
Abstract
Background and Purpose:
Routine imaging following ureteroscopy for treatment of renal/ureteral calculi continues to be a topic of debate. However, with the increasing focus on healthcare costs and quality, judicious use of diagnostic imaging to optimize outcomes while minimizing resource utilization is a priority. We sought to identify post-ureteroscopy imaging practices among experienced urologists.
Materials and Methods:
A REDcap questionnaire was sent to urologists in North America. The questionnaire surveyed demographic data, clinical volume, and imaging preferences post-ureteroscopy. Additionally, we surveyed the extent to which stone, anatomic, and procedure-related factors influenced these preferences. The likelihood of altering clinical practice and the desire for specific imaging guidelines were also assessed. The interquartile range (IQR) was utilized as a measure of median consensus.
Results:
Three hundred twenty-two urologists completed the questionnaire. The mean number of years in practice was 18±10; 82% of respondents performed more than five ureteroscopic stone procedures monthly. Routine postoperative imaging was obtained by 48% of participants as follows: ultrasound (US) (47%), kidneys, ureters, and bladder (KUB) (17%), CT (4%), intravenous pyelogram (IVP) (2%), and KUB+US (30%). Urologists who did not routinely image patients were more concerned about cost (55% vs 25%, p≤0.0001), radiation exposure (69% vs 44%, p≤0.0001), and diagnostic inaccuracy of US (57% vs 44%, p≤0.02). These urologists were also less likely to have completed an endourology fellowship (7% vs 23%, p≤0.0001). The most compelling predictors of obtaining postoperative imaging were postoperative pain and fever (median 5, IQR 1), residual stones (median 5, IQR 1), ureteral perforation (median 5, IQR 2), and presence of a solitary kidney (median 4.5, IQR 2).
Conclusions:
Currently, about 50% of urologists who regularly perform ureteroscopic stone procedures obtain postoperative imaging. Imaging preferences were guided by the presence of residual fragments, ureteral perforation, solitary kidney, and postoperative pain or fever.
Introduction
U
Materials and Methods
REDCap™ was used to create and administer a web-based survey, which was sent to 3130 urologists in North America (see Supplementary Data S1). The questionnaire surveyed demographic data: years of experience, completion of an endourology fellowship, location and type of practice, and the monthly clinical volume of ureteroscopies. The modality and timing of postoperative imaging in asymptomatic patients was also addressed. Finally, we surveyed the extent to which stone, anatomic, and procedure-related factors influenced physician preferences for imaging. The survey was sent out twice, 2 weeks apart. REDCap was used to collect and tabulate the anonymous responses. The median and interquartile range (IQR) were utilized for descriptive statistics. The IQR was utilized as a measure of median consensus, with a lower IQR denoting increased agreement. Statistical analysis was performed using standard computer software: JMP™ with the chi-square and Wilcox signed-rank tests with p<0.05 were considered statistically significant.
Results
Three hundred twenty-two urologists (10.3%) completed the questionnaire. The baseline characteristics of survey respondents are shown in Table 1. The mean number of years in practice was 18±10 years. The majority of respondents practiced in the United States or Canada (92% vs 7%, respectively). Of the respondents, 71% were in private practice while 27% worked in an academic setting. Fifteen percent of respondents completed a fellowship in endourology.
VA=Veterans Affair; URS=ureteroscopy.
Eighty-two percent of respondents performed at least five ureteroscopic stone procedures monthly. Forty-three percent of respondents performed between 5 and 10 procedures monthly; 30% performed 10 and 20 procedures per month. Approximately 8.5% of respondents performed more than 20 ureteroscopic stone procedures every month.
Regarding post-ureteroscopic imaging, 48% of respondents obtain routine postoperative imaging (Table 2). Among these, the imaging modality of choice is as follows: US (47%), KUB and US (30%), KUB (17%), CT (4%) and IVP (2%). The majority of those who obtained imaging did so between 1 and 3 months after the procedure (52%) while 39% obtained imaging within 1 month. A minority of urologists would wait till 3–6 months to re-image (8%), or beyond 6 months (1%).
IVP=intravenous pyelogram; KUB=kidneys, ureters, and bladder; US, ultrasound.
As shown in Table 3, the most compelling predictors of obtaining postoperative imaging in both groups were postoperative pain and fever (median 5, IQR 1), residual stones (median 5, IQR 1), ureteral perforation (median 5, IQR 2), and presence of a solitary kidney (median 4.5, IQR 2). Other significant predictors of postoperative imaging included recurrent stone formers, and anatomic factors such as UPJ obstruction, and ectopic kidney (median 4, IQR 2) (Fig. 1). Urologists generally agreed that the HU (median 1, IQR 1), distal ureteral stones (median 2, IQR 2), access sheath usage (median 2, IQR 2), CKD (median 2, IQR 2), and obesity (median 2, IQR 2) were not important in determining the need for postoperative imaging.
