
Abstract
The thulium fiber laser (TFL) is being explored as an alternative laser lithotripter to the standard holmium:yttrium-aluminum-garnet laser. The more uniform beam profile of the TFL enables higher power transmission through smaller fibers. In this study, a 100-μm core, 140-μm outer-diameter (OD) silica fiber with 5-mm length hollow steel tip was integrated with 1.3F (0.433-mm OD) nitinol wire basket to form a 1.9F (0.633-mm OD) device. TFL energy of 30 mJ, 500 μs pulse duration, and 500 Hz pulse rate was delivered to human uric acid stones, ex vivo. Stone ablation rates measured 1.5±0.2 mg/s, comparable to 1.7±0.3 mg/s using bare fiber tips separately with stone basket. With further development, this device may minimize stone retropulsion, allowing more efficient TFL lithotripsy at higher pulse rates. It may also provide increased flexibility, higher saline irrigation rates through the ureteroscope working channel, reduce fiber degradation compared with separate fiber and basket manipulation, and reduce laser-induced nitinol wire damage.
Introduction
H
Multiple endoscopic devices have been used to minimize stone retropulsion, and the stone basket is commonly used to retrieve stone fragments and minimize stone retropulsion during holmium laser lithotripsy. 12 Simultaneous, side-by-side use of a standard 270-μm core holmium laser fiber (464-μm outer diameter [OD]) and conventional 1.9F (633-μm OD) stone basket, however, limits saline irrigation rates because of space limitations within the single 3.6F (1.2–mm inner diameter [ID]) ureteroscope working channel. Saline irrigation during laser lithotripsy is important for flushing away stone debris and maintaining adequate visibility in the surgical field for safety.
While larger basket devices incorporating fibers are available, including 2.5F (833-μm OD) sheath with 150-μm core fiber and 3.0F (1.00-mm OD) sheath with 270-μm core fiber, they are not widely used, possibly because of concerns with reduced irrigation rates that compromise visibility and safety, and the larger, less flexible stone baskets that impede ureteroscope flexion.
The thulium fiber laser (TFL) is being studied as a potential alternative to the gold standard holmium laser for lithotripsy. 13 –24 The TFL wavelength of 1908 nm more closely matches a major water absorption peak in tissue than does the holmium laser wavelength of 2120 nm, translating into a TFL stone ablation threshold four times lower than for the holmium laser. 16 The shorter optical penetration depth in water at the TFL wavelength (∼80 μm for TFL vs ∼330 μm for holmium) also provides an improved safety profile compared with the holmium laser, with respect to undesirable collateral damage to the ureter and stone baskets during lithotripsy. 24
While the flashlamp-pumped holmium laser is limited to operation at low pulse repetition rates because of thermal effects in the laser rod, the diode-pumped TFL does not have such thermal limitations. The TFL has been tested at high pulse repetition rates up to 500 Hz for more rapid stone ablation compared with holmium laser lithotripsy performed at 600 mJ and 6 Hz through a 270-μm core fiber. 22 In addition, the near-single mode, uniform, spatial beam profile of the TFL originating from an 18-μm core thulium-doped silica fiber allows coupling of higher laser power into smaller (e.g., 50- and 100-μm core) fibers than does the nonuniform, multimodal holmium laser beam profile (e.g., ≥200 μm core). 14,15,23
The use of smaller fibers may be advantageous for laser lithotripsy procedures performed in the lower pole of the kidney, which necessitates extreme flexion of the ureteroscope without impedance from the fiber to access this difficult-to-reach location. Use of smaller, 100-μm core fibers (140-μm OD), may also enable further miniaturization of ureteroscopy tools, including stone baskets, which should in turn translate into higher saline irrigation rates through the ureteroscope working channel and result in improved visibility and safety. Insufficient irrigation through the ureteroscope working channel is a significant clinical concern that has motivated continued development of smaller diameter stone baskets for improved irrigation. 25 –27
A limitation of smaller fibers is that they are delicate and more susceptible to fiber fracture, degradation, and/or burnback during lithotripsy. 28 Recent studies have also found that initial fiber tip preparation (e.g., stripping and cleaving) also plays a significant role in fiber tip degradation. 29 Use of small fibers with a hollow steel distal tip design has been reported for reducing fiber tip damage during TFL lithotripsy. 20
This study describes preliminary ex vivo testing of a novel miniaturized and integrated hollow steel tip fiber and stone basket device. The device is designed to minimize stone retropulsion (which becomes a limitation for TFL operation at very high pulse rates 22 ) for more efficient TFL ablation of urinary stones, but also for improved flexibility, higher saline irrigation rates, decreased fiber burnback, and lower probability of laser-induced nitinol wire damage, compared with separate use of nonintegrated, bare-tipped fibers with stone baskets.
