
Abstract
Purpose
Materials and Methods:
The proposed stent comprised a 7F Double-J (DJ) stent and a polymeric flap valve. The valve was made of Tango Plus FLX980 and was fabricated using a 3D printer. Two types of stent were prepared for in vitro tests: DJ stents with (1) an uncoated valve (UCV) stent and (2) a parylene C coated valve (PCV) stent for enhanced biocompatibility. The flow characteristics of each stent were evaluated considering flow direction, parylene coating, and stent side holes, and were compared to the intact DJ stent.
Results:
The forward flow rate for the distal portion of the UCV and PCV stents was 9.8 mL/min and 7.8 mL/min at applied pressure of 15 cm H2O (normal anterograde pressure in patients with stents), respectively. Backward flow rate for the distal portion of the UCV and PCV stents was decreased by 28 times and 8 times at applied pressure of 50 cm H2O (maximum bladder pressure), respectively, compared with the distal portion of the intact DJ stent. Forward flow rates of whole stents were 22.2 mL/min (UCV stent) and 20.0 mL/min (PCV stent) at applied pressure of 15 cm H2O, and backward flow rates of whole UCV and PCV stents were decreased by 8.3 times and 4.0 times at applied pressure of 50 cm H2O, respectively, compared with the intact DJ stent.
Conclusions:
The anti-reflux ureteral stent was successfully designed and fabricated using a 3D printer. In vitro studies showed that the stent effectively prevented backward flow while minimizing reduction in forward flow.
Introduction
U
One method used to efficiently fabricate antireflux ureteral stents is three-dimensional (3D) printing. 3D printing is being widely used in various areas to fabricate complex structures, because it has the advantages of easy fabrication of miniaturized structures, high precision, mass production, rapid prototyping, and cost-effectiveness. 3D printing has been increasingly used in a variety of medical applications such as hearing aid molds, dental crowns, and prosthetic limbs, and even ureteral stents. 11 –17
This article aims to describe the design of an antireflux ureteral stent with a polymeric flap valve and the fabrication method using 3D printing. The stent effectively prevents backward flow with minimized reduction of the forward flow. A 3D printer was used to fabricate the miniaturized valves with high precision and rapid prototyping. Two whole DJ stents were prepared—one stent with an uncoated valve (UCV) and one with a parylene C coated valve (PCV) to enhance biocompatibility. Both stents were evaluated considering flow direction, parylene coating, and stent side holes and were compared with an intact DJ stent.