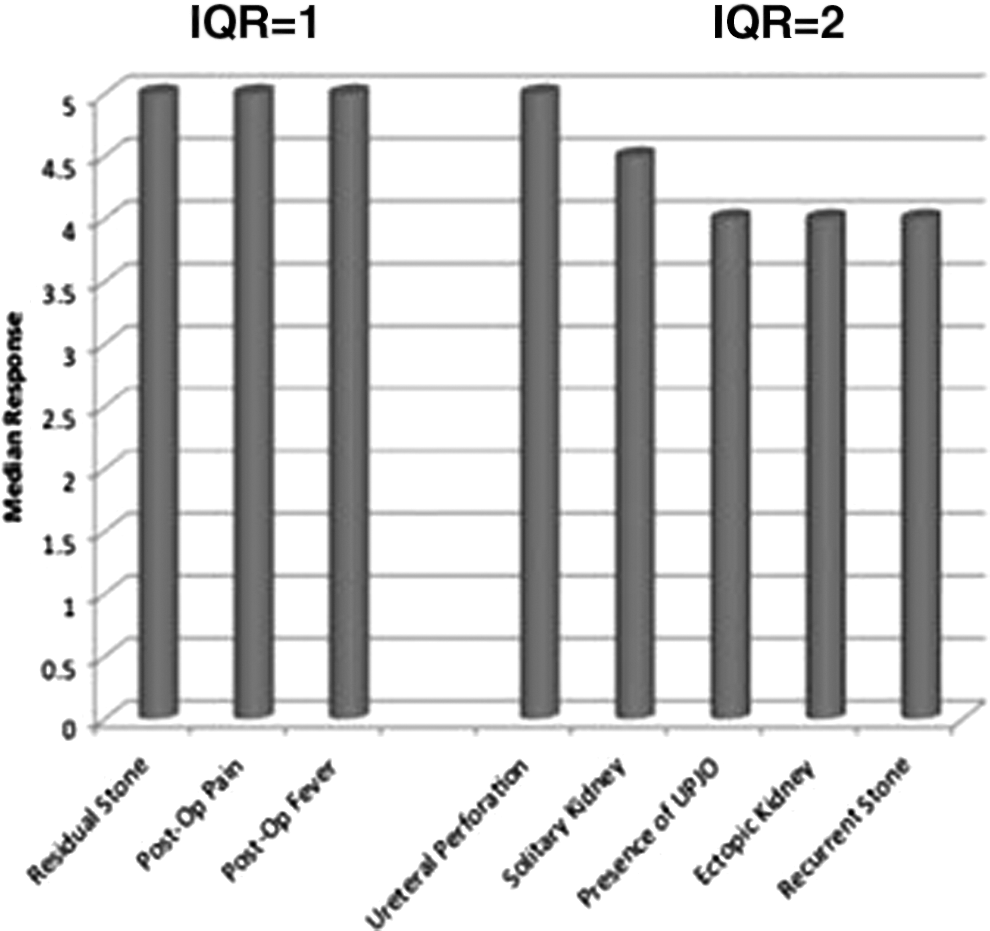
Relevant predictors of obtaining postoperative imaging. IQR=interquartile range; UPJO=ureteropelvic junction obstruction.
IQR is a measure of consensus with lower values denoting agreement among respondents and higher value denoting lack of consensus.
IQR=interquartile range; HU=Hounsfield units; UPJ=ureteropelvic junction; CKD=Chronic Kidney Disease.
Urologists who did not obtain routine postoperative imaging were significantly less worried about obstruction/hydronephrosis (p≤0.0036), distal ureteral stone fragment (p≤0.0001), balloon dilatation (p≤0.0001), stentless procedure (p≤0.0001), and use of an access sheath (p≤0.0001), compared to urologists who routinely imaged patients, who appeared to be more concerned with these issues, thereby prompting the use of imaging.
Table 4 shows the relative weight of specific factors that may impact the decision to obtain postoperative imaging between those who obtain routine imaging and those who don't. Urologists who do not routinely image patients were comparatively more concerned about cost (55% vs 25%, p≤0.0001, respectively), radiation exposure (69% vs 44%, p≤0.0001), and the accuracy of US (57% vs 44%, p≤0.0192) compared to those who routinely imaged patients. Those who did not obtain imaging routinely were also less likely to have completed an endourology fellowship (7% vs 23%, p≤0.0001).