Description of Technology
A 100-W, continuous-wave, thulium fiber laser (TLR 110-1908, IPG Photonics, Oxford, MA) with a center wavelength of 1908 nm was used. The laser beam was focused down to a 25-μm-diameter spot for coupling into a 100-μm core, low-OH silica optical fiber (FIP100120140, Polymicro, Phoenix, AZ) with 120 μm cladding and 140 μm buffer. The laser was electronically modulated to produce a pulse energy of 32.5 mJ, pulse duration of 500 μs, and pulse rate of 500 Hz. The pulse duration of 500 μs was chosen to be comparable to holmium laser pulse durations of 350–700 μs commonly used in the clinic. Given this TFL pulse duration, the laser was limited to a maximum pulse energy of 32.5 mJ. The TFL pulse rate of 500 Hz was chosen based on recent studies that showed that high stone ablation rates could be achieved at laser pulse rates up to 500 Hz, and that stone ablation rates scaled linearly with laser pulse rates. 21,22
The fiber buffer was removed from the distal fiber tip and stainless steel hypodermic tubing with ID and OD of 178 and 356 μm, cut to a length of 5 mm, was used for each hollow tip. The fiber was recessed in the tube to a distance of 500 μm under magnification, based on optimal results from a previous study 20 (Fig. 1).
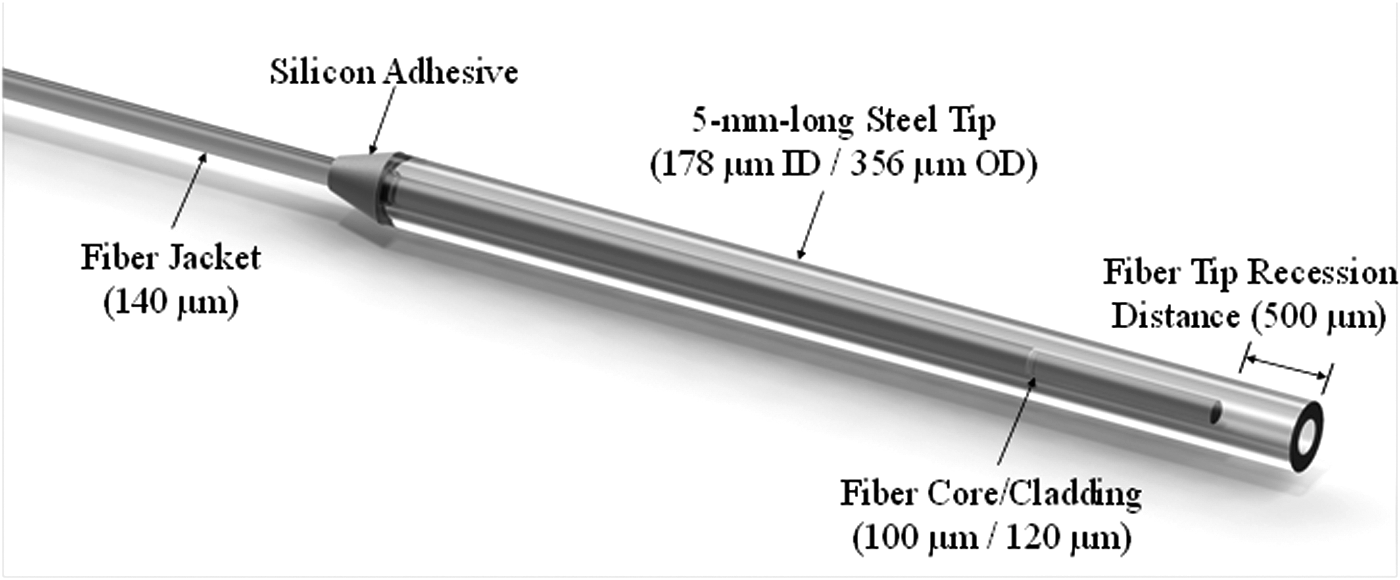
Diagram showing 100-μm core silica distal fiber tip recessed 500 μm inside the hollow stainless steel tubing. ID=inner diameter; OD=outer diameter.