Materials and Methods
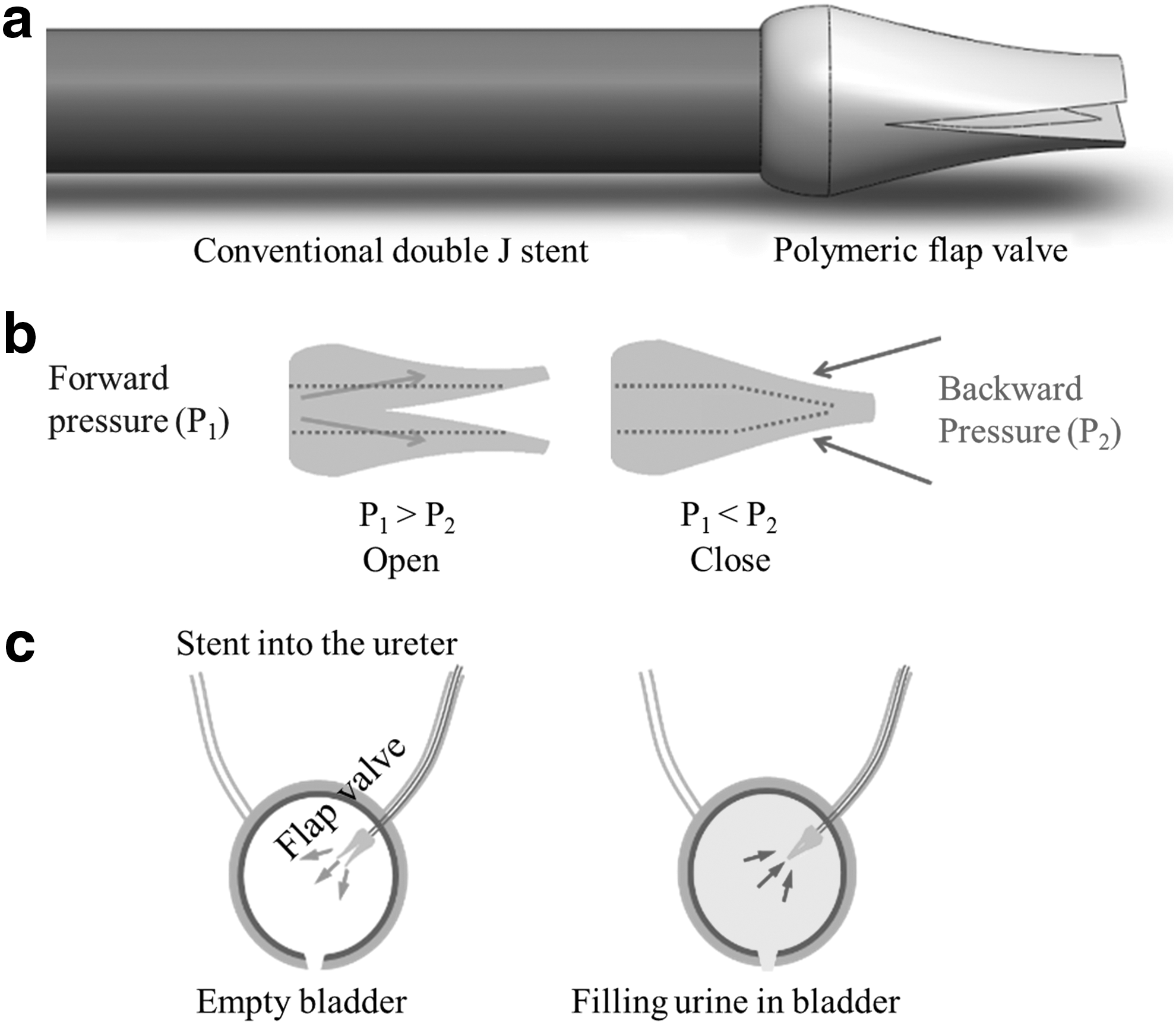
Figure 1a shows the configuration of the proposed stent. The stent was a conventional DJ stent with a flap valve. The basis for the flap valve was a 7F DJ stent (Percuflex™ Plus; Boston Scientific Corporation, Marlborough, MA). The detailed dimension was as follows: 26 cm in length, 2.3 mm in outer diameter, 1.3 mm in inner diameter, and 0.5 mm in tube wall thickness. The valve consisted of two liplike membranes and an inner cavity. The inner cavity had the function of both a fluidic channel and a pathway for insertion of a guidewire (Boston Scientific Corporation), which is an effective and safe method for achieving stent immobilization in the ureter.
(
The valve was made of Tango Plus FLX980 (tensile strength of 1.50 MPa, elongation at break of 218%, hardness 27 Shore A) 18,19 and was formed via a stereo deposition process in the 3D printer (Objet500 Connex printer; Stratasys Ltd., Minneapolis, MN) with a computer-aided design (CAD) model using SolidWorks software. The valve material possessed the important characteristics of flexibility, deformability, compactness, and good life span, which allowed the valve to function effectively with large deformation, and was a photosensitive polymer that passed from liquid to solid state under ultraviolet exposure during the stereo deposition process. Each layer deposited was of a thickness of 0.016 mm. It was able to assume complex shapes in a short production time and can be used in a number of devices at a time. To enhance the biocompatibility, a coating of parylene C of 1 μm thickness was applied on the top and bottom of the fabricated valve using low pressure chemical vapor deposition (PDS2010, Specialty Coating Systems, Inc. Indianapolis, IN).
The operation principle of the valve is shown in Figure 1b and 1c. When the forward pressure (P1) was greater than the backward pressure (P2) (empty bladder state), the pressure difference caused the valve to open, which might enable urine to flow in an anterograde direction from the renal pelvis to the urinary bladder in the human body. On the other hand, when P2 was greater than P1 (filled bladder state), the valve was closed and sealed, so that retrograde urine flow might be prevented.
