
Abstract
Background and Objectives:
Two-port laparoscopic radical cystectomy (LRC) using a multichannel platform through the umbilicus and one additional 10-mm in the right iliac fossa has been recently described. We compare the perioperative and early results of this technique with a cohort of patients simultaneously treated in our institution with four-port LRC and a 7 to 10 cm midline incision.
Materials and Methods:
A matched-pair study comparing perioperative outcomes, postoperative visual analog pain scale (VAPS), and morbidity of two-port (n=30) and four-port (n=30) LRC. Preoperative and perioperative data analyzed and compared included demographics, type of urinary diversion, operative time, blood loss, transfusion requirements, decrease in serum hemoglobin, operative complications, analgesic needs, length of stay, number of nodes removed, and other pathologic information. Complications in the first 3 months were evaluated according to the Clavien–Dindo classification.
Results:
There was no significant difference between the two groups regarding patient age, gender, body–mass index, American Society of Anesthesiologists (ASA) score, Charlson comorbidity index, tumor stage, percent of positive nodes, positive margin rate, number of nodes retrieved, proportion of neobladders, secondary carcinoma in situ, incidental prostate cancer, or need of systemic chemotherapy. Median operative time was 20 minutes higher in the two-port procedure, but this difference was not statistically significant (p=0.2). Estimated blood loss and differential hemoglobin change were lower in the two-port technique (each p=0.03), but no difference was detected regarding the intraoperative or postoperative transfusion rate. Length of hospital stay was also equivalent. Differences were not observed either in the number or severity of complications. VAPS at days 2, 3, and 5 was significantly lower for two-port LRC (p<0.01).
Conclusions:
Two-port LRC performed through an umbilical platform and an accessory 10-mm port seems technically equivalent to standard four-port LRC. Perioperative outcomes regarding hospital stay and complications are tantamount. Diminished blood loss and, especially, less postoperative pain favor the reduced-port approach in this complex urologic minimally invasive procedure.
Introduction
U
We must not lose the perspective that removing adequate number of nodes and achieving negative surgical margins are technical goals that cannot be sacrificed by minimally invasive approaches. However, laparoscopic radical cystectomy (LRC) has progressively gained grounds to open radical cystectomy due to reduced blood loss, lower transfusion rate, less analgesic requirements, quicker recovery, and less hospital stay, 4 –9 without impairing oncologic outcomes, 9,10 even in the older population. 11
Robot-assisted radical cystectomy (RARC) is the latest modality of minimally invasive radical cystectomy 10 and has proved feasible even with a totally intracorporeal neobladder diversion. 12 However, strictly speaking, comparative data between LRC and RARC are lacking. In regard to the open technique, RARC does not seem to compromise oncologic outcomes either, but still remains a morbid procedure. 12,13 It also comes with a significant learning curve and a discrete increase in operative time. 14 Of course, similar to LRC, it may bring earlier recovery in selected cases, but the cost of the procedure is severely increased. 15
The da Vinci surgical platform was not initially designed for single-port or a reduced number of port surgery, and the inherent difficulties of the technique imply a limitation to perform radical cystectomy laparoendoscopically. 16 In fact, robotic assistance usually needs six ports (three 8-mm robotic trocars, two 12-mm ports for assistance, and a 12-mm port for the camera) and a 5 to 7 cm midline subumbilical incision in males for specimen retrieval, thus limiting the benefits of the technique regarding indemnity of the abdominal wall and postoperative pain.
We have described a new variant of LRC with two ports (two-port LRC) through a multichannel reusable umbilical platform and an accessory 10-mm port in the right iliac fossa, followed by lymph node dissection and ileal loop or neobladder without the need of an additional skin incision. 17,18 In this study, we compare this reduced-port umbilical approach with the standard LRC performed in our institution using four ports and a 7 to 10 cm midline incision (four-port LRC). Comparison includes operative results, perioperative variables revealing outcomes and complications, and attempts to define potential benefits of one or the other technique in a practical setting.