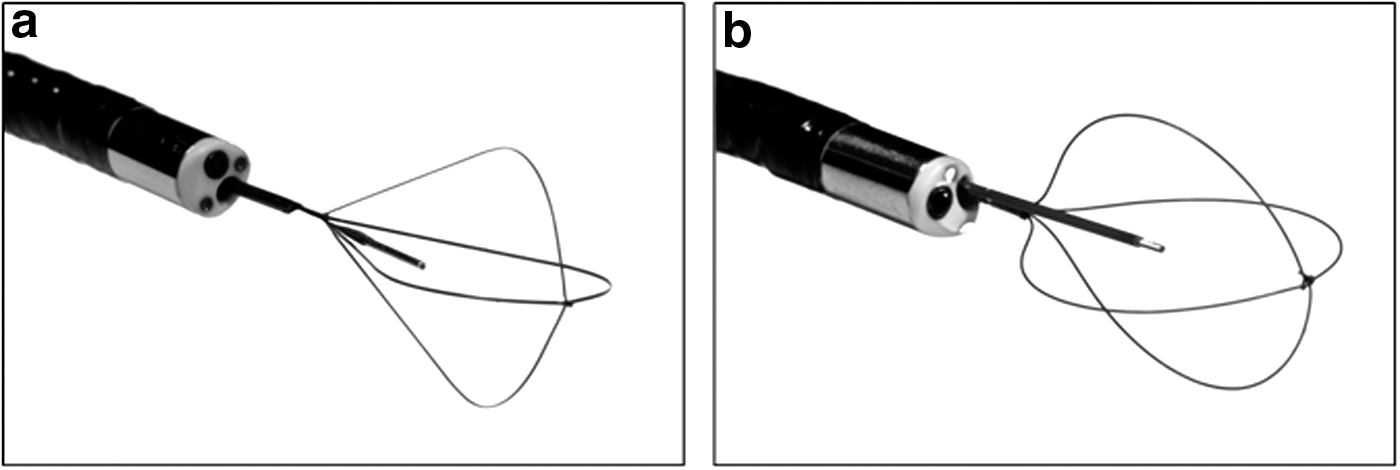
A stone basket (Zero Tip Nitinol Stone Retrieval Basket, Boston Scientific, Natick, MA) with sheath OD of 1.9F (633 μm) was dismantled to salvage the insertion sheath. A second stone basket (Optiflex Nitinol Stone Retrieval Basket, Boston Scientific) with sheath OD of 1.3F (433 μm) was also dismantled for the nitinol four-wire cage and wire for manipulation. These harvested parts were then combined with a 100-μm core trunk fiber and hollow steel tip to comprise an integrated fiber/basket device (Fig. 2a). All of the individual components used to assemble this “single-use” integrated fiber/basket device were inexpensive and commercially available.
(
Human uric acid (UA) stones with 4 to 11 mm diameter and 164 to 476 mg mass were desiccated in an oven and weighed with an analytic balance before and after lithotripsy to determine mass loss. The laser fiber and stone basket were inserted through the ureteroscope working channel and placed in contact with the stone sample, submerged in saline. Illumination from the ureteroscope and a magnified image from a charge-coupled device camera were used to observe the procedure. The integrated device testing involved using a 1.3F (0.433-mm OD) stone basket for stone stabilization. Stone vaporization rate (mg/s) was calculated by determining net mass loss as a function of laser irradiation time.
Residual stone samples greater than 2 mm were included in the measurements, consistent with the clinical end point for successful stone fragmentation. A minimum of five samples were tested for each data set, and mean±standard deviation was recorded. A paired Student t test was performed to determine statistical significance (P<0.05).
After stone ablation, a separate 140-μm OD fiber was placed into the distal opening of the hollow fiber tips, and the inserted distance was measured. The overall fiber burnback distance was recorded by comparing this measurement with the original depth before stone ablation.