The in vitro setup for evaluating the flow characteristics is shown in Figure 2. First, two types of whole stent were prepared—the UCV stent and the PCV stent. For each stent, one side (opposite side of the valve) of the stent was connected to a three-way cock, as shown in Figure 2a. The valve was then dipped in deionized (DI) water in a closed petri dish to maintain the hydrophilic environment around the stent and to eliminate external air turbulence and evaporation. Subsequently, hydrostatic pressure (P), measured using a commercial pressure transducer (ADT 672, Additel Corporation, Yorba Linda, CA), was applied to the stent on the opposite side of the valve. It should be noted that the equation of hydrostatic pressure was defined as P=ρċgċh, where ρ was the density of the DI water, g was gravity, and h was the height of the DI water. Finally, the mass flow rate was recorded using an electronic balance (PRESTO Testing Instrument, PAG214) whose resolution was 0.1 mg. This measurement was converted to volumetric flow rate. Every data point of the flow rate was obtained at 3-minute intervals for each applied pressure. The range of the applied forward pressure was from 5 cm H2O to 30 cm H2O (at 5 cm H2O intervals), which is high enough to cover the difference between the renal pelvis pressure and the intravesicle pressure (approximately 15–18 cm H2O). 6

In vitro setup to measure (
The backward flow rate was also measured by connecting the DI water-filled chamber between the three-way cock and the valve, as shown in Figure 2b. The valve was dipped into the DI water-filled chamber, and the opposite side of the valve was also dipped into DI water in a closed petri dish. Because the intravesicle pressure normally reaches 30 cm H2O during a twitch or 50 cm H2O on voiding, 6 the range of applied backward pressure was from 5 to 50 cm H2O, at 5 cm H2O intervals.
In addition, the distal portion (3 cm) including the valve was cut from each of the stents to exactly evaluate the function of the flap valve by eliminating side holes effect. The flow characteristics (forward and backward flow rate) of the distal portion were evaluated in the same manner.
Results
Table 1 shows the overall selection of specified dimensions of the polymeric valve with the CAD model using the SolidWorks software. These dimensions were determined considering the diameter of the 7F DJ stent for effective connection. Critical dimension and tolerance of the 3D printer were also reflected.

Figure 3 provides a photo image of the fabricated flap valve. The outer diameter and the height of the flap valve were 2.8 mm and 5.3 mm, respectively. The fabricated valve was bonded to the 7F DJ stent using biocompatible glue (Loctite 431), as shown in Figure 4a. Figure 4b shows that the guidewire can be easily inserted into the antireflux ureteral stent through the valve.
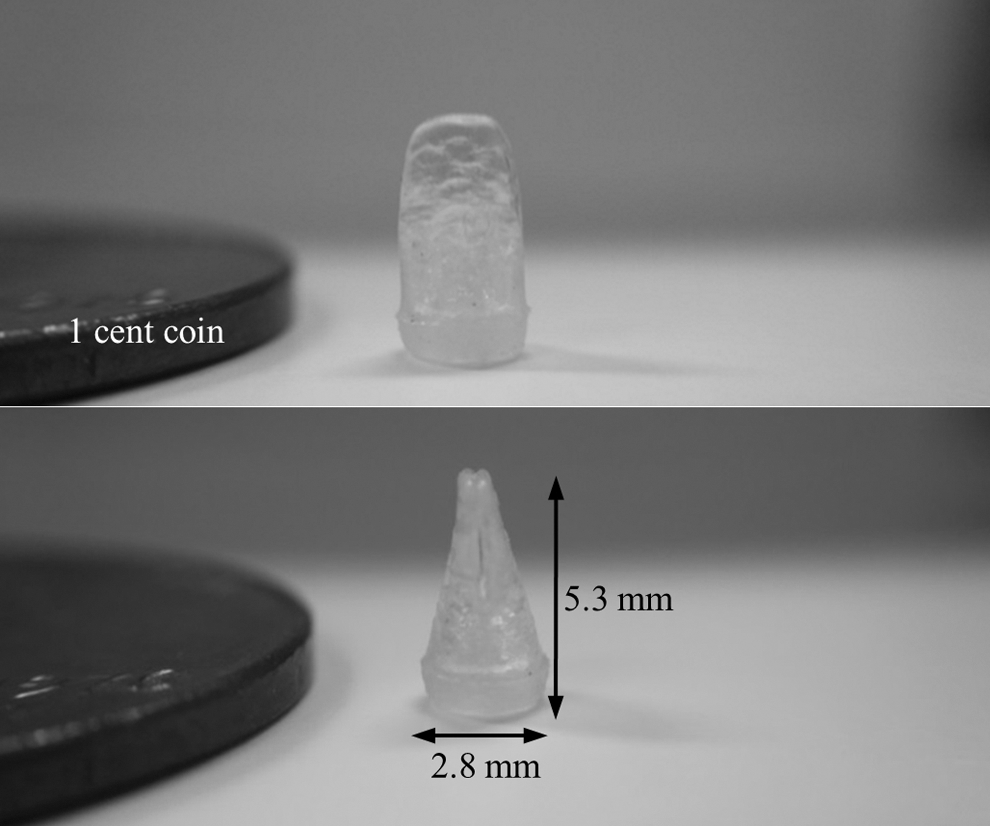
Photo images of the fabricated antireflux flap valve (side view and 90-degree-rotated one).