Materials and Methods
Study population
Patients with the diagnosis of nonmetastatic muscle-invasive bladder cancer considered candidates for radical surgery were proposed LRC in our institution since January 2008. The multimodal rehabilitation (fast track) program was initiated on January 2011, aiming to reduce the surgical stress response and postoperative morbidity and also to accelerate early recovery and improve patient-reported outcome. The key components of this program are preoperative patient education and information, intraoperative-enhanced (minimally invasive surgery, standardized anesthetic) and postoperative-enhanced mobilization, early oral nutrition, and effective pain relief. No bowel preparation was used, the nasogastric tube was initially avoided, and fluid was early administered. All patients were informed that the number and size of ports would be kept to as minimal as possible, even though additional ports could be placed or incisions performed if necessary. Previous abdominal surgery for colorectal cancer and overtly advanced or metastatic bladder cancer were considered contraindications for laparoscopy.
Sixty-two patients received LRC from January 2011 to April 2014 and converted to open radical cystectomy in two cases. A modification of LRC using a reusable multichannel umbilical port with curved instruments and one accessory port (two-port LRC) was introduced in November 2011 and 30 cases were thus successfully intervened. Another 30 cases had been operated using standard LRC with four ports (four-port LRC). There was no randomization for a group or the other, and the technique was decided based on surgeon and patient preferences. Several surgeons with similar experience performed the procedures. Both techniques are later described in depth (Figs. 1 –3).
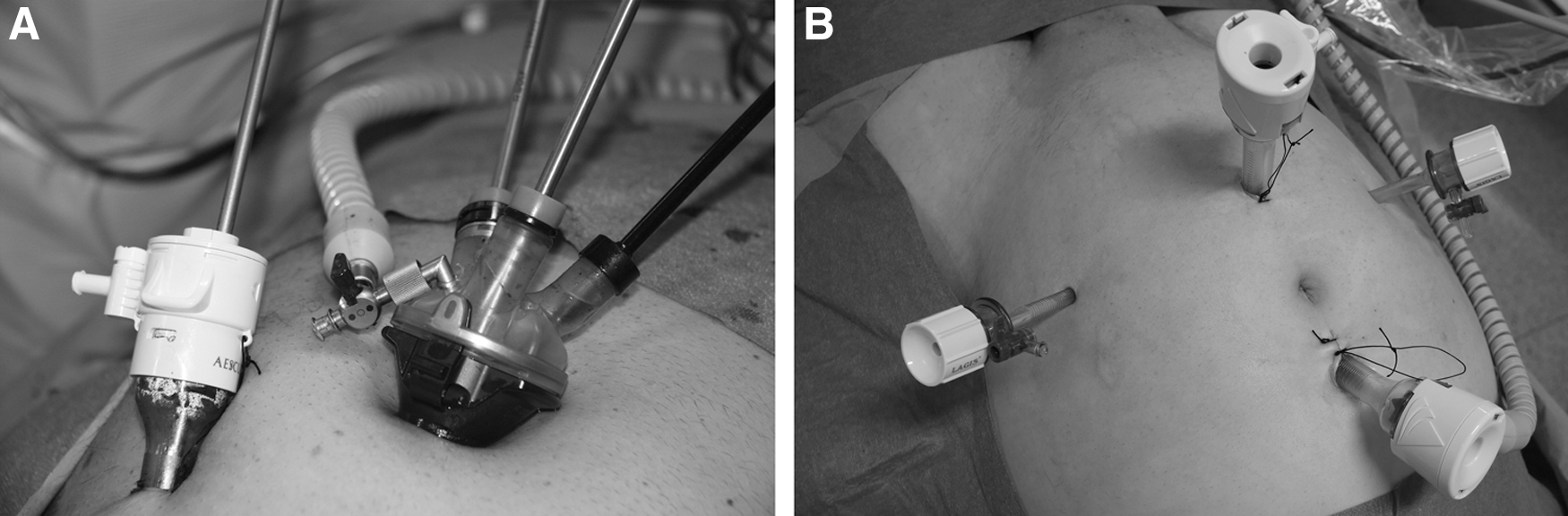
Port positioning.

