
Abstract
Purpose:
To describe our approach for port placement and robot docking for pelvic and kidney surgery (KS).
Patients and Methods:
We use a four-arm robotic approach and a 5 to 6 port placement consisting of: One 12-mm camera port, three 8-mm robotic ports, and one to two assistant ports. For radical prostatectomy, the working robotic ports run parallel below the level of the umbilicus. Radical cystectomy ports are more cephalad and above the level of the umbilicus. For transperitoneal KS, two bariatric robotic ports are used, aiming for an equilateral triangle configuration. With retroperitoneal (RN) KS, a balloon dilator and balloon port create the RN space; bariatric ports comprise the most anterior and posterior ports.
Results:
This technique has been used since 2010 on more than 2370 robotic urologic cases. To date, no procedure has needed patient or robot positioning while maintaining fourth arm functionality with minimal robotic arm clashing.
Conclusions:
Our approach of port placement and robot docking is reproducible and feasible for pelvic surgical procedures and KS.
Introduction
L
Technique
At our institution, a four-arm approach is routine for urologic robotic cases. Table 1 depicts the advantages and disadvantages of using four arms over three arms.
Port placement for pelvic surgery
Port placement for radical prostatectomy
We have previously reported on our port placement for robot-assisted radical prostatectomy (RARP) procedures. 1,2 The patient is placed in a steep Trendelenburg position in the dorsal lithotomy position. Once this is achieved, we then use a five- to six-port robotic approach with the fourth arm on the right side of the patient and the assistant port on the left (Fig. 1).
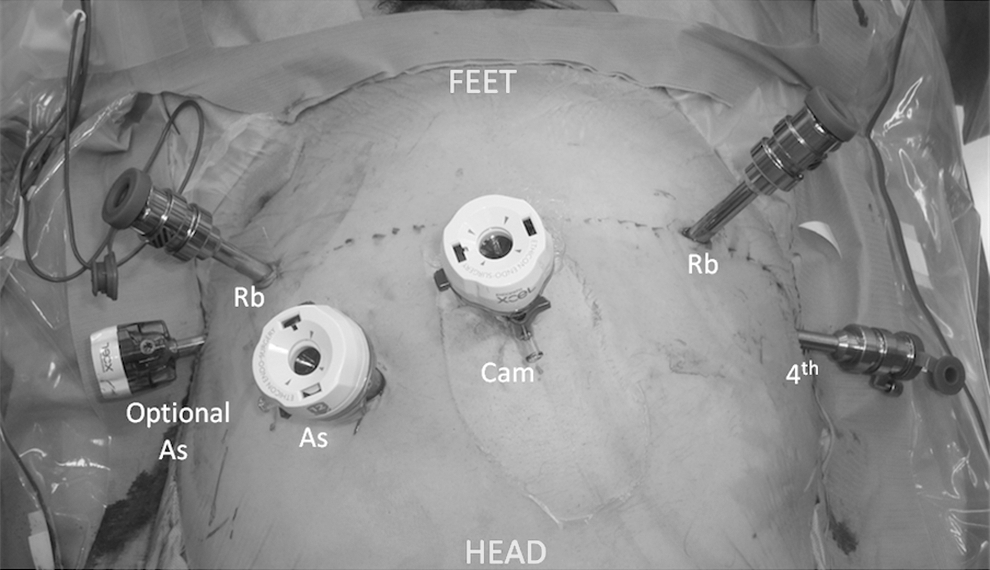
Port placement for robot-assisted radical prostatectomy. Operative representation. As=assistant port; Rb=robotic port; Cam=camera; 4th=fourth arm.
