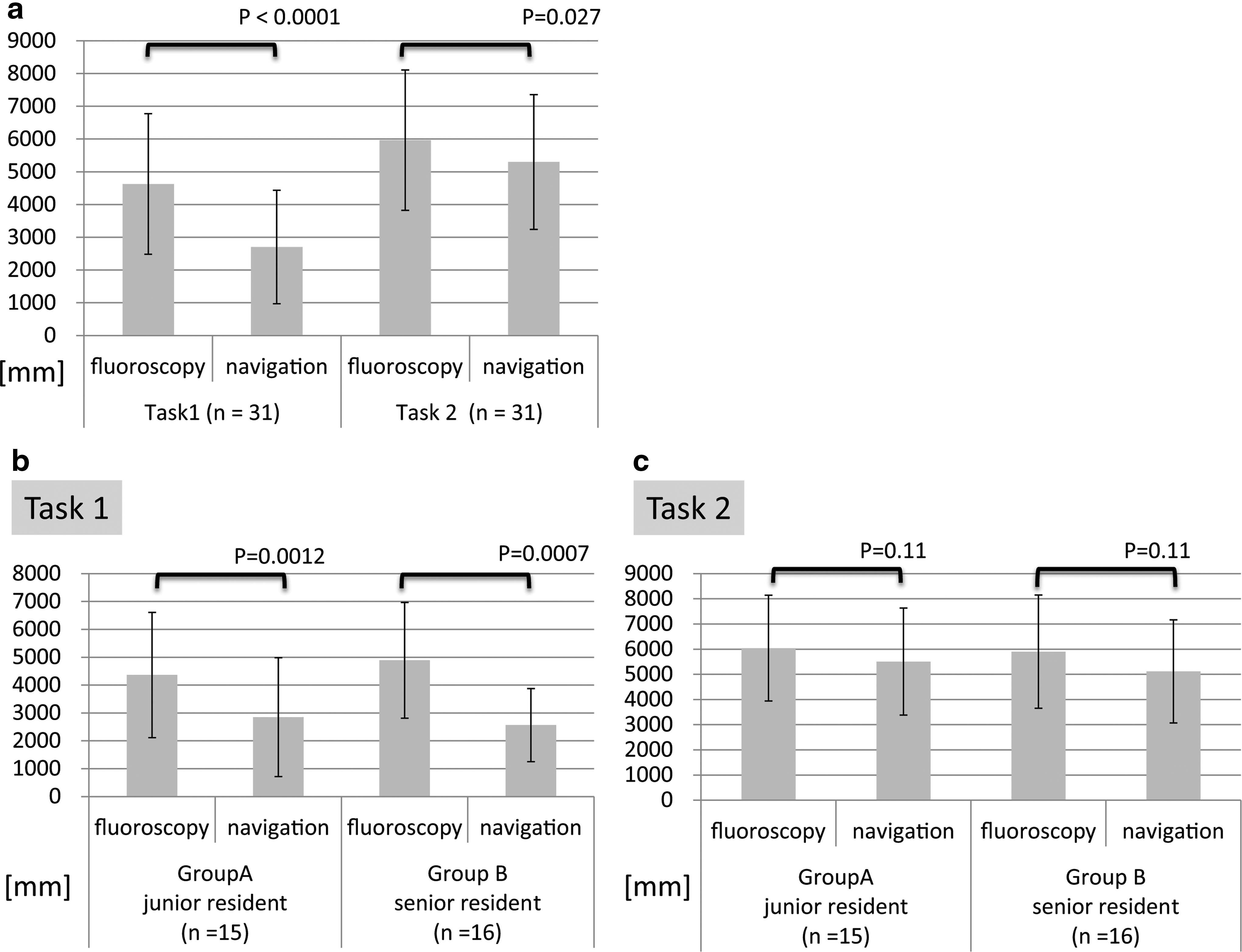
When analyzed by subgroups, the ML for Task 1 was significantly shorter with the navigation system in Groups A and B (Group A: 4363 mm [1835–8649 s] vs 2847 mm [1240–9980 mm], P<0.0001; Group B: 4890 mm [2287–8777 s] vs 2565 mm [1084–5495 mm], P=0.012; Wilcoxon test). The ML for Task 2, however, was not significantly different for either group (Group A: 6041 mm [3044–9455 s] vs 5507 mm [2278–9571 mm], P=0.11; Group B: 5900 mm [3064–11040 s] vs 5116 mm [2223–9786 mm], P=0.11; Wilcoxon test).
