
Abstract
Purpose:
To develop a robotic technique for exclusively transabdominal control of the suprahepatic, infradiaphragmatic inferior vena cava (IVC) to enable level 3 IVC tumor thrombectomy.
Materials and Methods:
Robotic technique was developed in three fresh, perfused-model cadavers. Preoperatively, inflow (right jugular vein) and outflow (left femoral vein) cannulae were inserted and connected to a centrifugal pump to establish a 10 mmHg pressure in the IVC for the water-perfused cadaver model. Using a five-port transperitoneal robotic approach, the falciform ligament was detached from the anterior abdominal wall toward its junction with the diaphragm and tautly retracted caudally; this adequately retracted the liver caudally as well. Triangular and coronary ligaments were incised, allowing ready visualization of suprahepatic/infradiaphragmatic IVC and right/left main hepatic veins. Under direct robotic visualization, IVC was circumferentially mobilized, vessel-looped, and controlled.
Results:
All three robotic procedures were successfully completed transabdominally. Average robotic time to control the suprahepatic IVC was 37 minutes; in each case, the suprahepatic IVC was circumferentially controlled with a vessel-loop. There were no intraoperative complications. Length of the mobilized suprahepatic IVC measured between 2 and 3 cm. Right and left suprahepatic veins were clearly visualized in each case. Necropsy revealed no intra-abdominal/intrathoracic visceral or vascular injuries to the suprahepatic IVC, bilateral hepatic veins, or tributaries.
Conclusions:
We developed a novel robotic technique for transabdominal control of the suprahepatic infradiaphragmatic IVC in a perfused human cadaver model. This approach may extend the application of advanced robotic techniques for the performance of major vena caval, hepatic, and level 3 IVC renal tumor thrombus surgery.
Introduction
R
Minimally invasive surgery for caval thrombi, performed in a completely intracorporeal manner, has evolved gradually over the past 15 years. Experimentally, laparoscopic techniques for level 2 and level 3/4 caval thrombus were initially developed in our laboratory in the early 2000s. 2,3 Clinically, initial case reports of laparoscopic renal vein thrombectomy were followed by the initial series of laparoscopic renal vein thrombectomy and robotic level 1–2 caval thrombectomy. 4 –7
Building on this, we reported the initial clinical experience with robot-assisted surgery for level 3 caval thrombus extending into the liver with successful control of the infrarenal IVC, renal, lumbar, and short hepatic veins, and intrahepatic IVC. 8 –10 Most recently, we reported the initial clinical case of completely minimally invasive (thoracoscopic) transthoracic control of the intrapericardial IVC for level 3 thrombus. 11
Currently, the only option for surgical removal of level 3 caval thrombus extending up to the confluence of the main hepatic veins is by major open operation. Typically, this has necessitated an abdominal bilateral subcostal (chevron) incision with midline sternotomy for transthoracic control of the IVC. Alternatively, a completely transabdominal open surgical approach can be used, wherein the coronal and triangular hepatic ligaments are incised and the right lobe of the liver reflected to the left side; this allows access to the suprahepatic infradiaphragmatic IVC, which can then be controlled transabdominally.
No minimally invasive alternative to this open approach of completely transabdominal IVC control is currently available, however. In other words, a robotic technique to transabdominally control the suprahepatic, infradiaphragmatic IVC currently does not exist.
We performed a focused study to assess the feasibility of, and describe the step-by-step technique for, robotic transabdominal control of the suprahepatic infradiaphragmatic IVC to facilitate level 3 caval thrombectomy in a perfused-cadaver model.