Saline irrigation rates were measured by introducing gravitational flow from a saline bag (at a fixed height of 100 cm) through the 3.6F (1.2 mm) single working channel of a flexible ureteroscope (Uretero-Reno Videoscope URF-V, Olympus, Southborough, MA). Saline flowed freely through the ureteroscope for 2 minutes for each experiment. Saline irrigation studies were conducted using a combination of different fibers and stone baskets, including experimental 100-μm-core silica fiber, clinical 270-μm core fiber (Holmium Lightguide 270D fiber, Olympus Gyrus ACMI), 1.3F stone basket, and 1.9F stone basket. Saline volume was measured with a graduated cylinder. A sample size of n=3 was performed for each study with mean±standard deviation recorded. Percent flow was calculated by dividing flow with an instrument inserted by flow through the empty working channel (control) without a fiber or basket present.
The same flexible ureteroscope as used for irrigation rate studies was also used to perform forward and reverse deflection tests both with and without the integrated fiber/stone basket inserted through the ureteroscope working channel. The maximally flexed ureteroscope configurations were photographed, and then a protractor was used to measure deflection angle.
Role in Endourology
TFL stone ablation rates using the integrated fiber/basket device measured 1.5±0.2 mg/s for UA stones, comparable to 1.7±0.3 mg/s (P=0.15) using bare fiber tips separately with a stone basket, for TFL ablation with incident pulse energy of 30 mJ, pulse duration of 500 μs, and pulse rate of 500 Hz. No measurable amount of distal fiber tip burnback was observed after UA stone ablation studies with the steel tipped fibers, as determined by inserting a separate fiber into the hollow tip. By contrast, for the bare fiber tips, a variable burnback rate averaging 180±220 μm/min was measured. There were also no observed cases of device failure (e.g., separation of the metal tip from the fiber during lithotripsy or damage to basket wires).
Table 1 shows saline irrigation rates through the working channel of the flexible ureteroscope as a function of instrument (fiber and/or stone basket) size. Comparison of the integrated instrument (100-μm core fiber, 1.3F basket, and 1.9F sheath) to simultaneous, side-by-side use of conventional 270-μm core fiber and 1.9F basket provides flow rates of 19.2 % and 7.7 % of the empty channel flow rates, respectively. Thus, the integrated device improved irrigation flow by a factor of 2.5. (Holmium laser fiber dimensions are frequently mislabeled and differ significantly in their dimensions based on manufacturer, 30 which has a direct effect on saline irrigation rates. The core, cladding, and jacket layers of the 270-μm core fiber provided in Table 1 and used in this study were carefully measured in the laboratory.)
