
Abstract
Purpose:
To analyze the impact of warm ischemia time (WIT) on early postoperative and ultimate renal function after elective laparoscopic partial nephrectomy (LPN).
Patients and Methods:
One hundred and twenty-seven patients who underwent elective, ischemia-applied LPN were investigated in this study. The study patients were without stage 3 or greater chronic kidney disease (CKD) (estimated glomerular filtration rate [eGFR] <60 mL/min/1.73 m2) before LPN. Initially, the patients were grouped using the criteria of postoperative de novo stage 3 or greater CKD: Group A (n=104, eGFR ≥60 mL/min/1.73 m2) and group B (n=23, eGFR <60 mL/min/1.73 m2). The patients were also divided into two groups using 27.75 minute cutoff value obtained by receiver operating curve (ROC) analysis for WIT: Group 1 (n=69, WIT <27.75 min) and group 2 (n=58, WIT ≥27.75 min). The groups were compared with regard to demographic, perioperative, histopathologic, and renal functional outcomes.
Results:
The decreased preoperative eGFR (P<0.001) and increased WIT (P=0.007), operative time (P=0.015), diabetes mellitus (DM) rate (P=0.019) and pathologic tumor size (P=0.031) were significantly different in group B. Multivariate analysis determined that independent predictors of de novo stage 3 or greater CKD in the early postoperative period were preoperative eGFR (P<0.001), WIT (P=0.014), and DM (P=0.030); meanwhile, preoperative eGFR (P=0.006) was the only independent predictor at last follow-up. Decreased median postoperative eGFR (P=0.018) and percent preserved postoperative eGFR (P=0.001) were significantly different in the increased WIT group, as well as elevated median postoperative eGFR loss (P=0.001). After similar follow-up (26 vs 23.5 months, P=0.913), the increased and limited WIT groups were not significantly different with regard to final eGFR (P=0.936), final eGFR loss (P=0.749) and percent preserved final eGFR (P=0.690).
Conclusions:
In elective LPN, increased WIT plays an important role in renal functional loss in the early postoperative period. This functional loss, however, recovered after an intermediate term follow-up period, similar to that of patients undergoing limited WIT.
Introduction
T
Renal hilar clamping, which may potentially cause warm ischemic kidney damage, is generally needed to control blood loss, achieve better visualization for negative oncologic margins, and perform precise renorraphy during PN. The mechanisms of ischemic renal injury are attributed to postischemic vasoconstriction with endothelial injury and mechanical obstruction of microvessels by leukocytes and platelets during the inflammatory process. 3 Meanwhile, reperfusion injury also decreases organ activity. Therefore, it has been emphasized that limiting WIT minimizes its effects on renal damage. 4
On the other hand, renal tolerance to prolonged WIT has also been mentioned by some authors. 5 –7 Recently, this concept has become crucial for patients undergoing PN because the significant role of factors other than the WIT, such as the quality and quantity of preserved renal parenchyma on final renal function, were reported by studies with long-term follow-up. 8 –10 In addition, the question of whether warm ischemia causes renal dysfunction that may resolve over time can be difficult to determine, especially in patients with a functioning contralateral kidney.
In the present study, we investigated the effect of WIT on renal function and consequences of warm ischemia-related renal dysfunction after elective laparoscopic PN (LPN) in patients with a contralateral functioning kidney.
Patients and Methods
Between February 2008 and July 2014, 185 patients with suspected renal masses underwent LPN at our institution. Fifty-eight patients were excluded, consisting of 21 whose records were incomplete or had follow-up of less than 6 months, 14 who underwent clampless LPN, 11 with a solitary kidney, 5 with Clavien classification III or greater complications (1 urinary fistula necessitating a nephrostomy tube, 1 reoperation for severe bleeding from the renal bed, 1 hemorrhage necessitating renal angiography and embolization, 1 vena cava injury, and 1 intraoperative severe bleeding from the adrenal gland), and 7 with preexisting stage 3 or greater chronic kidney disease (CKD) (estimated glomerular filtration rate [eGFR] less than 60 mL/min/1.73 m2) before LPN.