The port placement consists of: –Four robotic ports • 1: 12-mm port—camera • 3: 8-mm ports—fourth arm, right arm, and left robotic arm –One-two assistant ports • 1: 12-mm port • 1: 5-mm port (optional)
Two robotic ports are placed on the right side of the umbilicus, four fingerbreadths (one fingerbreadth ∼1.9 cm) apart from each other, and one robotic port is placed on the left side, five fingerbreadths from the midline. The 12-mm assistant port is located four fingerbreadths superior to the camera port and halfway in between the camera port and the left robotic arm. The camera port is placed supraumbilical, about 1.5 cm above the umbilical scar. The robotic ports are also placed on a parallel plane slightly below the umbilicus. The 5-mm assistant port is placed to the left of the left robotic port; it is optional and can be used for more difficult cases.
With this configuration, the body habitus of the patient does not become a concern and/or need different port locations. If the surgeon is concerned that the instrument may not be able to reach certain parts of the body, the ports can simply be pushed in if needed using our technique.
Port placement for radical cystectomy
The gold standard of care for muscle-invasive and refractory nonmuscle-invasive bladder cancer is radical cystectomy. 3 Like other robotic surgical procedures, robot-assisted radical cystectomy (RARC) is gaining in popularity. Studies conducted in the United States have demonstrated that the proportion of RARCs has consistently increased from 2004 to 2010. 4,5 We have reported previously on our technique for RRC. 6
Our port placement for RARC is similar to RARP, with a few differences (Fig. 2). The port placement consists of:
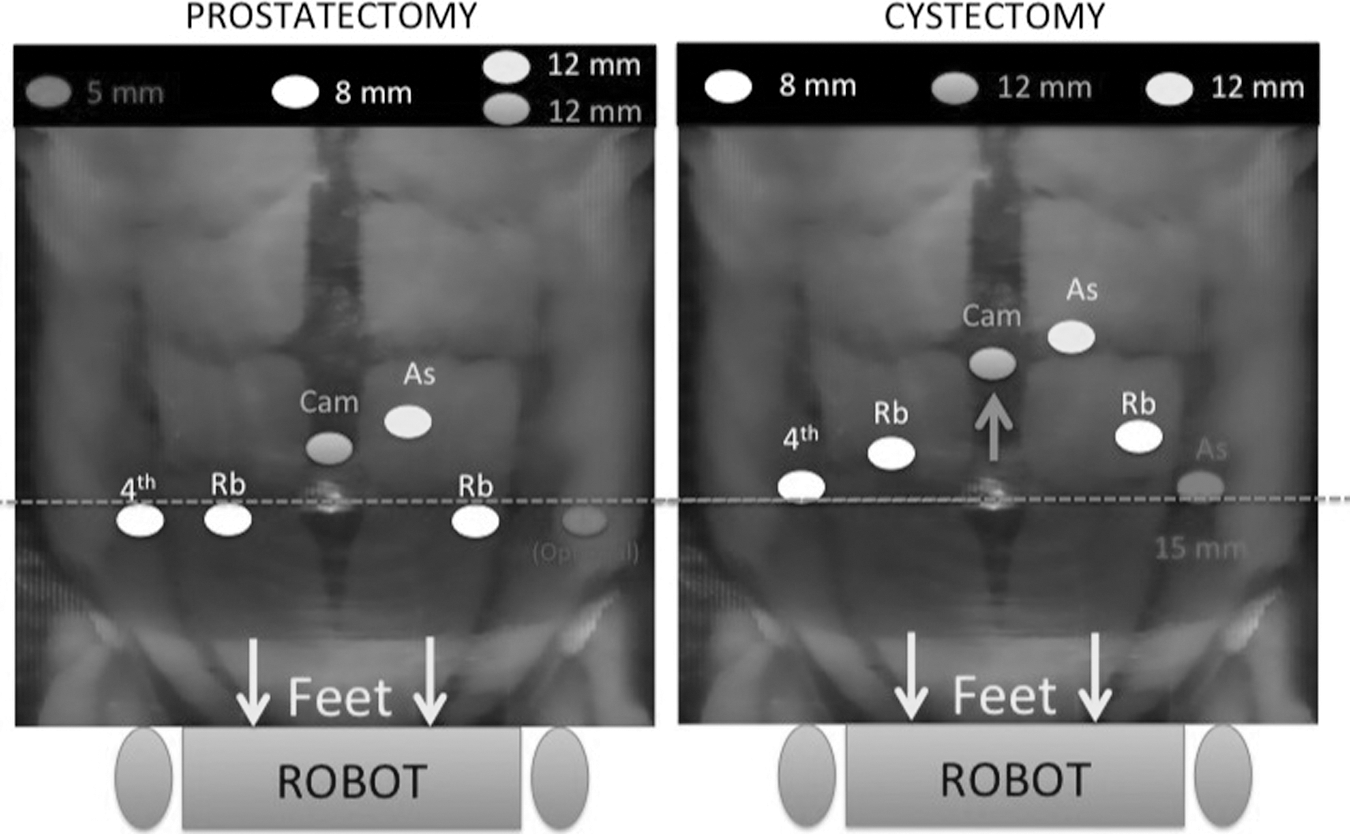
Port placement comparison for robot-assisted radical cystectomy.
