
Abstract
Purpose:
To describe the utilization of shockwave lithotripsy (SWL) and ureteroscopy (URS) in ambulatory surgery centers, as well as to identify patient-specific factors predictive of one procedure over the other.
Patients and Methods:
We evaluated the current trends in the use of SWL and URS in the ambulatory settings over a 5-year period in the state of California using the State of California Office of Statewide Health Planning and Development (OSHPD) database.
Results:
We identified 113,447 ambulatory kidney stone surgical procedures including 64,632 SWL (57%) and 48,815 URS (43%) treatments in the OSHPD database between 2005 and 2010. The total annual ambulatory stone surgeries increased from 17,831 cases in 2005 to 18,933 cases in 2010 (P<0.001). Between 2005 and 2010, the use of URS increased significantly from 6978 (39%) cases in 2005 to 9259 (49%) cases in 2010 (P<0.0012), whereas the use of SWL decreased from 10,853 (61%) cases in 2005 to 9674 (51%) cases in 2010 (P=0.0012). In multivariate analysis, age≥75 years (P<0.001), hypertension (P=0.025), and obesity (P<0.001) all increased odds of undergoing URS. In addition, men (P=0.013) and non-Medicaid patients (P<0.001) were more likely to undergo URS.
Conclusions:
The use of URS increased significantly in the state of California among patients undergoing urinary stone surgical procedures in the ambulatory setting, while the use of SWL decreased between 2005 and 2010. Possible explanations for these trends include improved URS stone-free rates, improved cost-effectiveness of URS, and enhanced technology leading to increased use of URS over SWL.
Introduction
U
Increasing prevalence of urolithiasis necessitates the need for safe, efficacious, and affordable treatment when surgical removal is warranted. The three most common procedures performed for the removal of upper urinary stones are shockwave lithotripsy (SWL), ureteroscopy (URS), and percutaneous nephrolithotomy. In the ambulatory surgery setting, SWL has long been the most used treatment modality. 3,4 Recent studies of the Medicare population, however, have shown that the use of URS in the ambulatory setting is on the rise. 5 It has been proposed that several factors play into this change, including patient and provider preference, differing stone-free rates (SFR), and overall cost of each treatment. 6 –9
Large population-based studies that compare the use of SWL and URS in the ambulatory setting have not yet been performed for younger patients in the United States. 10 The objective of this study was to evaluate the use of SWL and URS in the ambulatory surgery centers in the state of California from 2005 to 2010 for all adults, as well as to identify patient-specific factors predictive of one procedure over the other.
Patients and Methods
Data source
We used the State of California's Office of Statewide Health Planning and Development (OSHPD) database, which is a longitudinal database that captures general acute care hospitals and freestanding ambulatory surgery centers licensed by the California Department Public Health (CDPH). It must be noted, however, that not all freestanding ambulatory surgery centers are required to be licensed by the CDPH. Furthermore, in September 2007, a California court order changed the requirement for CDPH to license these facilities and instead required the Medical Board of California to assume this responsibility. The OSPHD database is publicly available and de-identified, and thus the Institutional Review Board of the University of California, San Diego, granted this study exempt status.
Study population
All patients 18 years or older who underwent SWL or URS from 2005 to 2010 were identified. Patients in the ambulatory setting were identified using Current Procedural Terminology codes (SWL 50590 and URS 52320, 52325, 52351, 52352, 52353).
Outcome variables
The primary end points of this study were the proportion of all stone treatments represented by each modality (SWL and URS), which were calculated annually.
Predictor variables
In each procedure category, patient demographics were recorded including age, sex, ethnicity (Caucasian or other), and insurance type (private, Medicare, Medicaid, or others). Clinical factors including stone location (renal versus upper ureteral), Charlson Comorbidity Index, and existing comorbidities (hypertension [HTN], diabetes, and obesity) were also described and analyzed.
Statistical analysis
Descriptive statistics of demographic, comorbidities, and third party payer were performed with proportions. Univariates analysis and multivariate analysis using binary logistic regression was performed to analyze covariates. Prevalence over time was examined using linear regression. We determined which covariates increased over time using the chi-square test. P value <0.05 is considered statistically significant. SPSS version 17.0 software (SPSS, Inc, Chicago, IL) was used for all statistical analyses.
Results
We identified 113,447 ambulatory stone surgeries for either SWL or URS in the OSHPD database between 2005 and 2010. A total of 64,632 SWL (57%) treatments and 48,815 URS (43%) treatments were performed in ambulatory settings in the state of California between 2005 and 2010 as captured by the OSPHD database.
Table 1 summarizes patient demographics, and clinical and stone characteristics for patients who underwent stone surgeries between 2005 and 2010 in the ambulatory setting obtained from the OSHPD database.
Considered statistically significant P<0.05.