Materials and Methods
Perfused-cadaver model
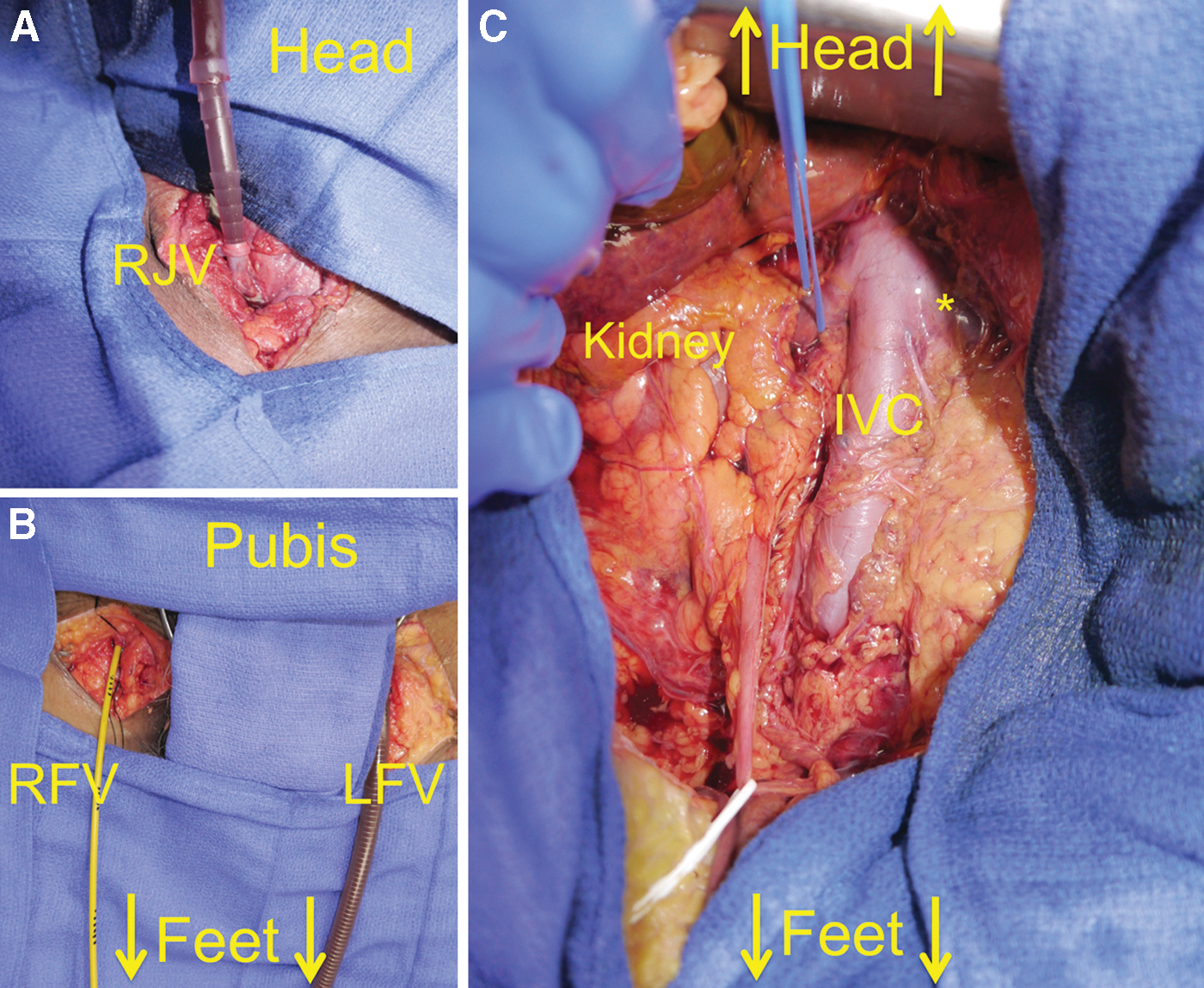
This study was conducted according to university protocol requirements for fresh tissue human cadavers. One fresh male cadaver was used to create the perfused cadaver model, as follows: The right jugular vein (as inflow channel), as well as the left femoral vein (as outflow channel) were cannulated and connected to a centrifugal pump (Bio-Pump® BP-80, Medtronic, Minneapolis, MN). The pressure in the IVC was set up for 