Finally, 127 patients with a contralateral functioning kidney who underwent clamped LPN were identified for this study. Our previously described LPN technique was performed for each of these patients, and all procedures were completed laparoscopically. 11 The WIT was defined as the interval between the first placement and removal of hilar clamping. No additional techniques, including renal cooling and protective agents, were administered. To standardize tumor characteristics, the preoperative aspects and dimensions for an anatomic (PADUA) classification and R.E.N.A.L. (radius; exophytic/endophytic; nearness; anterior/posterior; location) nephrometry scores were preoperatively calculated. 12,13
De novo stage 3 or greater CKD in the postoperative hospitalization period was characterized as renal dysfunction, and the patients were divided into two groups using these criteria: Group A (n=104, postoperative eGFR ≥60 mL/min/1.73 m2) and group B (n=23, postoperative eGFR <60 mL/min/1.73 m2). The prospectively recorded demographic, perioperative, and histopathologic outcomes were retrospectively compared between the groups. The significant factors in this comparison were further used as covariables in a multivariative analysis to define independent predictors of de novo stage 3 or greater CKD in the early postoperative period and during follow-up.
For renal functional assessment, eGFR calculation was derived using the Modification of Diet in Renal Disease Study Equation formula. 14 The baseline and early postoperative eGFR levels were calculated using the serum creatinine (sCr) level that was measured within 3 days before the operation and maximum sCr level during postoperative hospitalization, respectively. The patients were followed up with the sCr and eGFR level at 3, 6, and 12 months after the surgical procedure and every 6 months after 1 year.
The latest eGFR was calculated using the sCr level at the last follow-up. The percentage of postoperative and latest preserved renal function were calculated using (postoperative eGFR/baseline eGFR)×100 and (latest eGFR/baseline eGFR)×100 formulas, respectively. All sCr measurements were made at a single reference laboratory. The National Kidney Foundation classification was used to define stage 3 CKD. 15
Statistical analysis
The Pearson chi-square and Mann-Whitney U tests were used to compare categorical and nonparametric continuous variables, respectively. The statistical significance was accepted as P<0.05. Using significant factors as covariables, logistic regression (forward stepwise) analysis was performed to determine independent risk factors. For logistic regression, the significant continuous variables were converted to categorical variables using the cutoff values obtained via receiver operating curve (ROC) analyses. The hazard ratios (HRs) with a 95% confidence interval (CI) were reported as relative risks for each independent factor.
Results
The rate of preexisting diabetes mellitus (DM) at the time of LPN was significantly higher in group B (20.2 vs 43.5%, P=0.019). Among the perioperative parameters, group B had a significantly decreased median preoperative eGFR (90 vs. 72 mL/min/1.73 m2, P<0.001), increased median operative time (OT, 120 vs. 140 min, P=0.015) and WIT (25 vs 29 min, P=0.007). The pathologic tumor size was significantly increased in group B (3.2 vs 4.0 cm, P=0.031, Table 1). There were no differences between the groups with respect to PADUA (P=0.465) and R.E.N.A.L. nephrometry (P=0.605) scores and any other demographic, perioperative, and histopathologic parameters.
eGFR=estimated glomerular filtration rate; DM=diabetes mellitus; HT=hypertension; ASA=American Society of Anesthesiologists; PADUA=preoperative aspects and dimensions for an anatomic; R.E.N.A.L.=radius; exophytic/endophytic; nearness; anterior/posterior; location; Hgb=hemoglobin; RCC=renal–cell carcinoma.
A multivariative analysis for detecting independent predictors of early postoperative de novo stage 3 or greater CKD was performed using the preexisting DM, preoperative eGFR, OT, WIT, and pathologic tumor size. Continuous variables were converted to categorical variables using the cutoff values obtained by ROC analyses. The cutoff values were 80 mL/min/1.73 m2 (sensitivity=0.280, specificity=0.234, P<0.001), 122.5 min. (sensitivity=0.560, specificity=0.607, P=0.036), 27.75 min (sensitivity=0.640, specificity=0.571, P=0.008), and 3.6 cm (sensitivity=0.609, specificity=0.606, P=0.031) for the preoperative eGFR, OT, WIT and pathologic tumor size, respectively.
Accordingly, multivariative analysis revealed that a preoperative eGFR less than 80 mL/min/1.73 m2 (HR=12.67; 95% CI: 3.97–40.25, P<0.001), WIT longer than 27.75 min (HR=4.07; 95% CI: 1.33–12.48, P=0.014), and DM (HR=3.56; 95% CI: 1.13–11.12, P=0.030) remained independent risk factors for predicting early postoperative de novo stage 3 or greater CKD (Table 2). Moreover, the same variables were assessed for predicting stage 3 or greater CKD at the latest follow-up, and preoperative eGFR less than 80 mL/min/1.73 m2 was the only predictor of stage 3 or greater CKD (HR=4.9; 95% CI: 1.57–15.26, P=0.006) after a median follow-up of 26 months.