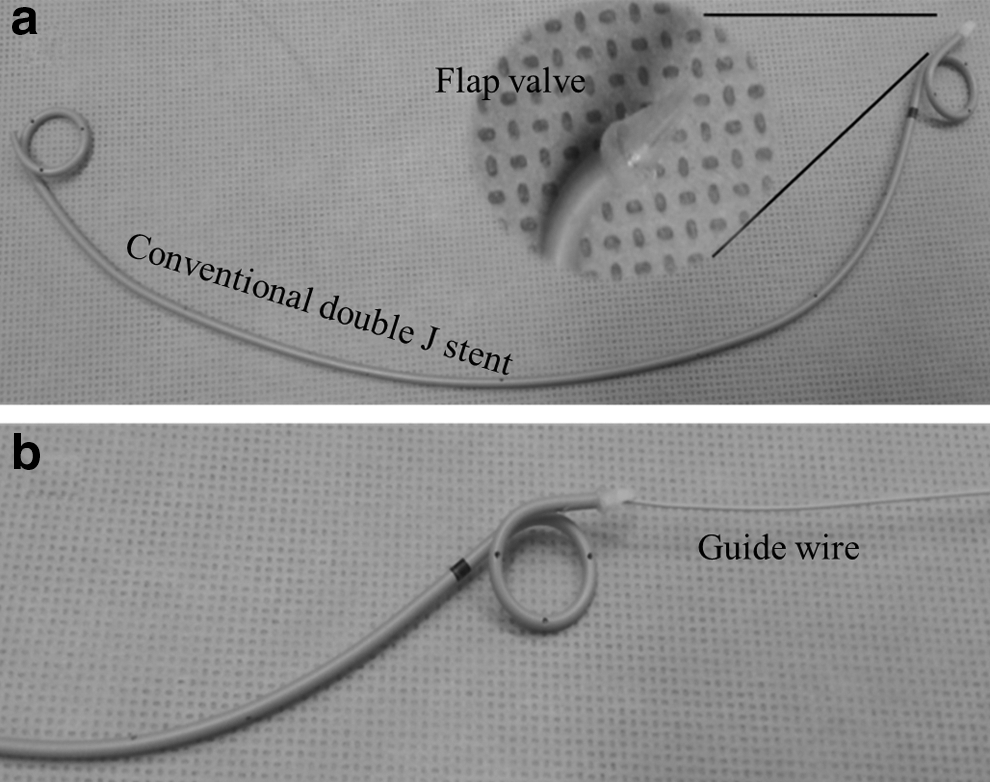
Photo images of the antireflux ureteral stent: (
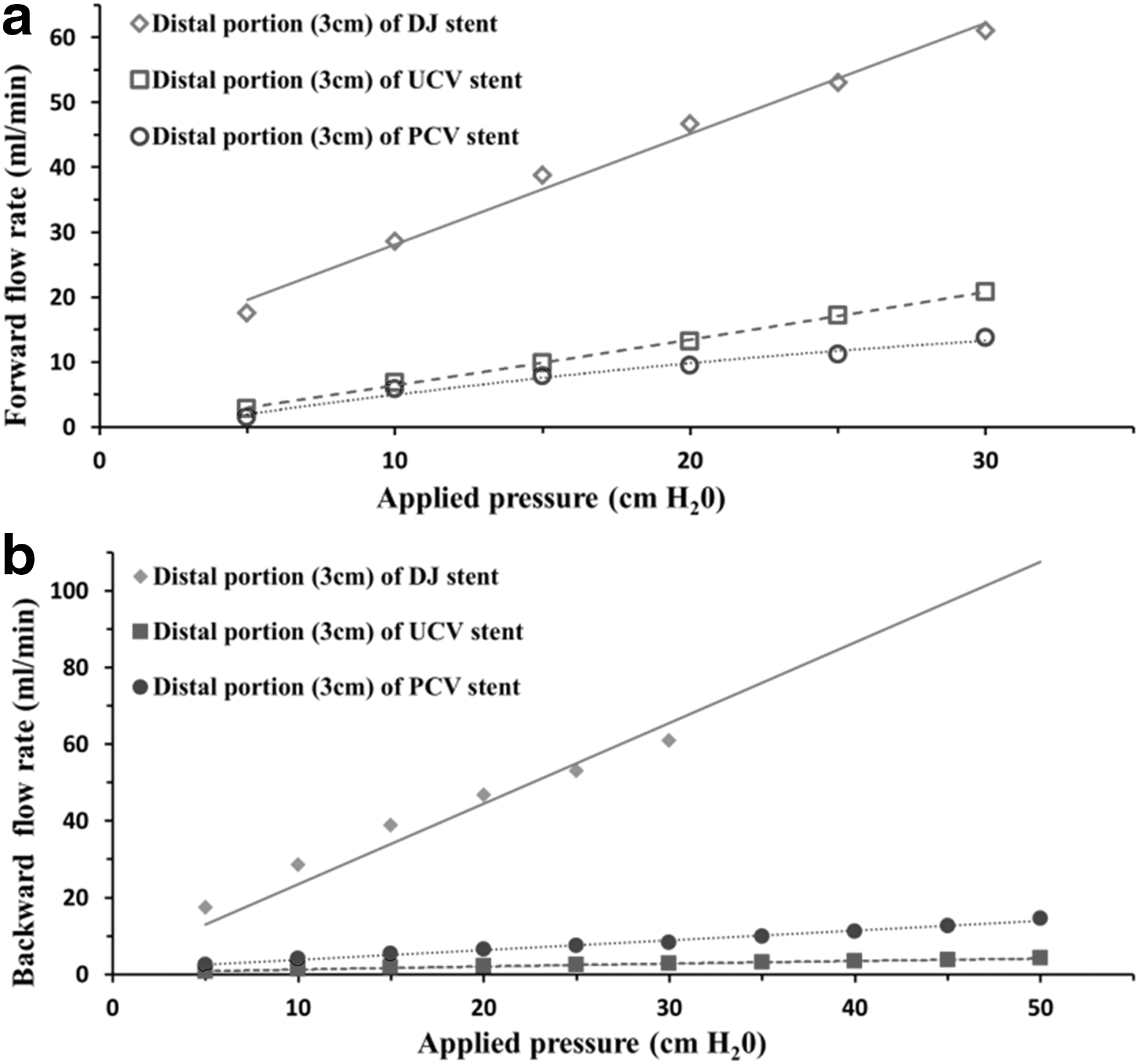
Figure 5 presents the experimental characteristics of the flap valves—the relationship between flow rate and the applied pressure for the distal portion (3 cm) of the DJ stents. The forward flow rates for the distal portion of the UCV and PCV stent were 9.8 mL/min and 7.8 mL/min at applied pressure of 15 cm H2O (normal anterograde pressure in patients with stents), respectively (Fig. 5a). The backward flow rates for the distal portion of the UCV and PCV stent were decreased by 28 times and 8 times at applied pressure of 50 cm H2O (maximum bladder pressure), respectively, compared with that for the distal portion only of the intact DJ stent (Fig. 5b).
In vitro test of (
Figure 6 shows the flow rates with respect to the applied pressure for the whole stents, which can be used for real clinical practice. The forward flow rates of the whole stents were 22.2 mL/min for the UCV stent and 20.0 mL/min for the PCV stent at applied pressure of 15 cm H2O (Fig. 6a). The backward flow rates of whole UCV and PCV stents were decreased by 8 times and 4 times at applied pressure of 50 cm H2O, respectively, compared with the intact DJ stent (Fig. 6b).