–Four robotic ports
• 1: 12-mm port—camera
• 3: 8-mm ports—fourth arm, right arm, and left robotic arm
–Two assistant ports
• 1: 12-mm port
• 1: 15-mm port
The patient is placed in the Trendelenburg position in the dorsal lithotomy position. In comparison with RARP, the port placement is considerably more cephalad for RARC; this is attributed mostly to the additional reach needed during proximal lymph node dissection and ureteral mobilization during neobladder diversion. The camera port is placed five fingerbreadths above the umbilicus while the working robotic ports are placed two fingerbreadths above the level of the umbilicus. The 15-mm assistant port is placed slightly more caudal and lateral; this positioning allows for improved angulation during stapling of the bowel reconstruction. The 15-mm port is used to pass the 15-mm Endocatch bag as well. In males, the specimen is retracted through the 15-mm port and in females, if possible, the specimen is extracted via the vagina.
Port placement for kidney surgery
Transperitoneal approach
One benefit to our port placement for robot-assisted transperitoneal renal surgery is that this configuration can be used when treating patients with renal tumors that are located in the upper pole, hilar region, and lower pole. We once again use a four-arm approach with one to two assistant ports (Fig. 3A, 3B). For our renal robotic surgical procedures, we use 8-mm bariatric robotic ports that are placed at the costal margin and just slightly cephalad and lateral to the pubic bone (just lateral to the medial umbilical ligament). An 8-mm traditional robotic port is placed two fingerbreadths above the anterior superior iliac spine. The camera port is placed on the same level as the 12th rib just lateral to the pararectus line, and the assistant ports are placed in their traditional locations (i.e., one assistant port is placed between the camera port and the upper most robotic arm, and the other is placed in between the camera and the lower robotic arm, both of which are placed slightly more medial than the other ports).