10 mm Hg and was measured using a datascope monitor (Datascope Passport monitor
(
Surgical technique
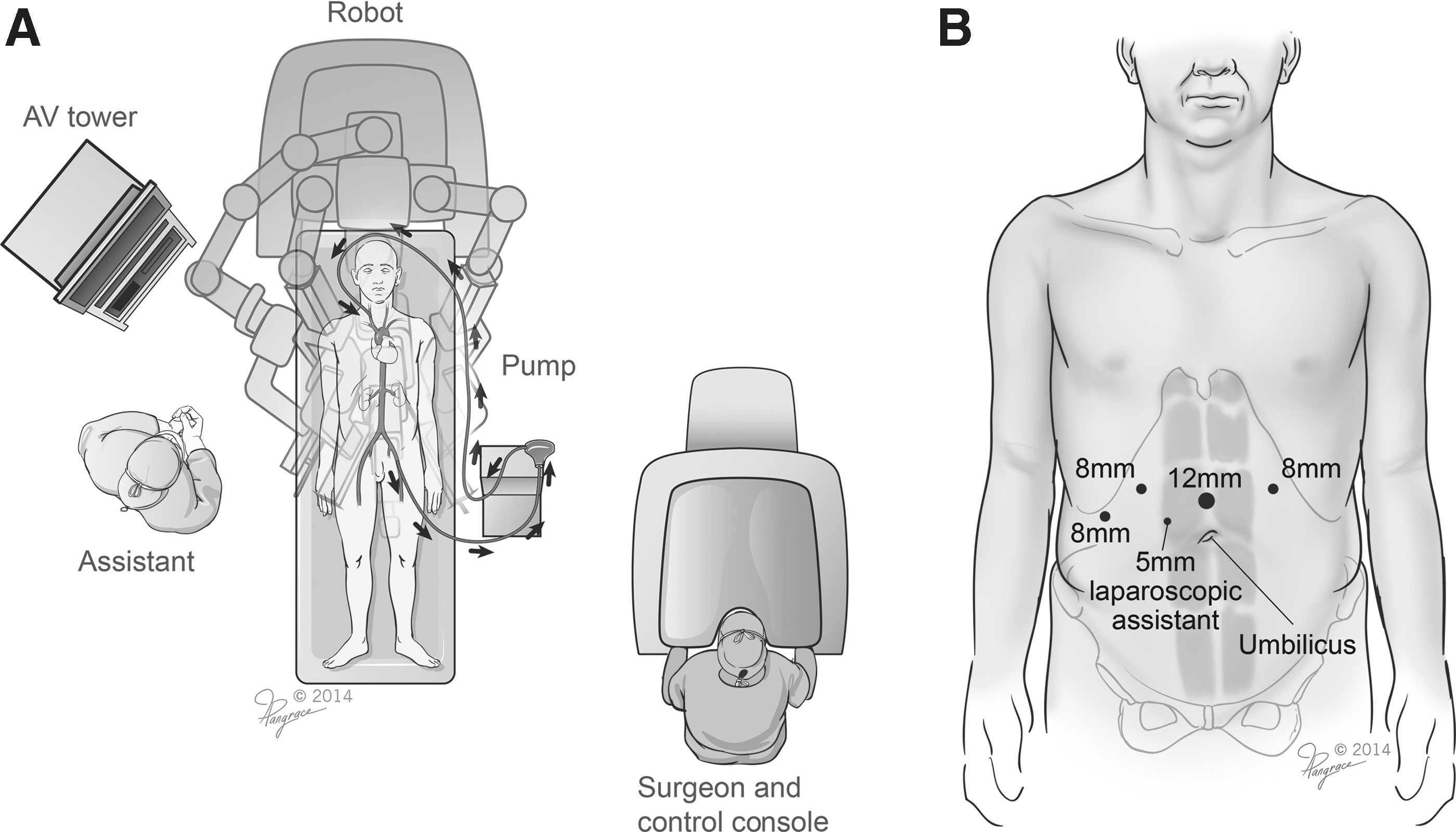
The cadaver was placed in the supine decubitus position, a 15-mm Hg CO2 pneumoperitoneum was established, and five ports were inserted transperitoneally similar to robotic esophagectomy. A slight reverse Trendelenburg position was obtained, and the robot (da Vinci Si Surgical System, Intuitive Surgical, Sunnyvale, CA) was docked over the cadaver's head (Fig. 2).