Duration of simulated radiation exposure
The sFT for Tasks 1 and 2 were 71 seconds and 57 seconds, respectively. The percentage of sFT for these tasks was 18.3% and 17.9%, respectively.
Discussion
In this report, we developed a system for simulated fluoroscopy and compared its ability to maintain spatial orientation of an ureteroscope to that of our navigation system. We also evaluated our system's potential to reduce radiation exposure to patients and urology staff.
With advances in ureteroscopic technology, it is now possible to manage many types of lesions using flexible ureteroscopy. With the increased use of endoscopic surgery of upper urinary tract calculi, including RIRS and endoscopically assisted intrarenal surgery, the use of fluoroscopy has also increased. Urologists should adhere to the “as low as reasonably achievable” principle to reduce the risks to themselves and to their patients. 6 In RIRS, macrohematuria and the complexity of the pyelocaliceal shape make it more difficult to identify the current position of the ureteroscope. Novice surgeons have a tendency to use fluoroscopy more often because they lose their spatial orientation. Weld and associates 7 reported the correlation of increasing ureteroscopic experience with decreasing fluoroscopy time by residents. Multiple studies have described an effective radiation reduction protocol to reduce fluoroscopy time during ureteroscopy. 2 –5 Despite these reports, it requires a lot of time and effort to minimize fluoroscopy time. Therefore, our navigation system, which shows the current position of the ureteroscope without fluoroscopy, could be helpful for decreasing fluoroscopy time.
Previously, we reported our novel navigation system for flexible ureteroscopic surgery in an ex vivo experiment. Although we evaluated performance during ureteroscopic maneuvers and found that our system could help increase AR (AR without navigation: novice surgeon 33%, expert surgeon 66.7%; with navigation: novice and expert surgeons 100%), the circumstances of the Task were different from true clinical operations. First, the participants were unable to use fluoroscopy to confirm the position of the ureteroscope. Second, the participants were asked to navigate through the noninternally marked phantom to the calices that they thought correct. Therefore, AR without navigation is slightly lower than with navigation. Furthermore, T and ML were not significantly different with and without navigation.
In the present study, the Tasks better simulated a true clinical setting. We developed the system to simulate fluoroscopy, which is widely used clinically. As a result, our current study showed that AR, T, and ML were significantly better with the navigation system than with simulated fluoroscopy alone. This confirms that our system has a better ability to maintain and regain the correct position of the ureteroscope over simulated fluoroscopy alone. Although there seems to be a learning curve for both tasks, we previously demonstrated that experience with the task without navigation does not impact the performance of the task with navigation. 1 Therefore, we decided that we did not need to perform the reverse study.
There are some limitations to our navigation system. First, our system needs registration between the pyelocaliceal phantom and CT DICOM data in the ex vivo experiment. It would be quite difficult to overcome the soft organ deformation in vivo. In partial nephrectomy, for example, there exist ex vivo data examining augmented reality that overlay preoperative 3D imaging reconstructions onto intraoperative imaging. 8 The most significant barriers between simulation and real-time images, however, are organ deformation and position changes. In our navigation system, we did not include position changes caused by breathing or the pyelocaliceal intraoperative deformation (expansion and contraction) caused during saline irrigation. We are currently developing a simulation program for overcoming these problems.
Expert surgeons are generally able to perform better maneuvers because of their experience. Losing their orientation during ureteroscopy, however, sometimes still occurs because of macrohematuria and the complexity of the pyelocaliceal system. Therefore, the navigation system for RIRS could help a wide range of experienced surgeons to perform exact and effectual maneuvers. Although fluoroscopic guidance would be necessary to put on the guidewires and ureteral stent, our system has the potential to reduce radiation exposure by showing a 3D real-time position of the ureteroscope.
Conclusion
Use of our novel ureteroscopic navigation system improved AR, T, sFT, and ML of ureteroscopic maneuvers among surgeons with a wide range of experiences. Our system has the potential to reduce radiation exposure by showing surgeons the real-time position of the tip of the ureteroscope on the 3D navigation image. For the clinical application of this system in future, however, we need to overcome the problems of registration of the ureteroscope, respiratory movement of the kidney, and expansion and deformation of the pyelocaliceal system by irrigation.
Footnotes
Author Disclosure Statement
No competing financial interests exist.