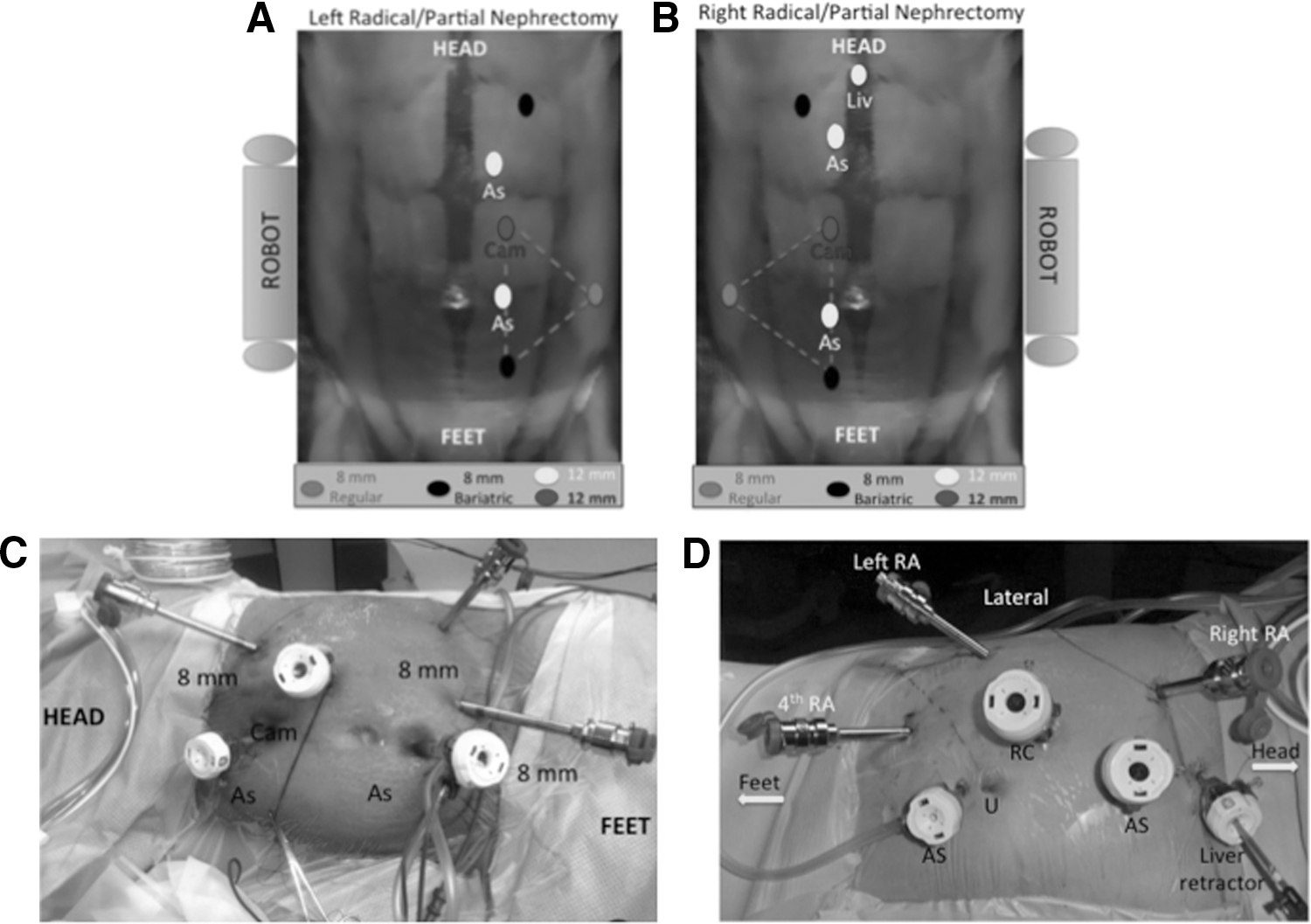
Port placement for robotic kidney surgery. (
To minimize instrument clashing, we aim for an equilateral triangle between the camera port, the lower bariatric port, and the lateral regular robotic port. For right renal surgery (Fig. 3B), the port placement is similar with the addition of the liver retractor port, which is placed at the xiphoid sternum. This configuration allows for optimal use of the four robotic arms while minimizing intraperitoneal instrument clashing and exterior robotic arm clashing. In this configuration, the lower bariatric port is the most “active” arm, regardless of dexterity. If a mass is located within the upper pole of the kidney, the reach may be considered a problem. Because this port is bariatric and thus longer, however, the port can simply be pushed in to ensure the surgeon can reach the upper pole location. For specimen retrieval, the more caudal assistant port is typically used, although it varies by patient.
Retroperitoneal approach
The retroperitoneal approach for robotic kidney surgical procedures is less popular than the transperitoneal approach. There is minimal literature discussing a four-arm approach for retroperitoneal kidney surgery. 7,8 At our institution, while we also use a four-arm approach, our port placement is vastly different from the transperitoneal approach. The patient is positioned in full flank (lateral decubitus) position. The table is flexed to allow maximal separation between the costal margin and iliac crest. We use a balloon dilator (either kidney or regular shaped) and a temporary balloon port to access the retroperitoneum and create the retroperitoneal space.