(
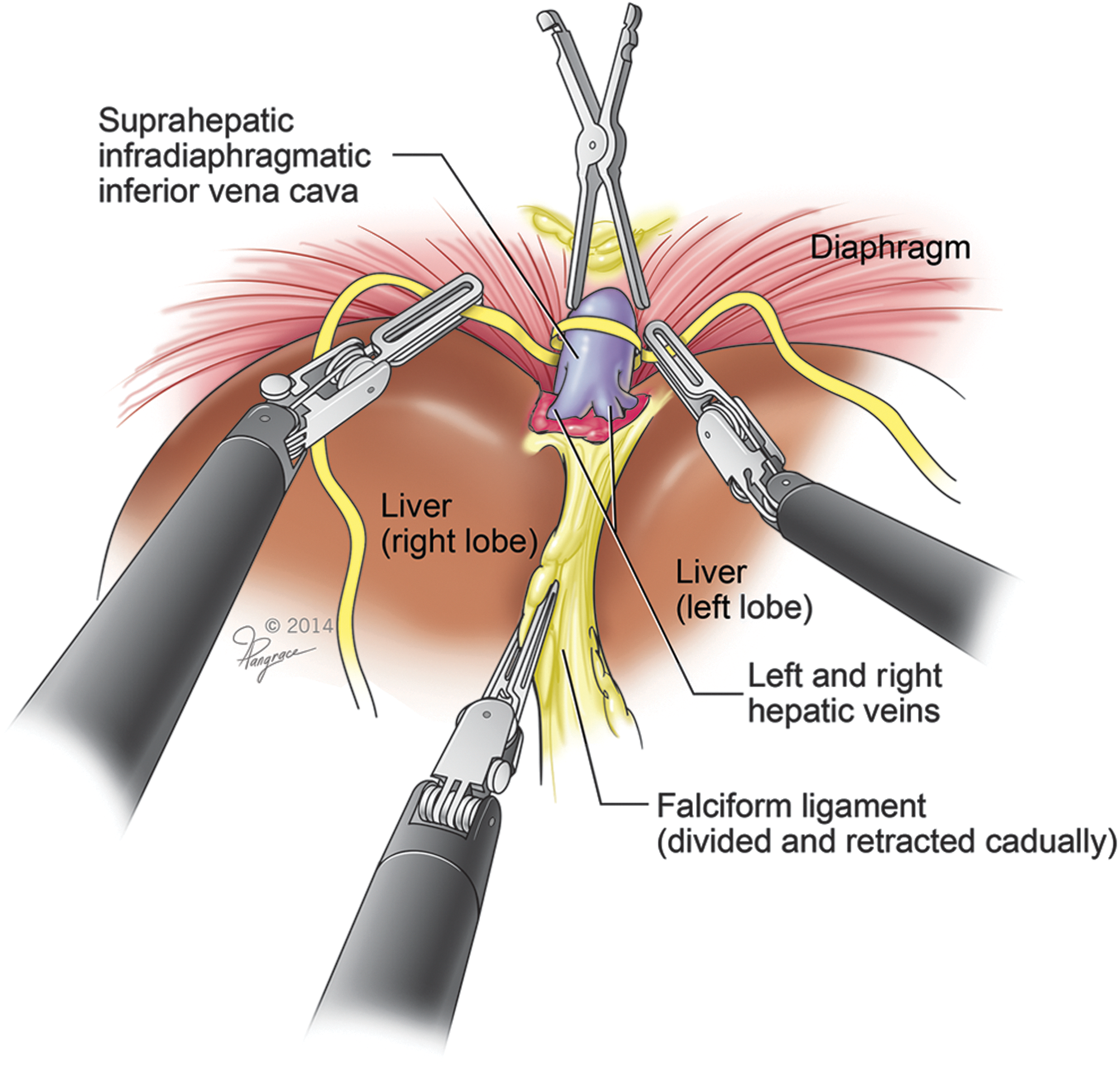
The procedure began by identifying and incising the hepatic round ligament. The falciform ligament was then incised immediately alongside the undersurface of the anterior abdominal wall and carried cephalad toward its junction with the diaphragm. The fourth robotic arm was used to grasp and tautly retract the falciform ligament caudally, which resulted in both lobes of the liver being retracted caudally as well. The triangular and coronary hepatic ligaments were incised, which allowed identification of the right and left suprahepatic veins and IVC (Fig. 3). The right diaphragmatic pillar was dissected laterally, paying attention to avoid injury to any diaphragmatic veins. At this point, the anterior surface of the IVC was exposed.