Surgical wound.
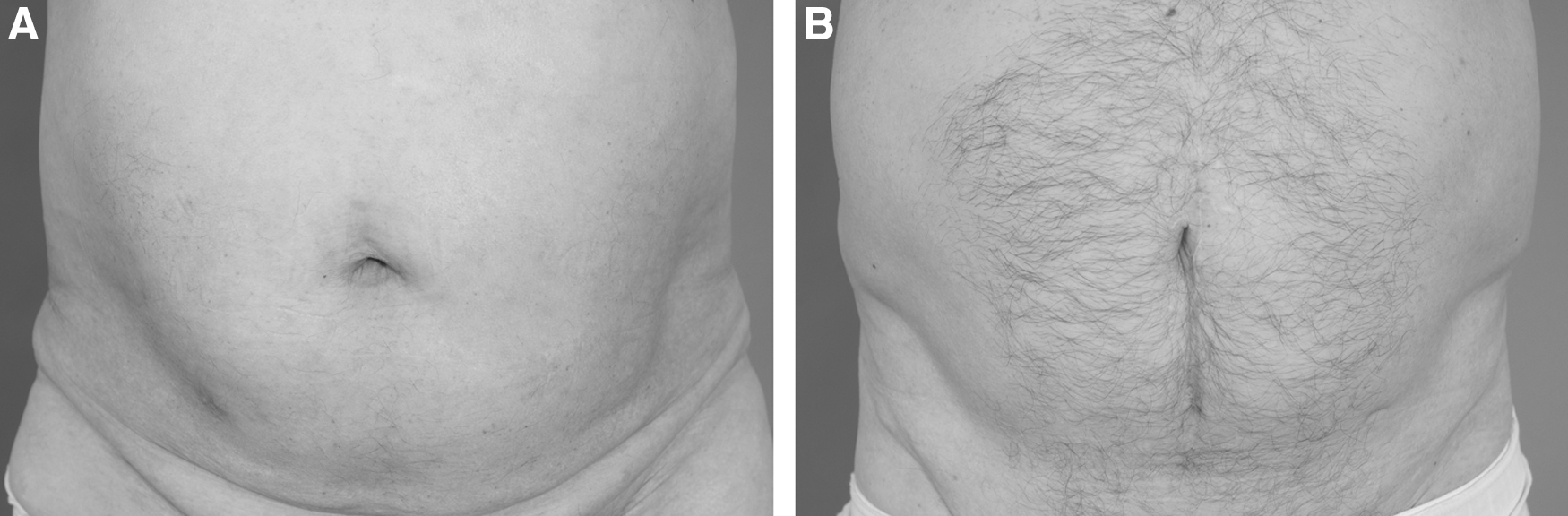
Residual surgical scar.
Data prospectively entered an institutional review board-approved database that included demographics, tumor characteristics, operative parameters, outcomes, and patient follow-up. Estimated blood loss; differential hemoglobin, calculated as postoperative day 2 minus preoperative day 14; operative time; conversion to standard laparoscopy; intraoperative complications; postoperative complications according to the Clavien–Dindo classification 19 ; hospital stay; and visual analog pain scale (VAPS) at days 1, 2, 3, and 5 were registered and compared.