Because the WIT was determined as one of the independent predictors for early postoperative de novo stage 3 or greater CKD, the patients were restratified into two groups using 27.75 min WIT as the cutoff value, which was obtained via ROC analysis (sensitivity=0.640, specificity=0.571, P=0.008), for group 1 (n=69, WIT<27.75 min) and group 2 (n=58, WIT 27.75 min), and we compared the clinicohistopathologic and renal functional outcomes between the groups. There was no significant difference between groups 1 and 2 in terms of the demographic, perioperative, and histopathologic parameters, except OT and estimated blood loss, favoring group 1 (Table 3).
WIT=warm ischemia time.
Renal functional analyses showed that group 2 patients had a significantly lower median early postoperative eGFR (79 vs 72 mL/min/1.73 m2, P=0.018), higher rate of de novo stage 3 or greater CKD (11.6 vs 25.9%, P=0.038), and increased median early postoperative eGFR loss (5 vs 17 mL/min/1.73 m2, P=0.001). The percent of preserved early postoperative eGFR was significantly higher in group 1 patients (91.7 vs 81.1%, P=0.001) (Table 4).
After a similar median follow-up (26 vs 23.5 months, P=0.913), the median latest eGFR level (81 vs 80.5 mL/min/1.73 m2, P=0.936), rate of stage 3 or greater CKD (10.1 vs 15.5%, P=0.363), and median latest eGFR loss (6 vs 10 mL/min/1.73 m2, P=0.749) were not significantly different between groups 1 and 2. In addition, the percent of the preserved latest eGFR was similar between the two groups (90.2 vs 88.3%, P=0.690).
Figure 1 is a scatterplot of the relationship between the WIT and percent change of eGFR during the early postoperative period (Fig. 1a) and at the latest follow-up (Fig. 1b). Figure 2 charts the percent of preserved eGFR at different points in the limited and increased WIT groups.
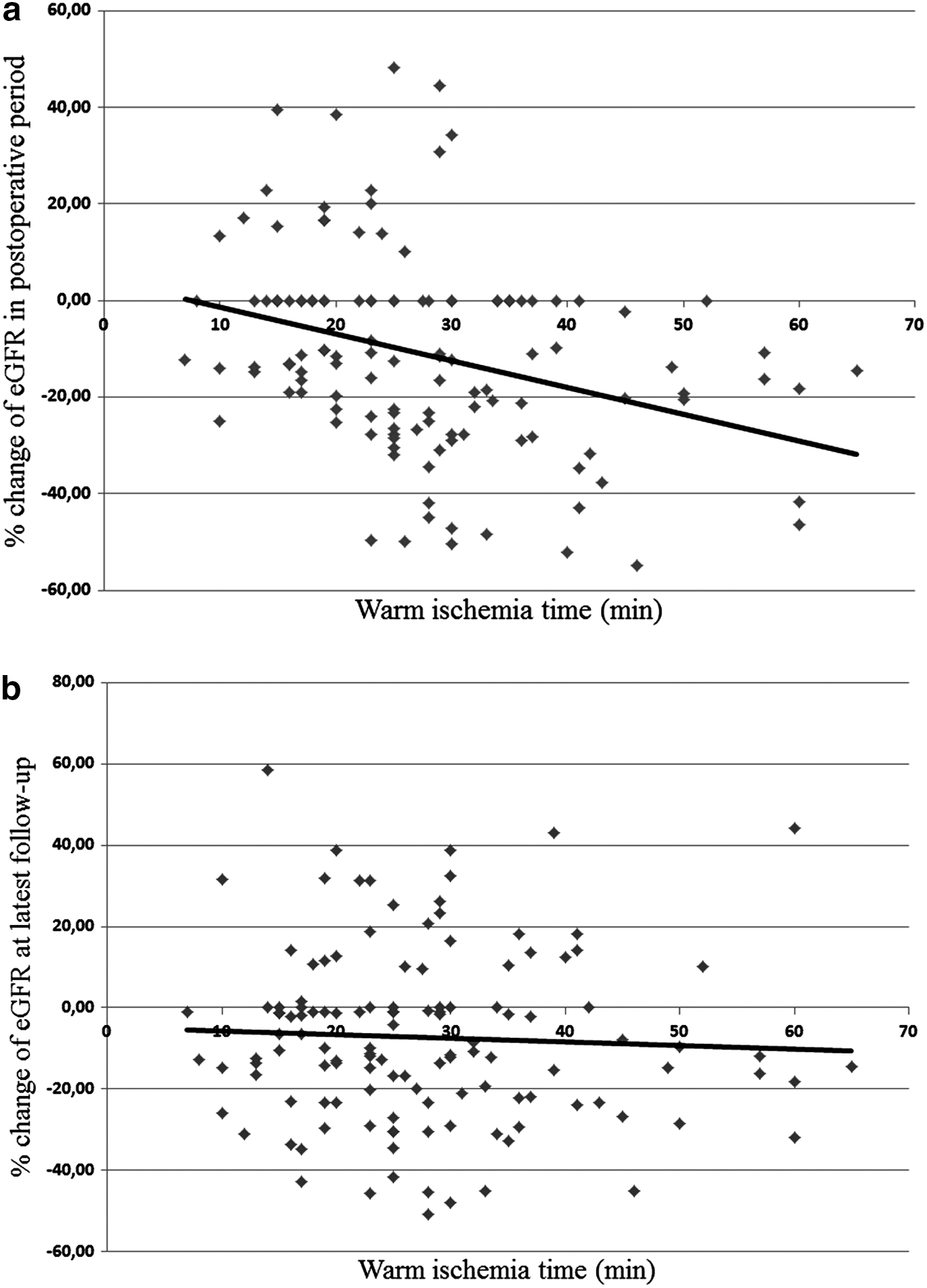
Scatterplot of relationship between % change of estimated glomerular filtration rate (eGFR) and warm ischemia time in postoperative period