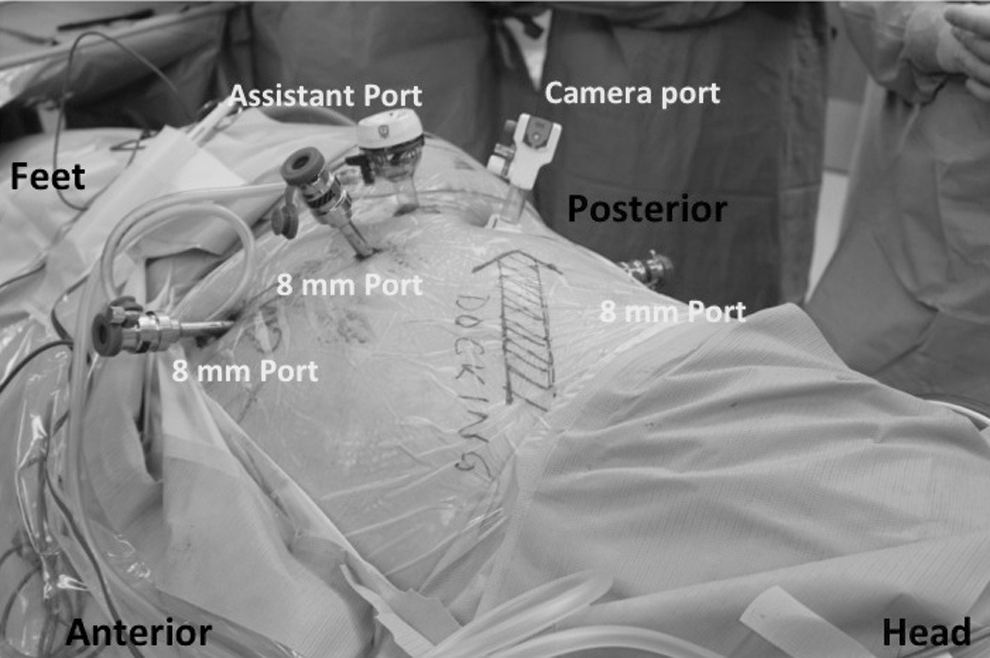
The 12-mm camera port is placed in the midaxillary line between the costal margin and iliac crest. The 8-mm robotic ports are placed under direct visualization. The most posterior and medial ports are placed in the posterior axillary line and the anterior axillary line, which are respectively parallel to the camera port (Fig. 4A). To minimize arm clashing, bariatric robotic ports are used for the most anterior and posterior ports (Fig. 4B). The fourth arm is in the most anterior port position, and the assistant is positioned behind the patient's back.

Port placement for robotic retroperitoneal kidney surgery. (
Robot docking
Because we use the additional robotic arm, it is imperative to dock the robot and position the arms in the most optimal positioning possible to minimize exterior arm clashing. The robotic arms should be positioned to maximize the “sweet spot” (Fig. 5), the maximum angle possible to help prevent clashing of the robotic arms during the procedure. During RARP and RARC, the robot approaches the patient in a straight line at the foot of the table. During transperitoneal renal surgery, the robot is docked on the contralateral side to the kidney undergoing the procedure (i.e., for a left partial nephrectomy, the robot is docked on the right side of the patient). In retroperitoneal renal surgical procedures, however, the robot comes in from the anterior aspect of the patient's abdomen and from over the patient's shoulder (Fig. 6).

Robot docking. Optimal arm placement for robotic arms.
Robot docking placement for retroperitoneal kidney surgery.
Equipment
• da Vinci SI robotic system (Intuitive Surgical, Sunnyvale, CA)
• 12-mm camera port
• 8-mm port
• 12-mm assistant port
• 15-mm assistant port
• 5-mm assistant port (optional)
• 8-mm bariatric ports (2)
• Hernia/kidney-shaped balloon (OMSPDBS2, Covidien, Mansfield, MA)
Role in Urologic Practice
Results
Our approach for port placement and robot docking has been used consistently since 2010 on more than 2370 robot-assisted urologic cases. To date, no procedure necessitated patient or robot repositioning. All procedures maintained fourth arm functionality with minimal robotic arm clashing.