Patients were discharged in the absence of complications after stool passage and with stable hemoglobin. In the initial 36 hours, all patients received epidural perfusion of bupivacaine (0.125%) and fentanyl (2 μcg/mL) plus an additional bolus of 3 mL on PCA, if required (3 bolus/hour maximum). Continuous intravenous (i.v.) metamizole sodium was used for the next 36 hours, later substituted by oral or i.v. narcotics as needed. Slow liquid intake started on day 2 and food intake on day 5; surgical drainage removed on day 4, ureteral stents on day 10, and the Foley catheter on day 14 under fluoroscopic control. All patients followed the same standards of postoperative care and criteria for analgesia, intake restoration, tube extraction, hospital discharge, adjuvant treatment, and follow-up. Patients with positive nodes or macroscopic fat infiltration received adjunct systemic chemotherapy.
Surgical technique
Two-port LRC
The patient was placed in the Trendelenburg position. KeyPort™ (Richard Wolf, Knittlingen, Germany), a reusable rigid trocar sized 2.5 cm at the tip and 3.5 cm at the base fitting a 2.5 cm umbilical opening, was inserted in a screw-driven manner. The inner element was removed and the soft multichannel cover with three openings (5-, 10-, and 15-mm, respectively) closed to insert curved instruments that incorporate the Duo-rotate™ system (Richard Wolf) and allow precise movements of the tips after alignment of the arms. A 5.3-mm-wide, 45-cm-long, 0° lens laparoscope and two operative curved instruments were used. The second surgeon used a 10-mm port placed in the right iliac fossa and held the lens inserted through the umbilical platform (Fig. 1A). This two-port technique facilitates proper working angle, avoids clashing of the laparoscope with the instruments, and also the accessory port serves to extract drainage and ureteral stents in the case of neobladder.
At the end of cystectomy and lymph node dissection, the specimen and umbilical port are extracted throughout the umbilicus. In females, vaginal delivery of the specimen is feasible. Placement of a disposable disc slightly extends the umbilical hole to facilitate exposure of ureters and bowel outside the navel to construct the neobladder extracorporeally. The umbilical port is reintroduced to perform the urethral anastomosis laparoendoscopically. Optionally, an ileal segment can be isolated, and separate Bricker anastomosis to the distal end of spatulated ureters performed extracorporeally. The ileal loop is then introduced and the stoma constructed at the site of the 10-mm port (Fig. 2A). Concrete technical aspects are described in detail in a previous publication. 18 Umbilical placement of the system hides the surgical scar inside the navel, giving the final appearance of a scar-free surgery, with or without stoma, depending on the diversion chosen (Fig. 3A).
Four-port LRC
LRC and pelvic lymphadenectomy performed with a four-port transperitoneal approach in a rhomboid manner. A 10/12-mm trocar was placed over the umbilicus to introduce a 0° lens, followed by a hypogastric 15-mm port under the umbilicus and two 5-mm ports on either iliac fossa lateral to the epigastric vessels halfway between the umbilicus and pubis (Fig. 1B). The technique essentially duplicates that of open cystectomy and includes a thorough pelvic lymphadenectomy. Upon completion of the cystectomy, the specimen was removed through a 7 to 10 cm midline infraumbilical incision that connects both midline ports and also used for extracorporeal construction of the urinary diversion (Fig. 2B). Bowel work and ureteroileal anastomosis are done extracorporeally both for an ileal conduit and an orthotopic neobladder, and the procedure ends with a cutaneous ileostomy or a reservoir placed again inside the abdominal cavity with midline incision closed and pneumoperitoneum restored. Laparoscopic urethro-neobladder anastomosis is performed around a Foley catheter and the procedure ends with the extraction of ureteral stents and drains through trocar incisions. This approach leaves a discrete midline scar (Fig. 3B).
Statistical analysis
Data regarding perioperative outcomes, complications occurring within the first 3 months of the procedure, measurements of convalescence, and histologic variables revealing outcomes in both study and control population are compared using the Cochran–Armitage tendency test for categorical variables and Mann–Whitney tests for continuous variables. Statistical analysis was performed using SAS 9.3 (SAS Institute, Inc., Cary, NC). Data are presented as the median and interquartile range between brackets.