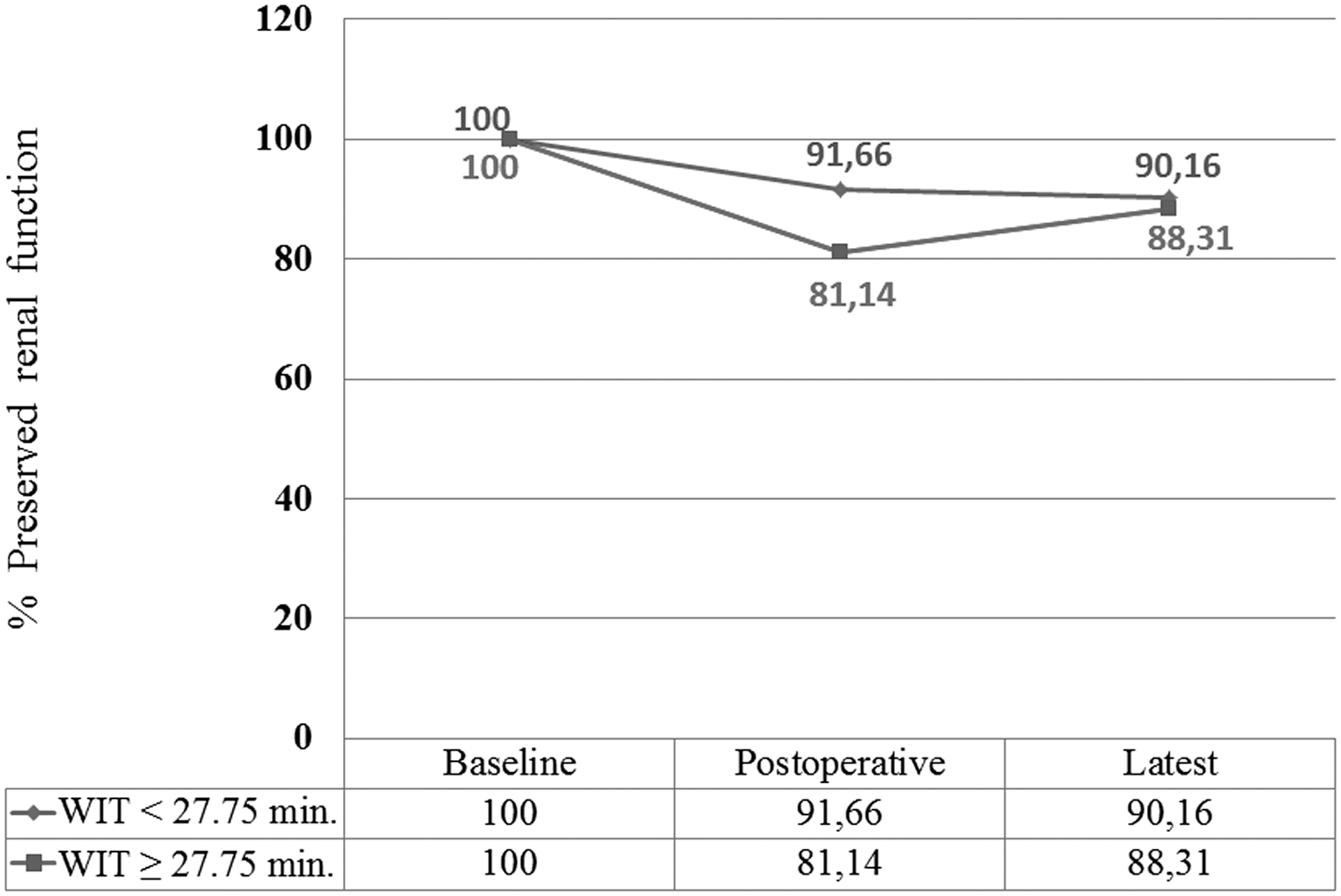
Line charts of % preserved renal function at baseline, postoperative period, and latest follow-up in limited and increased warm ischemia groups. WIT=warm ischemia time.
Discussion
LPN is a surgical treatment option for patients with T1 renal masses that is largely available in tertiary centers. As well as achieving satisfactory oncologic outcomes, preservation of maximum functional nephrons is one of the main goals of LPN. Several patient-, tumor-, and surgery-related factors, however, such as the duration of the ischemic interval, could interfere with this goal. To optimize renal functional preservation, several innovative techniques have been described to limit the WIT, including early unclamping, regional hypothermia, and without (zero) ischemia. 16 –19
The present study confirms that the WIT is an important independent predictor of postoperative renal dysfunction with some other nonmodifiable factors, such as preoperative eGFR and preexisting DM. We determined the safe limit for the WIT in LPN as 27.75 minutes, and a WIT longer than this cutoff independently increased the risk of de novo stage 3 or greater CKD 4.07-fold during the early postoperative period.
The consequences of the ischemia-related dysfunction on the operated kidney may be evaluated in two groups of studies: (1) Studies with a solitary kidney undergoing PN and (2) studies evaluating the affected kidney in patients undergoing elective PN.
Regarding PN in solitary kidneys, a study with a large cohort of patients previously reported that warm ischemia, compared with no ischemia, was significantly associated with acute renal failure and eGFR <15 mL/min per 1.73 m2 in the early postoperative period and new onset stage 4 CKD during follow-up. 20 Moreover, it was noted that every minute during hilar clamping increased the risk of kidney dysfunction. 21 Meanwhile, some experimental solitary kidney models in both open and laparoscopic procedures have investigated the upper limit of the WIT at which renal functional damage could be tolerated.