OD=outer diameter.
Figure 3 shows the influence of the integrated fiber/stone basket device on ureteroscope deflection. Forward deflection with and without the device measured 240 and 260 degrees. Reverse deflection with and without the device measured 155 and 165 degrees. Previous studies have reported that maximum deflection of this specific ureteroscope decreased from 275 to 217 degrees (forward) and 180 to 161 degrees (reverse) with prolonged clinical use. 31 Thus, although there is some measurable loss of ureteroscope deflection using the integrated fiber/basket device, it appears to be minimal compared with normal loss of flexion experienced with standard repeated use of the ureteroscope.
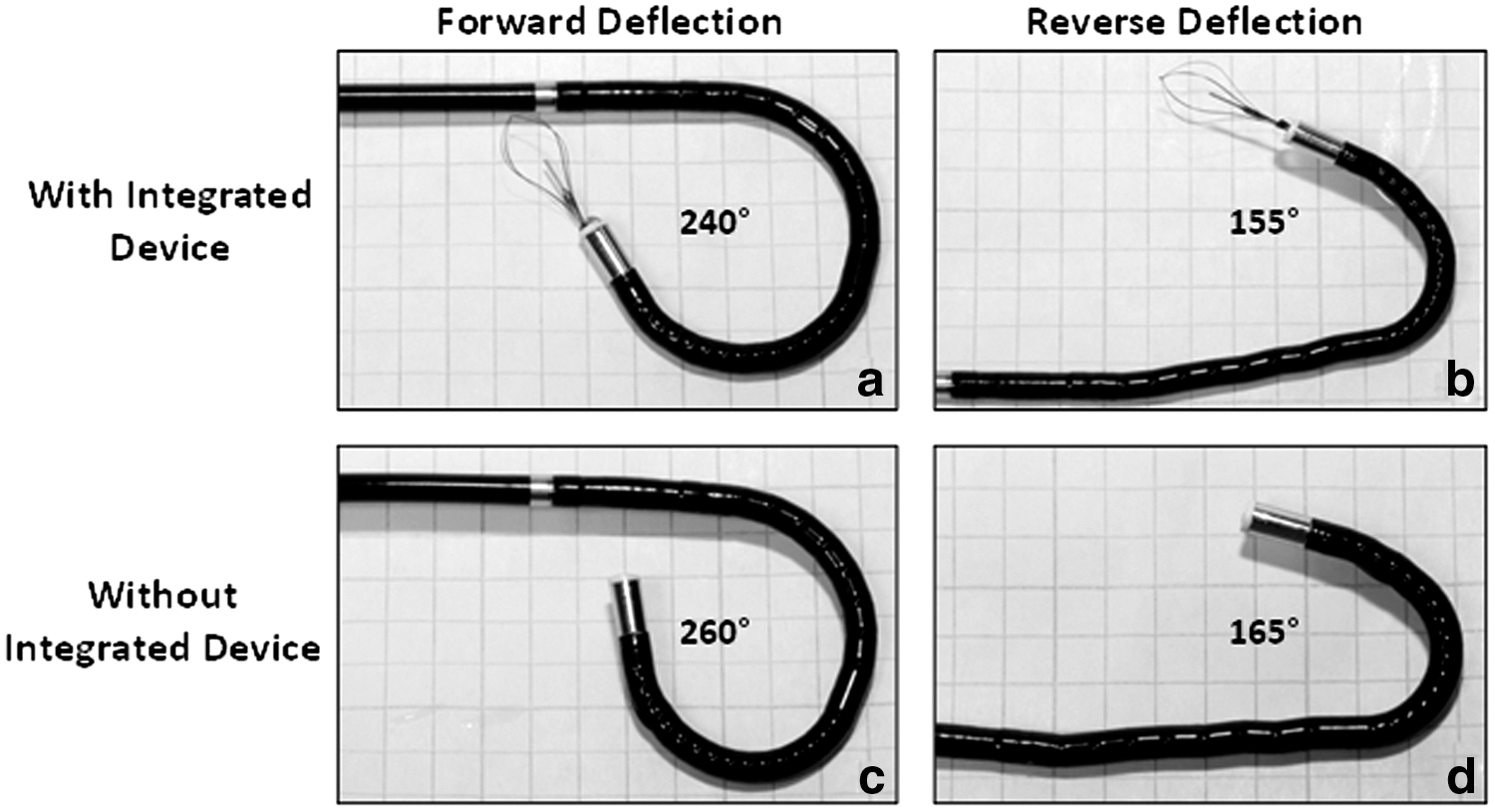
Ureteroscope deflection tests performed using integrated fiber/stone basket device inserted through the ureteroscope working channel. (
In summary, an integrated 1.9F (0.633-mm OD) device consisting of a steel tip fiber and stone basket was successfully built and tested, providing comparable TFL stone ablation rates to bare fibers when operated at pulse rates up to 500 Hz. This device may provide not only more efficient stone ablation with minimal stone retropulsion, but also improved flexibility, higher saline irrigation rates, reduced fiber burnback, and less probability of laser-induced nitinol wire damage, compared with current use of separate, nonintegrated, bare fiber tips with stone baskets.
This miniaturized device is also significantly smaller than the smallest commercially available, 2.5F (0.833-mm-OD) stone basket that accepts 150-μm core fibers (Laser Flat Wire Stone Extractor, Cook Urological, Bloomington, IN). With further development, it may be possible to reduce the size of our integrated fiber/basket device below 1.9F, using even smaller 1.2F stone baskets, 27 in combination with our recently tested 50-μm core, 85-μm OD fibers. 23
Footnotes
Acknowledgments
Christopher Wilson was supported by a seed grant from the Office of Technology Transfer and the Center for Biomedical Engineering and Science at UNC-Charlotte. Luke Hardy was supported by an undergraduate summer research fellowship from the Charlotte Research Scholars program at UNC-Charlotte. Thomas Hutchens is currently an optical engineer with Opto-Alignment, inc. (Indian Trail, NC). The authors thank William Perkins for his assistance with the studies.
Author Disclosure Statement
Nathaniel Fried is currently a consultant with Boston Scientific Corporation. The research described in this manuscript was completed before this consulting arrangement. Nathaniel Fried has also received previous research funding from Covidien and Lockheed Martin Aculight for unrelated projects. For the remaining authors, no competing financial interests exist.