Results
All patients were followed for at least 6 months. Median follow-up of the total series was 22.9 (10.6) months, 24.7 (9.7) months for patients intervened with two ports, and 21.1 (11.3) months for those treated with four ports (p=0.19). Demographic, clinical, and pathologic data revealed no significant differences between patients in each group in terms of age, gender, body–mass and Charlson comorbidity indexes, American Society of Anesthesiologists (ASA) score, tumor stage, positive surgical margins, incidental prostate cancer, presence of carcinoma in situ, number of positive nodes, or number of nodes removed. However, a tendency for a higher Charlson index appeared in the four-port group (Table 1).
ASA=American Society of Anesthesiologists; BMI=body–mass index; IQR=interquartile range; LRC=laparoscopic radical cystectomy.
One case in each group was converted to open radical cystectomy due to intraoperatively noticed highly advanced tumor stage, and these cases were excluded for the analysis of operative results and complications. No case in the two-port group was converted to conventional multiport laparoscopy. Median duration of surgery was slightly higher in two-port LRC, but this difference was not statistically significant (p=0.2). In addition, the proportion of neobladders was higher in this group, but did not reach statistical significance either (p=0.19). Median estimated blood loss was significantly lower in the two-port group [347.5 (100) vs 410 (250) mL; p=0.036] and so was median hemoglobin difference [−2 (1.8) vs−2.65 (1.5) g/dL; p=0.039]. The intraoperative transfusion rate was higher in the four-port group, but did not reach statistical significance (p=0.18). No difference was observed regarding postoperative transfusion (p=1). Median length of hospital stay was 1 day inferior in the two-port group, but did not reach statistical significance either (p=0.12). However, the proportion of patients discharged before postoperative day 8 was significantly superior in the reduced-port approach (36.7% vs 13.3%; p=0.037) (Table 2 and Fig. 4).

Days of hospital stay for two-port (up) and four-port (down) laparoscopic radical cystectomy (LRC). Differences are more noticeable in the proportion of patients discharged before postoperative day 8.
Statistically significant difference.
TPN=total parenteral nutrition; VAPS=visual analog pain scale.
No intraoperative complications occurred in either group, and the number and severity of postoperative complications were equivalent (Table 2). In the reduced-port group, 18 patients (60%) had no complications, 1 case (3.3%) had Clavien I complication (ileus), 8 (26.7%) had Clavien II complications (acute pyelonephritis, 2 cases; transfusion, 2 cases; fever due to infection of central venous catheter needing antibiotics, 1 case; ileus needing total parenteral nutrition [TPN], 3 cases, one with transfusion and another with pneumonia), 2 (6.6%) had Clavien III complications (acute limb ischemia due to embolic occlusion of external iliac artery treated with intra-arterial thrombolysis and percutaneous thrombectomy, 1 case; peritonitis due to progression of mixed urothelial and squamous-cell carcinoma needing colostomy, 1 case), and another patient (3.3%) had Clavien IV complication (septicemia needing intensive care unit stay, TPN, and transfusion).
In the standard four-port approach, 15 patients (50%) had no complications, 2 (6.6%) had Clavien I complication (pain needing extra analgesia, 2 cases), 10 (33.3%) had Clavien II complications (wound infection, 1 case; transfusion, 1 case; acute pyelonephritis, 2 cases, one with transfusion and another causing readmission; ileus needing TPN, 6 cases, 2 of them with transfusion), 1 (3.3%) had Clavien III complication (rectourethral fistula requiring colostomy), 1 (3.3%) had Clavien IV complication (upper digestive tract hemorrhage and pulmonary embolism requiring intensive care unit stay and transfusion), and another case (3.3%) had Clavien V complication (massive pulmonary embolism leading to death).