These studies have suggested that warm ischemia application up to 90 minutes causes postoperative renal dysfunction, and this dysfunction rapidly recovers within the first 15 postoperative days. 7,22,23 Although the pathophysiologic changes may differ between animal and human kidneys under ischemia, the contribution of these findings to clinical practice should be considered.
In patients with elective PN, the compensatory role of the contralateral functioning kidney might mask the functional damage of the operated kidney. For this reason, it might be rational to focus on studies using renal scintigraphy to assess differential renal function in patients undergoing elective LPN. Among these studies, Funahashi and associates 24 demonstrated a constant decrease in the effective renal plasma flow (ERPF) in the operated kidney by 28.7% and 21.1%, at postoperative 1 week and 6 months, respectively. They also reported that this decrease was greater in the patients with a WIT greater than 25 minutes.
Another study concluded that the risk of ERPF decrease greater than 20% (defined as loss of renal function) in the operated kidney was significantly increased in patients with a WIT longer than 25 minutes at both the postoperative 3 and 12 months. 25 Similarly, Choi and colleagues 26,27 showed a significant, consistent renal functional reduction of the operated kidney at 3 and 12 months after LPN in patients with a WIT greater than 28 minutes. No significant change was noted in patients with limited WIT, however.
All of the aforementioned studies also showed that increased WIT severely decreased renal function in the operated kidneys in the early postoperative period, but the affected kidney had a trend of recovery after 6 or 12 months, but the rate of recovery is lower in cases with increased WIT. The long-term results of scintigraphic studies are more important for elective LPN indications to evaluate the differential functional change of the operated kidney.