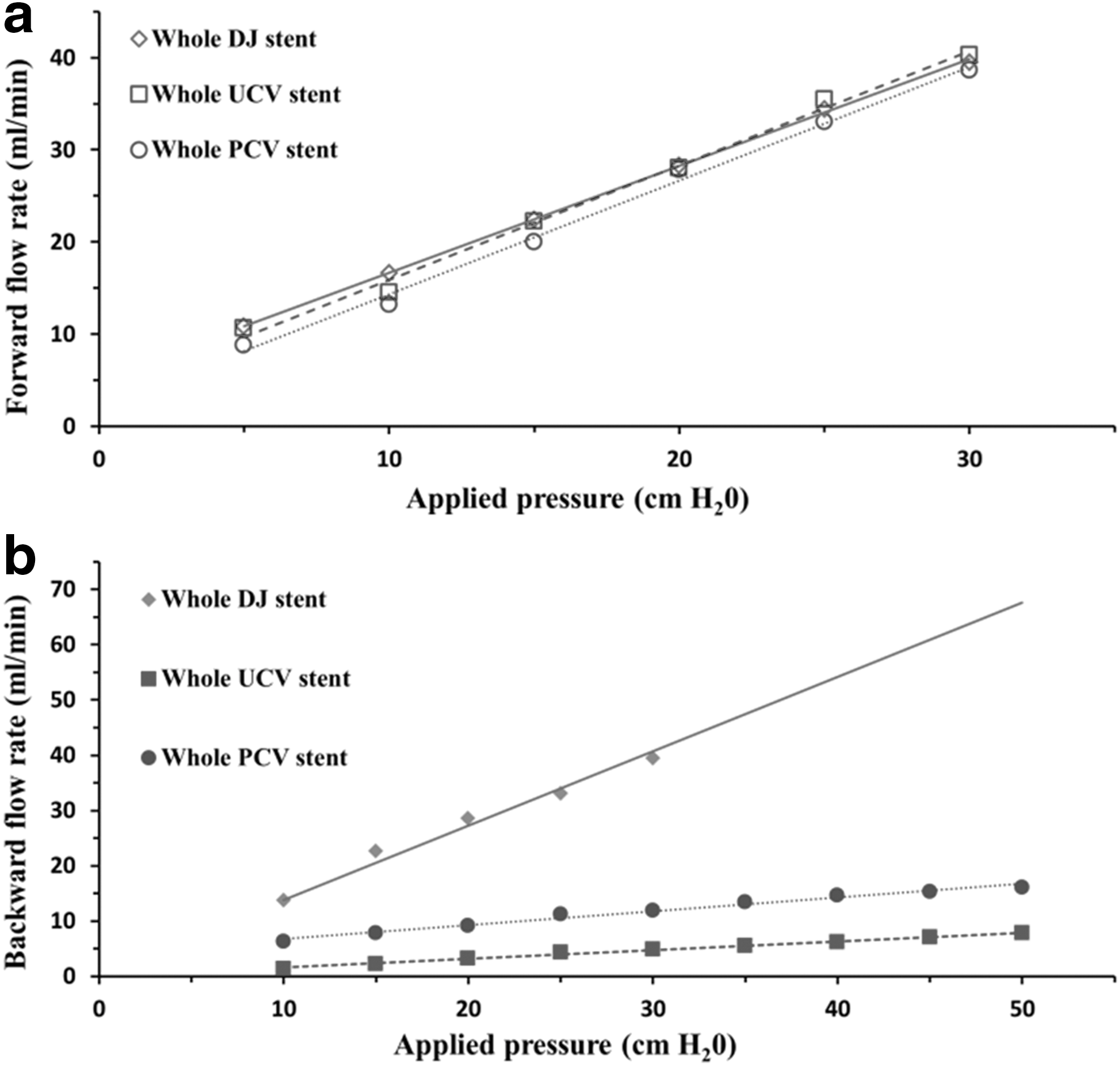
In vitro test of (
Discussion
The proposed antireflux ureteral stent was designed and fabricated to potentially reduce side effects such as flank pain and urinary tract infection that occur because of the retrograde urine flow caused by the conventional DJ stent. Several groups have previously developed antireflux ureteral stents to counteract these problems. 9,10 In 1992, Yamaguchi and associates 9 designed an antireflux ureteral stent by adding a thin silicon sleeve at its distal end, which acted as an antireflux valve. Ritter and colleagues 10 designed a different type of antireflex ureteral stent in 2012, which had a long, thin, and uncurled distal end. The distal end of this stent acted as an antireflux valve, and it was long enough to cross the midline of the bladder. These newly designed stents, however, are not yet widely used clinically.
For practical use of the antireflex ureteral stents clinically, maintaining the original form of the ureteral stent is thought to be important. If the design of the antireflex ureteral stents becomes larger or longer in any part because of variations, it may have side effects such as difficulties in stent insertion, more severe stent-related symptoms, and mucosal injuries of the lower urinary tract. 20,21 Therefore, miniaturizing the antireflux valve is important to maintain the original form of the ureteral stent as much as possible, which consequently may reduce the side effects. Because 3D printing enables easy fabrication of miniaturized structures, high precision, mass production, rapid prototyping, and cost-effectiveness, antireflex ureteral stents with the flap valve can be effectively fabricated with minimal changes to the original form of the ureteral stent.