The proportion of patients with paralytic ileus needing TPN was lower in the two-port than four-port technique, but did not reach statistical significance (p=0.47), although median duration of ileus was statistically inferior in the reduced-port approach [5 (3) vs 8 (2) days; p=0.015] (Table 2 and Fig. 5). In addition, median VAPS was lower for the two-port technique analyzed every day, and differences were statistically significant on day 2 [2 (1) vs 3 (1) days; p=0.005], day 3 [1 (1) vs 3 (1) days; p<0.0001], and day 5 [1 (1) vs 2 (1) days; p=0.005].
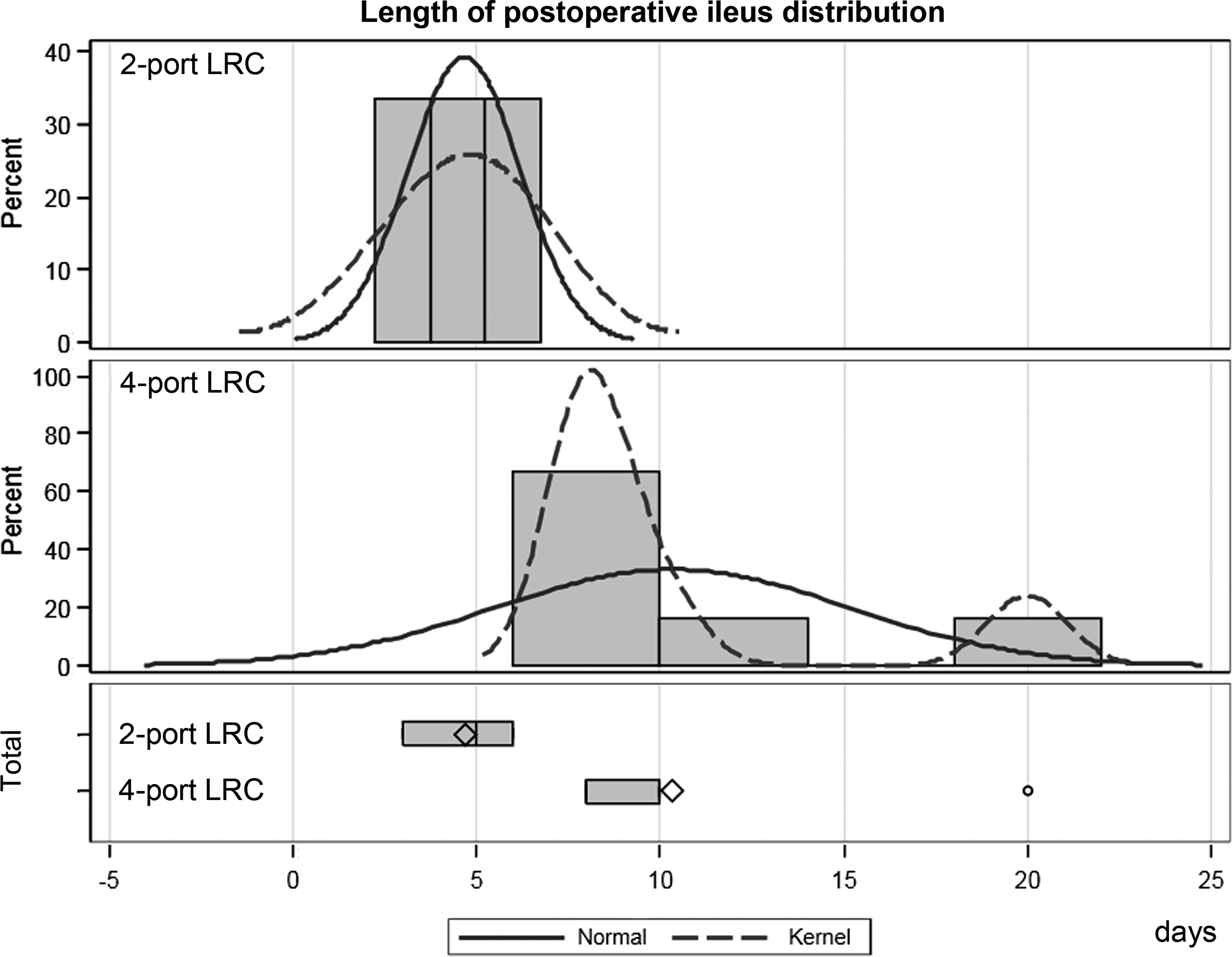
Days of postoperative ileus for two-port (up) and four-port (down) LRC.