(
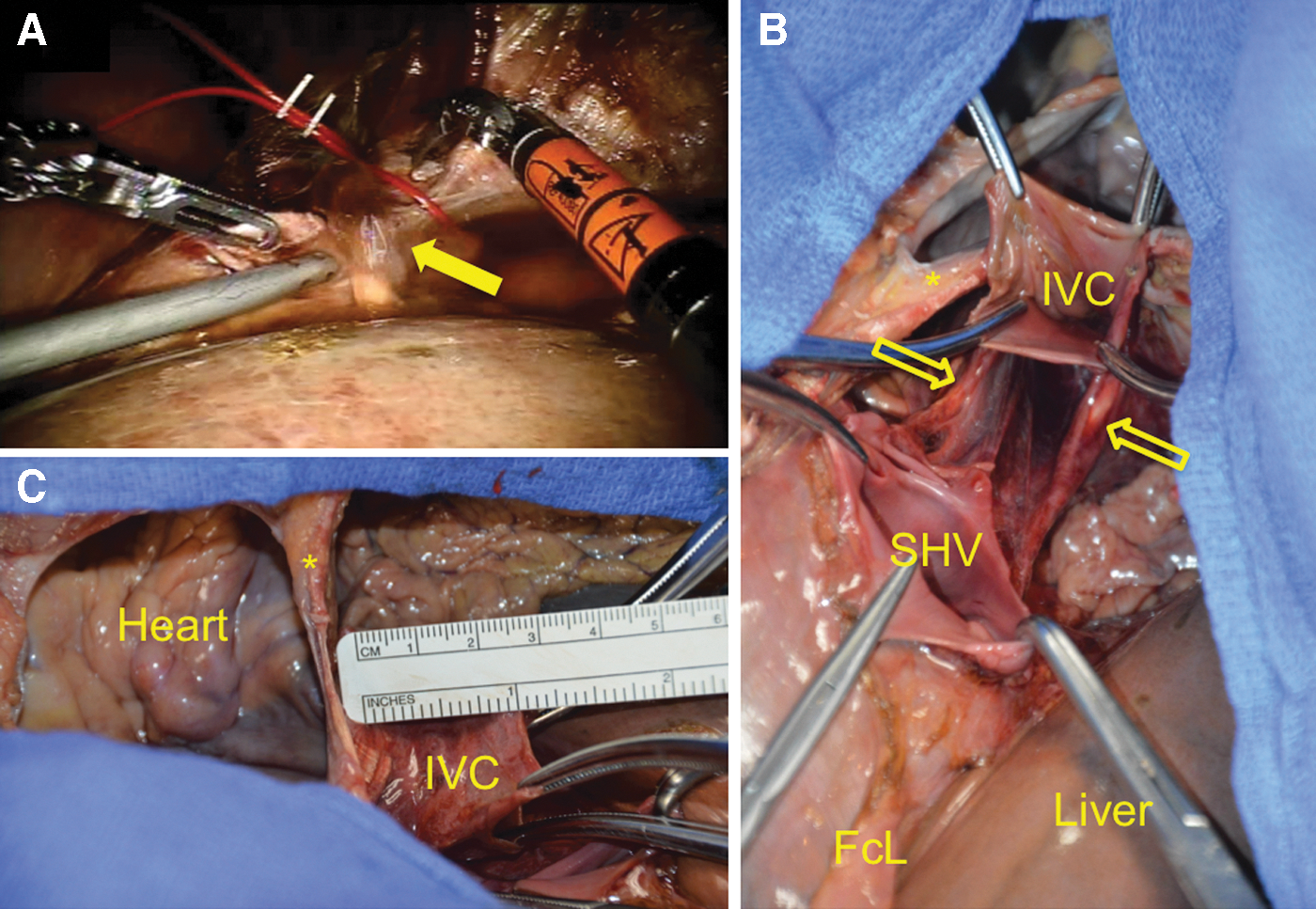
Careful bilateral and posterior dissection of the IVC was performed under direct robotic visualization, resulting in a left-to-right circumferential dissection of the IVC. The suprahepatic IVC was then vessel-looped and controlled (Fig. 4).
Final aspect of suprahepatic, infradiaphragmatic inferior vena cava control.
Necropsy
During necropsy, the thoracic cavity, liver, diaphragm, suprahepatic IVC, right and left supra-hepatic veins, spleen, and bowel were carefully examined. Measurements of the suprahepatic IVC were obtained.
Results
All robotic procedures were completed successfully with surgical times of 45, 35, and 30 minutes, respectively. Intraoperative complications or conversion to open surgery did not occur in any case. On completion of the robotic procedure, we intentionally created a cavotomy in the anterior wall of the suprahepatic IVC using robotic scissors. Immediate voluminous efflux of the circulating perfusate fluid confirmed two findings: (a) Continuous perfusion of the cadaver was adequately maintained throughout the robotic procedure by the centrifugal pump, and (b) because no leakage of perfusate was noted during the suprahepatic dissection, this further validated that no iatrogenic vascular injury had occurred to the suprahepatic IVC, bilateral hepatic veins, or their tributaries during robotic dissection.
During in situ necropsy, no injuries were found to any organs including bowel, liver, diaphragm, heart, lungs, nor was there any intrathoracic violation (Fig. 5). In all cases, the IVC was completely dissected circumferentially (vessel-looped), and there was no injury to its posterior wall. The mobilized infradiaphragmatic suprahepatic IVC measured between 2 and 3 cm in length and approximately 2.5 cm in diameter. Right and left suprahepatic veins were clearly visualized in all three cases.
(
Discussion