Recently, the role of the quality (preoperative renal function) and quantity (the volume) of the preserved renal parenchyma, as well as the role of WIT, on the functional change after PN has been investigated. Therefore, the idea that limited WIT had only a marginal effect on kidney function became even more important in elective PN. 28 From this perspective, Simmons and coworkers 8 assessed the percent functional volume preservation (PFVP) using CT images of the kidney. In their subsequent report, which used the same methodology in a large group of patients with extended follow-up (1.2 years), the authors demonstrated that the PFVP and WIT were independent predictors of early postoperative GFR preservation, but only PFVP was critical for late GFR preservation. 9
Another study showed similar findings in a large series with solitary kidneys. 29 In that study, postoperative acute renal failure was associated with the preoperative eGFR, preserved kidney volume, and WIT, while stage 4 CKD during follow-up was associated with the preoperative eGFR and preserved kidney volume, but it was not associated with the WIT. In addition, Mir and colleagues 10 suggested that the preserved parenchymal volume primarily correlated with the ultimate preserved renal function, while the WIT played a secondary marginal role even if it was limited or hypothermia was used. All of these studies strongly suggested that the renal functional change after PN is not only correlated to the WIT, but it is also a result of the balance between the WIT, preoperative quality, and postoperative quantity of preserved kidney.
Our results contribute to the concept that the WIT has a marginal effect on the final renal function after LPN with a contralateral functioning kidney because no significant eGFR change was observed at the latest follow-up between patients with WIT ≥27.75 minutes and <27.75 minutes. In parallel with previous studies, WIT caused renal dysfunction in the early postoperative period, which seemed to recover during the intermediate-term follow-up.
The statistically significant early postoperative decrease of the percent of preserved eGFR (81.14%) in patients with increased WIT showed a tendency toward recovery (88.3%), which was closer to the percent of preserved eGFR for limited WIT cases (90.1%) after 2.1 years of follow-up. In other words, the characteristic of the increased warm ischemia-related kidney dysfunction in elective LPN is notable after the operation, but it is well tolerated during follow-up.
At this point, the evidence in the literature suggests that the contralateral kidney only plays a significant compensatory role in the initial period up to 3 months and no longer after 1 year. 10,27 Recently, it was also documented that kidneys undergoing hilar clamping recovered from ischemia-related renal dysfunction regardless of their poor or strong preoperative functional capacity. 30 The multivariate analyses in the present study revealed that the WIT only predicted the decreased renal function during only the early postoperative period, which was not the case for intermediate-term follow-up. The primary predictor of renal dysfunction (stage 3 or greater CKD) at both the early postoperative period and intermediate-term follow-up in this study was the preoperative eGFR, because of the preoperative quality of the kidney.
Of note, the predictive scores for operative challenge in PN might have a potential role for estimating renal function after PN. Neither the PADUA nor R.E.N.A.L. nephrometry scores, however, were associated with early postoperative or final renal function after LPN in the present study.
In particular, the role of pneumoperitoneum, which may be related to the WIT and renal functions, should also be mentioned. Current evidence suggests that the pressure of the pneumoperitoneum on the renal vessels might cause a constant decrease in the blood flow during LPN, which should help the renal parenchyma to tolerate the sudden effect of hilar clamping. 7,23,24 Therefore, the pneumoperitoneum could play a preconditioning role for kidney tolerance against warm ischemia, which might affect long-term renal function.
This study is not without limitations. One was the relatively small number of patients. The lack of quantitative analysis, such as preserved renal parenchyma, was another limitation, and its relationship between the WIT and preoperative eGFR was not evaluated. Other limitations include the retrospective nature of the study and the fact that nuclear scintigraphy was not performed to better assess ipsilateral renal function. Meanwhile, the relatively long-term follow-up was the major strength of the present study. Despite these limitations, this study supported the idea that WIT had a predominant role in predicting the early postoperative, but not the final, renal function in patients undergoing LPN with a contralateral kidney.
Conclusion
The present study revealed that an increased WIT causes early postoperative renal dysfunction after LPN in patients undergoing elective LPN. This renal dysfunction, however, resolves in intermediate-term follow-up, which is similar to patients with limited WIT. Meanwhile, the preoperative kidney function is the only predominant factor affecting both the early postoperative and final renal function after LPN.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.