The total number of annual ambulatory stone surgeries increased from 17,831 cases in 2005 to 18,933 cases in 2010 (P<0.001). Between 2005 and 2010, the use of URS increased significantly from 6978 (39%) cases in 2005 to 9259 (49%) cases in 2010 (P<0.0012), whereas the use of SWL decreased from 10,853 (61%) cases in 2005 to 9674 (51%) cases in 2010 (P=0.0012). In 2010, the number of URS performed in ambulatory settings (9259 cases, 49%) nearly equaled SWL (9674 cases, 51%) (Fig. 1).
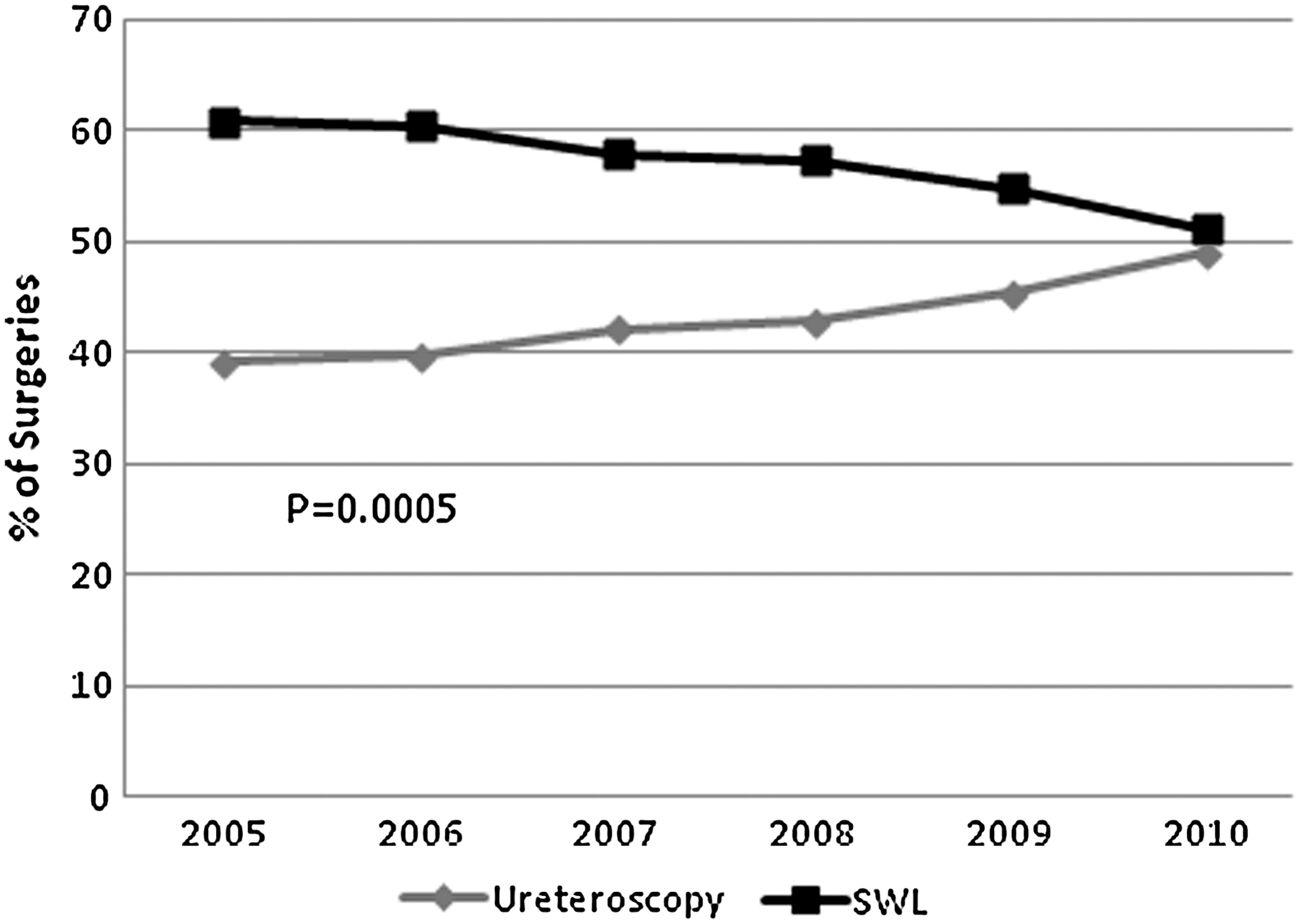
Ambulatory stone surgeries over time from 2005 to 2010, Office of Statewide Health Planning and Development. SWL=shockwave lithotripsy.
Univariate analysis is reported in Table 1. In multivariate analysis, age≥75 years (P<0.001), hypertension (P=0.025), and obesity (P<0.001) all increased odds of undergoing URS. In addition, men (P=0.013) and non-Medicaid patients (P<0.001) were more likely to undergo URS. For each year, patients were more likely to undergo URS than SWL, P<0.001 (Table 2).