Discussion
Ureteroscopy has an increasing role in the treatment of urinary calculi. 10,11 Despite the rarity of ureteral strictures with modern instrumentation, there may still be some bias to obtaining routine imaging after ureteroscopy. 12,13
As of now, imaging accounts for 16% of the total healthcare cost of each episode of ureteral calculi. The 2013 AUA Technology Assessment recommends US as the minimal imaging requirement following all cases of ureteroscopic stone procedures. 8 The panel contends that low cost of US and lack of ionizing radiation warrants routine utilization for the follow-up of patients treated for ureteral calculi. 8 This assessment however, does not recommend the optimal timeline for postoperative surveillance. Additionally, the assessment does not establish precise criteria targeting patients most likely to benefit from postoperative imaging.
In our study, most urologists agreed that postoperative pain, postoperative fever, residual fragments, and ureteral perforation were clear indications for postoperative imaging (median 5, IQR 1). Additionally, respondents agreed anatomic variants such as solitary kidney (median 4.5, IQR 2), UPJ obstruction (median 4, IQR 2), and ectopic kidney (median 4, IQR 2) justified follow-up imaging and our findings are generally consistent with the literature. 4,8,9,14
Beiko et al. 15 reviewed their experience with imaging following laser lithotripsy and concluded that imaging was only necessary in cases of significant ureteral trauma, stricture change, chronic impaction, preexisting renal impairment, and postoperative pain and fever. In a similar study, Karadag et al. 4 proposed proximal migration of stone fragments and presence of residual fragments on the first postoperative day should be additional indications for postoperative surveillance.
Adiyat et al. 9 retrospectively reviewed the effectiveness of selective imaging following ureteroscopy. Patients whom underwent complicated ureteroscopies involving mucosal perforation, balloon dilatation, chronic impaction, or postoperative pain following stent removal received imaging studies within 1 month. Otherwise, patients with uncomplicated procedures underwent imaging within 6–12 months. All cases of ureteral stricture occurred in patients with complicated procedures with an incidence equal 5.3% (3/56). The risk for postoperative hydronephrosis in the complicated URS cohort was 10.7% (6/56). No stricture developed in patients who underwent uncomplicated ureteroscopy, leading the authors to conclude that imaging can be performed selectively in patients with mucosal perforation, balloon dilation, chronic impaction, or persistent postoperative pain.
In contrast, Weizer et al. 16 recommended routine postoperative imaging to detect early silent obstruction. While postoperative pain was the only clinical factor significantly associated with postoperative obstruction, seven patients demonstrated obstruction in the absence of pain.
While the overall response rate of our study was 10.3% (322/3130), it is possible that endourologists may have been more inclined to participate. Further, urologists that perform ureteroscopy more frequently may be more definitive in their stance with respect to postoperative imaging. In our study, 48% of respondents routinely imaged patients following ureteroscopic stone procedures, primarily utilizing either US (47%) or a combination of US and plain film (30%). The consensus indications for postoperative imaging were fever, pain, residual stones, or ureteral perforation. Nonroutine imagers were significantly less concerned with obstruction or hydronephrosis, stone in distal ureter, balloon dilatation, stentless procedure, and the use of an access sheath. Urologists electing not to routinely image patients were significantly more concerned with cost, radiation exposure, and the accuracy of US. In our study, most urologists agreed that postoperative pain, postoperative fever, residual fragments, and ureteral perforation were clear indications for postoperative imaging after ureteroscopy. Many feel strongly that imaging is justified in asymptomatic patients with significant risk factors: residual fragments, solitary kidney, UPJ obstruction, and ectopic kidney. As these criteria are consistent with the literature, strict guidelines indicating the risk factors necessitating postoperative surveillance in asymptomatic patients along with appropriate timing intervals may decrease the costs associated with unnecessary imaging and optimize resource utilization for urinary stone disease. It is noteworthy that despite the AUAs clinical effectiveness protocol encouraging postoperative imaging for all ureteroscopy patients, only half of our responders complied. Accordingly, this emphasizes a need for clear evidence-based guidelines to best guide imaging practices; this was supported by 59% of the respondents, who were in favor of imaging guidelines for stones.
Conclusions
The controversy of imaging and stones persists—with almost an equal division of urologists who routinely obtain post-ureteroscopy imaging, and those who do not. Most urologists obtain imaging after ureteroscopy in instances of excessive postoperative pain, postoperative fever, known residual fragments, and ureteral perforation. To unify the approach to postoperative imaging, definitive guidelines specifying which asymptomatic patients require postoperative surveillance may significantly reduce unnecessary imaging.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.