Discussion
The use of robotics is quickly gaining acceptance as the standard of care for many intra-abdominal procedures in urology. It is becoming more imperative that optimal port placement and robot docking be used to allow for the maximum benefits of using a robot. There have been reports demonstrating unique port placements for specific and difficult procedures or for children. 9,10 It is beneficial, however, that newly trained urologists and the novice urologic surgeons understand a more generalized approach and technique for port placement and robot docking. These factors can play a significant role in providing the best treatment for their patients. Providing a foundation of the best way to approach pelvic and kidney robotic surgical procedures in adults will allow physicians to improve treatment and allow for them to improve patient care.
We have consistently used our port placement and robot docking approach on more than 2300 robot-assisted urology cases to date. In our experience, this configuration allows for the most optimal use of the four robotic arms and ample space for the procedure. In our port placement for pelvic surgery, we have the fourth robotic arm on the right side. This is different from many robotic surgeons who have their fourth robotic arm on the left side of the abdomen. Our reason for this configuration is to place the assistant on the left side of the table. Most assistants are right-handed, and by having the assistant port on the left side, this allows for the assistant to be comfortable and provide quality care during the surgery.
In our configuration for right transperitoneal kidney surgery, we use a 5-mm assistant port for liver retraction. This port could be considered optional; as surgeons become more experienced, they may not find use for this port or this retractor. In our experience, however, we always create this port placement because we do not know before the surgery how the intra-abdominal anatomy will impact the surgery. Thus, this port is made in case we need assistance, which may not happen all the time. For upper pole tumors of the kidney, however, we frequently use the liver retractor to provide optimal exposure during the surgery.
There are many port placement configurations within the literature for transperitoneal renal surgery, both in peer-reviewed journals and textbooks. The quality of the port placement configuration is dependent on the surgeon—whichever technique he/she prefers and with which he/she is accustomed. Our technique is unique in that we use four robotic arms while a majority still use a three robotic arm configuration, as depicted by Rogers and associates. 11 This institution uses a three-arm robotic approach for kidney surgery and aims for a wide “V” configuration. In addition, the surgeons do not use bariatric ports.
In our technique, we are able to use the robot to its fullest, by using all of its arms. Furthermore, because of our four-arm approach, we aim for an equilateral triangle and not a wide “V”. Because we use bariatric ports, our configuration does not need to be changed because of the patient's body habitus, as it may with techniques that do not use bariatric ports.
Retroperitoneal kidney surgery is a technique that is starting to get used more frequently robotically. Two recent articles demonstrate the benefits of using this approach for a specific subset of patients and location of kidney tumors (posterior). Hu and colleagues 12 recently discussed their experience using a robotic three-arm technique, while Ghani and coworkers 8 provided step-by-step instructions for their three-arm retroperitoneal approach.
Our technique is different from both, because our method uses four robotic arms, while both experiences utilize only three arms. When compared with Ghani and colleagues, 8 the robot is docked directly over the patient's head parallel to the spine, while in our technique, the robot comes in from the anterior aspect of the patient's abdomen and from over the patient's shoulder. The only other study that demonstrates the use of four robotic arms for retroperitoneal partial nephrectomy was performed in 2012. 7 Their approach is very similar to ours; however, they do not discuss the docking of their robot. Our docking position allows for the trajectory of the camera port to be looking directly at the hilum.
Conclusion
Robotic surgery is increasing in popularity. It is paramount that port placement and robot docking are optimized for allowing the use of additional robotic arms to complete more technically complex surgical procedures while reducing robotic arm clashing externally and inside the operative field. A four-arm approach can be used successfully as long as the optimum robotic port placement and robot positioning is employed.
Disclosure Statement
No competing financial interests exist.