During surgical excision, the specific intraoperative maneuvers are dictated by thrombus level. Renal vein thrombus (level 0) can typically be milked back toward the kidney followed by vascular stapling at the renal vein-IVC junction. Level 1 thrombus extending into the IVC necessitates either partial circumference Satinsky clamping of the IVC for vascular control or limited complete IVC control. Level 2 thrombus necessitates complete, circumferential IVC control, including lumbar vein ligation, infrarenal IVC control below the thrombus, contralateral renal vein control, and suprarenal IVC control above the thrombus, without the need to control the short hepatic veins. Level 3 thrombus necessitates additional maneuvers, including ligation of various short hepatic veins with mobilization and control of the intrahepatic IVC; in some cases, control of the porta hepatis, the suprahepatic IVC, or the intrapericardial IVC may be needed. 8
Management of level 3 vena cava thrombi is a major surgical undertaking that has always been performed exclusively by open surgery. For high intrahepatic level 3 thrombi approaching the hepatic venous confluence, careful and reliable control of the suprahepatic IVC is necessary in addition to securing the inflow channels into the infra/intrahepatic IVC. Typically, a large incision (bilateral subcostal [chevron], midline abdominal or thoracoabdominal) is necessary, often combining urologic and cardiothoracic surgical teams. The attendant postoperative morbidity is not inconsiderable. 1
We, and others, have carefully developed minimally invasive IVC tumor thrombectomy in a stepwise manner. 2 –9 Clinically, robot-assisted thrombectomy for level 1 and 2 thrombi has been performed. 4,6,8 Recently, the initial experience with robotic level 3 IVC thrombectomy has been described, wherein the thrombus extends intrahepatically cephalad to the short hepatic veins. 8 –10,12 Most recently, we published the initial description of completely thoracoscopic control of the supradiaphragmatic IVC in a patient with level 3 IVC thrombus up to the diaphragm, 11 wherein control of the porta hepatis was also achieved minimally invasively. This necessitated two teams of surgeons working in conjunction during the operation.