A similar proportion of patients in each group received adjunct chemotherapy after surgery (Table 2). At the time of this report, nine patients (15%) of the total series had died of bladder cancer, four cases (13.3%) in the two-port group and five (16.7%) among those treated with four ports (p=1).
Discussion
Laparoendoscopic single-site surgery (LESS), with or without the application of robotic assistance, has become widely applicable for many different urologic procedures 20 and is slowly progressing in complex pelvic surgery. 21,22 However, the fact that radical cystectomy and urinary diversion imply a high number and severity of complications, often makes urologic surgeons reluctant to use a minimally invasive approach for this procedure. In this sense, LRC has possibly been the last oncologic surgery to demonstrate the advantages of laparoscopic approach in urology and some academic centers have been reluctant to favor its use. 23
However, apart from the complication rate of radical cystectomy, it is true that a cosmetic advantage is not a major issue for a disease with so high a mortality rate as high-grade bladder cancer. However, it is clearly demonstrated that laparoscopy allows over its open counterpart a prompt recovery, secondary to diminished blood loss and reduced postoperative pain. 4 –9 In our experience, a reduced-port approach for LRC also replicates the effect of reducing pain and blood loss, and this effect is sustained by objective data like the VAPS score and differential hemoglobin. The magnitude of effect in the VAPS score reduction that we reveal in this pilot study is small, but seems to be consistent. Reduction of number and size of ports may help, but avoidance of midline incision definitely consolidates the abdominal wall indemnity of the two-port approach. In as much, extraction of surgical specimen and performance of urinary diversion extracorporeal exclusively through the umbilicus sustain the earlier and less-painful recovery. Possibly a mean estimated blood loss difference of about 60 mL may be statistically but not clinically significant (mean hemoglobin difference 0.6 g/dL) and cause no change itself in transfusion risk. Similarly, reduction in blood loss might correspond to greater care at the time of surgery on line with the increased difficulty of the reduced-port approach that avoids minor bleeding in these cases.
What is undeniable is that the duration of ileus was lower in the two-port LRC and also that early hospital discharge was far more likely than in the four-port LRC. These data parallel minor invasiveness as can be expected through the avoidance of the 7 to 10 cm midline incision that is performed after completion of cystectomy in the four-port LRC.
Conclusion
Other experiences confirm that minimally invasive LRC and urinary diversion are feasible and safe for selected patients either through a single port, with or without an accessory 5-mm port, 21,24 –26 or through a single-incision laparoscopic surgery. 27 The two-port technique we have developed uses a reusable umbilical platform that is versatile, cost-effective, 17,18 and allows performance of the procedure through a minimally reduced incision. The advantages of single-site surgery based mainly on a reduced incision have already been demonstrated for different techniques regarding convalescence, postoperative use of analgesics, postoperative pain, and satisfaction with the scar. 28 –30 Of course, additional controlled studies are needed to determine if these modalities of reduced port number and caliber could be really advantageous over the conventional open-assisted multiport laparoscopic approach. Our experience with the two-port approach for LRC seems to be encouraging; although intestinal time is performed extracorporeally, it totally obviates the midline incision, as the two midline ports turn into an intraumbilical single one. We believe this concept of single multichannel platform plus satellite coaxial port facilitates LESS surgery and could even facilitate development of newer robotic technologies in the future.
Footnotes
Acknowledgments
The authors thank José Dominguez for photographic assistance and Juan Dorado (Pertica) for statistical analysis.
Author Disclosure Statement
No competing financial interests exist.