Considered statistically significant P<0.05.
OR=odds ratio.
Discussion
While both SWL and URS are effective treatments for patients with upper urinary stones, emerging data challenge the notion that the two modalities have similar outcomes. 11 The development of SWL in the late 1970s and early 1980s provided a safe and noninvasive treatment option for patients with upper tract stone disease, supplanting the need for the more invasive surgical techniques of that era. Over the ensuing decades, however, URS has undergone significant refinement and now provides another effective, minimally invasive option for the management of upper tract stones. Indeed, ureteroscopic technology has advanced from large caliber, rigid scopes, to smaller, semirigid scopes, to the latest generation of flexible digital ureteroscopes with enhanced visualization, smaller calibers, and extended flexibility. Introduction of a myriad of disposable devices along with proven efficacy of the holmium:yttrium-aluminum-garnet laser has further increased URS adoption. In all, these changes have increased URS capability, safety, and efficacy to include the management of proximal ureteral as well as renal stones. 12,13
In this study, we present population-based data showing a major shift in practice patterns for the state of California. Others have also documented similar trends in North America. A 19- year Canadian study of the province of Ontario was the first analysis to demonstrate an increase in URS utilization with a reciprocal decrease in SWL utilization. 14 From 1991 to 2010, SWL use decreased from 69% to 34% of all procedures (P<0.0001) and URS use increased from 25% to 59% of all procedures (P<0.0001). Ancillary procedures for SWL remained unchanged while URS ancillary procedures significantly decreased. 14
A study of the Nationwide Inpatient Sample database demonstrated different results with both SWL and URS utilization unchanged from 1999 to 2009. This administrative dataset, however, only evaluated inpatient care and likely excluded a large proportion of the outpatient SWL and URS procedures. 10 Lastly, an investigation of the Medicare dataset from 1997 to 2007 uncovered potential factors that predict choice of SWL and URS, but did not seek to document temporal trends of procedural use. 5 To our knowledge, this is the first population-based report demonstrating an almost equivalence in utilization of SWL and URS within the United States.
Unlike SWL, technology advances and improvement of URS have taken significant strides over last few decades. With this technological advancement, there has been noticeable increase in URS adoption among urologists. Furthermore, two separate reports of the American Board of Urology case logs indicate a shift in adoption from only younger urologists to both younger and older urologists increasing their use of URS over SWL. 9,15
Improvements in flexible ureteroscopic technology resulting in decreased costs as well as improvements in surgical outcomes such as SFR and re-treatment rate may play a role in these trends. 11 –13 Furthermore, these studies indicate URS reporting appears to be higher in practitioners who have more recently completed their urologic training. Although more senior urologists reported an increase in URS use, more junior urologists still reported a higher use of URS. 15 These trends together may indicate that increased URS use is because of increased exposure during residency training and increased competency with these techniques.
Despite these theories being attractive and intuitive, the current body of literature still does not permit a true causal relationship to be established. Furthermore, existing reports fail to determine the effect of patient preference in evolving utilization. That withstanding, our study is interesting in that URS use within this region of the United States is on track to equal SWL use, if not overcome its use with time. And if, in fact, URS truly represents a more efficacious technology over SWL, these trends are encouraging as they align outcomes with utilization—particularly because the SWL higher reimbursement rate poses a potential misalignment of incentives with outcome efficacy.
Whether our study's findings are simply regional phenomena is unclear and will need other regional reporting; however, there appears to be growing evidence from other national sources (Medicare and inpatient data) that these trends may not be regionalized in the United States. We also acknowledge certain limitations exist in that the OSHPD dataset does not capture all the ambulatory surgical centers. Furthermore, centers were no longer required to report to CDPH after September 2007. Both of these factors introduce an underreporting effect to our data and conceivably threaten its internal validity, although it is noteworthy that data preceding this court order (2005–2007) demonstrated a rise in URS with a relatively stable use of SWL. Whether centers rapidly converted from OSHPD licensing to CA medical board licensing through the remainder of the analysis time period is unknown (2008–2010), which may mitigate the underreporting bias.
Lastly, the analysis also suggests that elderly age, male sex, obesity, HTN, and non-Medicaid insurance were clinical factors that predicted use of URS. Compromised efficacy of SWL with obesity is well established, but it is otherwise not possible to explain the relationship of these other factors with the choice of technology from this population-based database.
Conclusions
Our analysis of the OSHPD data suggests that use of URS has increased significantly in the state of California among patients undergoing upper tract urinary stone surgery in the ambulatory setting, while use of SWL have decreased between 2005 and 2010. For the first time, the use for URS and SWL are nearly equal in California. Future studies guiding the management of upper urinary tract stones will require geographically broader datasets that also contain the granular detail needed to examine SFR, cost-effectiveness, and procedurally related complications.
Footnotes
Author Disclosure Statement
No competing financial interests exist.