The goal of the current study was specifically focused on determining the technical feasibility of controlling the suprahepatic infradiaphragmatic IVC robotically by a completely transabdominal approach in the perfused fresh cadaver model. If indeed successful, it could eliminate the need for a large incision or for entering the thoracic cavity, potentially decreasing postoperative morbidity. From an anatomic perspective, we documented that there is a 2 to 3 cm length of suprahepatic infradiaphragmatic IVC that can be robotically accessed transabdominally. Achieving control of the suprahepatic IVC necessitated an average operative time of 37 minutes, and there were no vascular injuries.
Control of the porta hepatis, infrarenal IVC, contralateral renal vein, and lumbar veins must also be achieved to fully exclude the tumor thrombus-bearing IVC segment. We intentionally did not perform any of these infrahepatic maneuvers in this experiment, because we already achieved these maneuvers clinically in patients using an exclusively robotic/laparoscopic approach. 8,9,12 Furthermore, prolonged perfusion in the cadaver causes tissue edema and extravasation of perfusate in the bowel and in intra-/retroperitoneal tissues, resulting in reduced operating space and compromised laparoscopic exposure and visualization, precluding a minimally invasive approach. As such, we addressed only the suprahepatic IVC segment of interest.
The flow of perfusate through the IVC can be set for both directions, either proximal-to-distal or distal-to-proximal. We established proximal-to-distal jugular-to-iliac venous perfusion flow because doing so allowed use of a larger caliber cannula in the iliac vein, thus simulating low-pressure IVC flow. Such low-pressure flow adequately simulated bleeding in case of venous or IVC injury.
Our study has limitations. Completely robotic high level 3 IVC tumor thrombectomy in the clinical scenario would necessitate sequential control of infrarenal IVC, its major feeding veins (lumbar, bilateral renal, right adrenal), short hepatic veins, and porta hepatis, before transabdominally controlling the suprahepatic IVC. As discussed above, we focused solely on the hitherto unanswered question of whether the suprahepatic IVC can be accessed and controlled transabdominally by a purely robotic approach. Thus, our study is unable to comment on the need for patient repositioning, robot redocking, and location of additional ports for the infrahepatic part of the operation, issues that are pertinent for this procedure. It is noteworthy that the newly available da Vinci Xi robotic platform (Intuitive Surgical) may eliminate the need for robot repositioning and redocking.
Also, the perfused cadaver model is not without limitations. The liver may have been suboptimally perfused, which may have made hepatic retraction easier in the cadaver model than it may be clinically, with the potential for a smaller suprahepatic working space. Also, the perfused cadaver model lacked cardiac contractions and diaphragmatic respiratory movements, which could make the clinical procedure more challenging. Nevertheless, we think the perfused cadaver model is currently the most realistic model that allows us to test the feasibility of this procedure using human anatomy before advancing to clinical application.
Conclusions
Robotic transabdominal control of the suprahepatic, infradiaphragmatic inferior vena cava appears feasible in the human. This may have implications in advancing the field of robotic surgery for major upper abdominal applications such as IVC surgery, hepatic surgery, and level 3 vena cava tumor thrombus surgery, all performed in a completely intracorporeal manner.
Footnotes
Author Disclosure Statement
No competing financial interests exist.