The flap valve was made of Tango Plus, which is a rubber-like material that has high elasticity, 18 and therefore the stent has a high potential to return to its initial shape. Experiments on guidewire insertion into the antireflux stent through the UCV and PCV were performed three times to test its durability; any scratches or shape deformation on the valve were not noticeable, and therefore functional degradations are not expected in clinical use.
Parylene C, which is a bioinert and nontoxic material to tissue, is qualified as a Class VI polymer by the Food and Drug Administration. 22 Furthermore, the parylene C, which is coated on the antireflux valve (Tango Plus) in this study, 17 is being widely used in the encapsulation of implantable medical devices, and its biocompatibility to the bladder wall has been confirmed by many researchers. 23 Only parylene C matters in the sterilization of the proposed flap valves, because the antireflux valve (Tango Plus) was coated with parylene C film. It has been reported that parylene C does not change the chemical and crystalline properties when exposed to H2O2-plasma whereas gamma radiation decreases the crystallinity and ethylene oxide changes Cl-nature. 24 The increased stiffness, however, caused by the addition of parylene C coating might slightly inhibit the flap valve motion, specifically degrading the reduction of a backward flow both for the distal portion of stents and whole stents.
The anterograde flow rate of the urine in the ureter is approximately 0.5 mL/min when the pressure difference between the renal pelvis and the bladder is usually 15 to 18 cm H2O in patients with stents. Therefore, the forward flow rates of whole UCV (22.2 mL/min) and PCV (20.0 mL/min) stents are potentially able to cover the anterograde flow rate. The backward flow rate of whole UCV and PCV stents was decreased by a maximum 8.3 times and 4.0 times at applied pressure of 50 cm H2O (bladder pressure could be reached to the 50 cm H2O), respectively, compared with that of the intact DJ stent. These results imply that the proposed stent could potentially eliminate unwanted VUR. It is noteworthy that different stent sizes are associated with different flows, and any difference associated with use of the flap valve may be exaggerated or diminished with the use of the different stent sizes. 25 The experimental methods and flow characteristics of the proposed flap valve can be, however, extended to the evaluation of other stents of different sizes.
In view of clinical use, there might also be a concern that urinary reflux may occur through the extraluminal space (space between the stent and ureter) of the stent. We assume that at least the severity of VUR will be downgraded by significant reduction of the intraluminal urinary reflux, which may ultimately reduce the possibility of long-term sequelae of VUR. In vivo studies estimating VUR occurrence and severity in the proposed antireflux ureteral stent compared with conventional DJ stents are necessary to confirm our assumption. A reflux-preventing ureteral stent developed in 1992 had a similar design to the proposed stent and suggested similar extraluminal reflux-related problems. It had an antireflux device at the distal end of the stent, and showed a significant decrease in VUR compared with the conventional DJ stent in an actual patient. 9
The proposed antireflux ureteral stent is expected to have advantages in patients who need long-term placement of ureteral stents. These patients may probably be affected by repeated VUR in the presence of a conventional DJ stent. The proposed stent may also reduce the negative effects observed in short-term stent placement; patients will more likely be free from micturition-caused flank pain and acute pyelonephritis from transient VUR compared with those with conventional DJ stents inserted. Clinical studies should be conducted in the near future to validate the proper function of the proposed stent: Sterility, durability, encrustation, and any other damages in an animal model (e.g., porcine model), ex vivo animal urinary tract, cadaver, or other more biological model.
Conclusion
An antireflux ureteral stent with polymeric flap valve was successfully designed and fabricated using a 3D printer. The in vitro test results showed that the proposed stent effectively prevented backward flow with minimal reduction in forward flow. These results indicate that the stent could potentially eliminate VUR while maintaining sufficient anterograde flow for smooth urination in the bladder. Further clinical studies will be conducted to assure the proper function and the safety of the proposed stent.
Footnotes
Acknowledgments
This work was supported by BioNano Health-Guard Research Center funded by the Ministry of Science, ICT & Future Planning (MSIP) of Korea as Global Frontier Project (Grant Number H-GUARD_ERND2013M3A6B2078957) and IMSE, GIST.
Disclosure Statement
No competing financial interests exist.